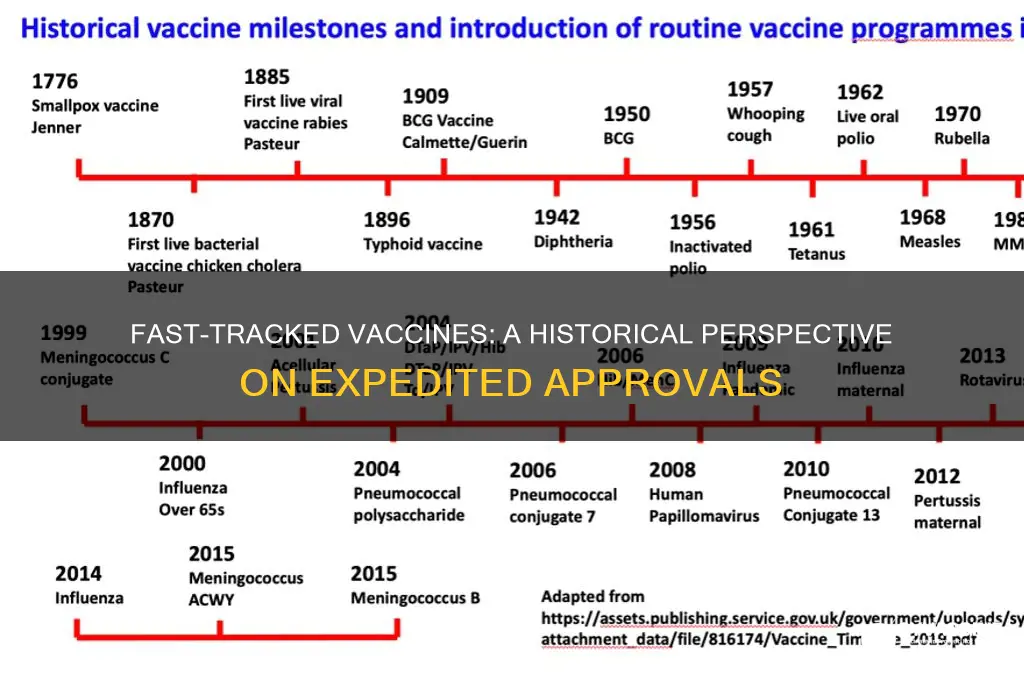
The rapid development and approval of COVID-19 vaccines have sparked discussions about the precedent of fast-tracking vaccines for other diseases. Historically, vaccine development has typically taken several years, if not decades, due to rigorous testing and regulatory processes. However, instances of accelerated timelines have occurred in response to urgent public health crises. For example, the Ebola vaccine (Ervebo) was fast-tracked during the 2014-2016 outbreak, receiving approval in less than five years. Similarly, the H1N1 influenza vaccine in 2009 was developed and distributed within months to combat a global pandemic. These examples demonstrate that while COVID-19 vaccines were unprecedented in their speed, the concept of expediting vaccine development is not entirely new, particularly when global health emergencies demand swift action.
| Characteristics | Values |
|---|---|
| Definition of Fast-Tracking | Accelerated approval processes by regulatory agencies like FDA, EMA, etc. |
| Historical Examples | Ebola, H1N1 (Swine Flu), Zika, Meningitis B vaccines. |
| Reasons for Fast-Tracking | Public health emergencies, pandemics, or urgent medical needs. |
| Regulatory Agencies Involved | FDA (U.S.), EMA (Europe), WHO, MHRA (UK), etc. |
| Safety and Efficacy Standards | Maintained despite accelerated timelines; post-approval monitoring required. |
| Funding and Collaboration | Government funding, public-private partnerships (e.g., CEPI, GAVI). |
| Timeline Comparison | Traditional vaccines: 10+ years; fast-tracked: 1-2 years (e.g., COVID-19). |
| Post-Approval Monitoring | Phase 4 trials, pharmacovigilance to ensure long-term safety. |
| Public Perception | Concerns about safety vs. necessity during emergencies. |
| Recent Examples (Pre-COVID) | Ebola vaccine (Ervebo) approved in 2019 after fast-tracking. |
| COVID-19 Context | Multiple vaccines (Pfizer, Moderna, AstraZeneca) fast-tracked in 2020-2021. |
| Global Access Initiatives | COVAX, ensuring equitable distribution of fast-tracked vaccines. |
Explore related products






What You'll Learn
- Historical Precedents: Past vaccines expedited for emergencies like Ebola, swine flu, and meningitis
- COVID-19 Comparison: How COVID-19 vaccine development speed differs from traditional timelines
- Safety Protocols: Rigorous testing and monitoring maintained despite accelerated approval processes
- Public Trust: Impact of fast-tracking on vaccine hesitancy and public confidence
- Regulatory Changes: Adaptations in approval processes by agencies like FDA and EMA
![]()
Historical Precedents: Past vaccines expedited for emergencies like Ebola, swine flu, and meningitis
The 2014 Ebola outbreak in West Africa highlighted the critical need for rapid vaccine development. In response, the rVSV-ZEBOV vaccine, developed by Merck, was fast-tracked through clinical trials and approved for use in 2019. This vaccine demonstrated 100% efficacy in a ring vaccination strategy, where close contacts of infected individuals were prioritized. Notably, the vaccine required only a single dose, administered intramuscularly, and was approved for individuals aged 18 and older. This precedent underscores the feasibility of accelerating vaccine development without compromising safety, provided robust international collaboration and adaptive trial designs are in place.
During the 2009 H1N1 swine flu pandemic, global health authorities expedited vaccine production to curb the rapidly spreading virus. Within six months of identifying the strain, vaccines were developed, manufactured, and distributed worldwide. These vaccines were administered in a single dose for adults and a two-dose regimen for children under 10, with a 21-day interval between doses. The swift response was facilitated by pre-existing pandemic preparedness plans and the use of established influenza vaccine platforms. However, the urgency led to logistical challenges, such as ensuring equitable distribution and addressing public hesitancy, which remain lessons for future fast-tracked vaccine efforts.
The 2015 meningitis outbreak in Niger demonstrated how existing vaccines could be repurposed and deployed rapidly in emergencies. The MenAfriVac vaccine, initially developed for serogroup A meningitis, was used off-label to control the outbreak. This vaccine, costing less than $0.50 per dose, was administered to individuals aged 1–29 in mass vaccination campaigns. The success of this response hinged on flexible regulatory frameworks that allowed for rapid deployment and the ability to scale up production quickly. This case illustrates how pre-existing vaccines can be a critical tool in emergency settings, provided regulatory and logistical barriers are minimized.
Comparing these examples reveals a common thread: successful fast-tracking relies on preparedness, flexibility, and collaboration. For instance, the Ebola vaccine’s single-dose regimen simplified administration, while the swine flu vaccine’s rapid production leveraged existing infrastructure. In contrast, the meningitis response highlighted the value of repurposing proven vaccines. For future emergencies, stakeholders should prioritize developing platform technologies, establishing global manufacturing agreements, and fostering public trust. Practical tips include pre-approving clinical trial protocols, securing funding for rapid scale-up, and ensuring clear communication strategies to address vaccine hesitancy. These historical precedents offer a roadmap for balancing speed and safety in vaccine development during crises.
Aborted Fetal Tissue in Vaccines: Which Ones and Why?
You may want to see also
Explore related products






![]()
COVID-19 Comparison: How COVID-19 vaccine development speed differs from traditional timelines
The COVID-19 vaccines were developed in record time, with some authorized for emergency use within a year of the pandemic’s onset. This unprecedented speed contrasts sharply with traditional vaccine development timelines, which typically span 10 to 15 years. For example, the mumps vaccine, developed in the 1960s, took four years from initial research to approval. The COVID-19 vaccines’ rapid progression raises questions about how this was achieved without compromising safety or efficacy.
To understand the difference, consider the stages of vaccine development. Traditionally, preclinical testing, clinical trials (Phases 1, 2, and 3), and regulatory approval occur sequentially, with each phase taking months or years. For COVID-19, these stages overlapped significantly. For instance, manufacturing began during clinical trials, a risky but strategic move that ensured doses were ready immediately upon approval. This parallel processing, combined with global collaboration and funding, shaved years off the timeline.
Critics often question whether fast-tracking compromises safety. However, COVID-19 vaccines underwent the same rigorous testing phases as any other vaccine. The difference lies in the scale and speed of trials. Moderna’s mRNA vaccine, for example, enrolled 30,000 participants in its Phase 3 trial, a larger-than-average cohort, and results were expedited due to high infection rates in trial locations. Regulatory agencies like the FDA reviewed data in real-time, further accelerating approval without bypassing safety checks.
Practical takeaways from this comparison are clear. First, the COVID-19 model demonstrates that vaccine development can be expedited during emergencies without sacrificing safety. Second, it highlights the importance of global cooperation and funding in achieving such feats. For future pandemics, policymakers should consider pre-emptive manufacturing and streamlined regulatory processes. Individuals can contribute by participating in clinical trials and staying informed about vaccine safety protocols.
Finally, while the COVID-19 vaccines’ rapid development is exceptional, it builds on decades of scientific advancements, such as mRNA technology. This innovation, pioneered in the 2010s, allowed researchers to quickly adapt the platform to target SARS-CoV-2. The pandemic served as a catalyst, proving that with sufficient resources and urgency, vaccine timelines can be dramatically shortened. This sets a precedent for addressing other global health challenges, from influenza to emerging diseases.
Tetanus Vaccine: Unique Features and Differences from Other Immunizations
You may want to see also
Explore related products






![]()
Safety Protocols: Rigorous testing and monitoring maintained despite accelerated approval processes
The COVID-19 pandemic spotlighted the concept of fast-tracked vaccines, but this approach isn’t new. Historically, vaccines like the Ebola vaccine (Ervebo) were expedited through emergency use authorizations, yet safety protocols remained non-negotiable. For Ervebo, Phase 3 trials involved over 16,000 participants, ensuring efficacy and safety before approval. This example underscores that acceleration doesn’t bypass rigor—it reorders it, prioritizing urgent needs without compromising standards.
Consider the steps involved in maintaining safety during accelerated approval. First, clinical trials are condensed but not abbreviated. For instance, the HPV vaccine Gardasil underwent Phase 3 trials with 24,000 participants, while fast-tracked COVID-19 vaccines enrolled over 40,000 each. Second, regulatory bodies like the FDA and EMA mandate real-world monitoring post-approval. The COVID-19 Vaccine Adverse Event Reporting System (VAERS) and V-safe tracked millions of doses, flagging rare side effects like myocarditis in young males (12.6 cases per million doses in 12-17-year-olds). These systems prove that speed doesn’t sacrifice scrutiny.
A persuasive argument for maintaining rigorous protocols lies in public trust. Fast-tracking without transparency erodes confidence. During the H1N1 pandemic, the 2009 vaccine was approved in four months but built on decades of influenza research. Similarly, mRNA technology, used in COVID-19 vaccines, had been studied for 20 years. By communicating this foundation, health authorities can reassure the public that accelerated timelines don’t equate to shortcuts. Practical tip: When discussing vaccines, emphasize the cumulative science behind them, not just the recent trials.
Comparatively, fast-tracked vaccines often leverage existing platforms, reducing unknowns. The Ebola vaccine used an adenovirus vector, a method tested in other vaccines. COVID-19 vaccines built on mRNA, a platform studied since the 1990s. This reuse of proven technologies allows for faster development while maintaining safety. For instance, the Moderna COVID-19 vaccine’s 30-microgram dose was optimized through prior research, balancing efficacy and side effects. This strategic reuse highlights how acceleration and safety can coexist.
In conclusion, fast-tracking vaccines isn’t about cutting corners—it’s about redefining timelines while upholding safety. From Ebola to COVID-19, accelerated approvals rely on robust trials, post-market surveillance, and proven technologies. For parents, healthcare workers, or policymakers, understanding this process is key. Practical takeaway: When evaluating fast-tracked vaccines, look for transparency in trial data, post-approval monitoring systems, and the scientific history behind the technology. Speed and safety aren’t mutually exclusive—they’re partners in protecting public health.
Congress Passes National Childhood Vaccine Injury Act: A Historical Overview
You may want to see also
Explore related products






![]()
Public Trust: Impact of fast-tracking on vaccine hesitancy and public confidence
Fast-tracking vaccines is not a new phenomenon, yet its application during the COVID-19 pandemic heightened public scrutiny like never before. Historically, vaccines such as the Ebola vaccine (Ervebo) were expedited through regulatory processes, receiving approval in record time. For instance, Ervebo was greenlit by the European Medicines Agency in less than a year, compared to the typical 10–15-year timeline. This precedent demonstrates that accelerated development and approval are feasible without compromising safety, but the COVID-19 vaccines’ unprecedented speed—some approved in under a year—sparked unique concerns. The question arises: how does this pace affect public trust, and what lessons can be drawn from past examples?
Consider the mechanics of fast-tracking. Regulatory agencies like the FDA and EMA employ mechanisms such as rolling reviews, where data is assessed as it becomes available, rather than in one final submission. This streamlines the process but can fuel misconceptions about corners being cut. For example, a 2021 survey revealed that 40% of unvaccinated individuals cited concerns about rushed development as a primary reason for hesitancy. To counter this, transparent communication is critical. Public health officials must emphasize that fast-tracking eliminates bureaucratic delays, not safety checks. Highlighting post-approval surveillance, such as the CDC’s v-safe program, which monitors vaccine side effects in real time, can reassure skeptics.
A comparative analysis of fast-tracked vaccines reveals a pattern: public confidence hinges on perceived transparency and inclusivity. The HPV vaccine, Gardasil, faced initial resistance due to its rapid approval and aggressive marketing, but trust grew as long-term safety data became available. Conversely, the COVID-19 vaccines’ rollout was marred by inconsistent messaging and political interference, amplifying distrust. Practical steps to rebuild confidence include involving community leaders in vaccine campaigns and providing clear, age-appropriate information. For instance, explaining to parents that the pediatric COVID-19 dose is one-third the adult amount (10 mcg vs. 30 mcg) can alleviate fears about safety in younger age groups.
Persuasively, the impact of fast-tracking on public trust is not inherent but contextual. When expedited processes are paired with robust communication and community engagement, they can enhance confidence. For example, Rwanda’s successful rollout of the Ebola vaccine in 2019 was bolstered by door-to-door education campaigns and local health worker involvement. In contrast, the rushed deployment of the Dengvaxia dengue vaccine in the Philippines, without adequate risk communication, led to widespread panic and mistrust. The takeaway is clear: speed must be balanced with sensitivity to public concerns. Policymakers should adopt a dual strategy—accelerate where necessary but invest equally in building trust through transparency and inclusivity.
Finally, a descriptive lens reveals the human element at the core of vaccine hesitancy. Fast-tracking, while scientifically justified, often clashes with the public’s need for reassurance. Stories of individuals who overcame skepticism, such as those who initially doubted the H1N1 vaccine in 2009 but later advocated for COVID-19 vaccination, underscore the power of personal experience and peer influence. Practical tips for addressing hesitancy include hosting town halls with healthcare providers, sharing testimonials from trusted figures, and leveraging social media to debunk myths. By framing fast-tracking as a tool for saving lives rather than a shortcut, public health efforts can bridge the gap between scientific urgency and societal acceptance.
Effective Tips to Soothe Sore Arm Pain After Vaccination
You may want to see also
Explore related products






![]()
Regulatory Changes: Adaptations in approval processes by agencies like FDA and EMA
The COVID-19 pandemic spotlighted the ability of regulatory agencies like the FDA and EMA to adapt approval processes for vaccines. Historically, vaccine development and approval spanned 10–15 years, but the Pfizer-BioNTech and Moderna COVID-19 vaccines received emergency use authorization (EUA) within 11 months. This unprecedented speed raises the question: how did regulatory agencies balance urgency with safety, and have such adaptations been applied to other vaccines?
One key adaptation was the use of rolling reviews, where regulators assessed data as it became available rather than waiting for complete trial results. This approach, also used for the Ebola vaccine Ervebo (approved in 2019), allowed the EMA and FDA to shave months off review timelines. For instance, the EMA’s rolling review of the AstraZeneca COVID-19 vaccine began in October 2020, enabling conditional marketing authorization by January 2021. This method is now being considered for vaccines targeting emerging pathogens like Zika and Lassa fever, where rapid response is critical.
Another significant change was the reliance on platform technologies, such as mRNA and viral vectors, which had been studied for years prior to the pandemic. The FDA’s prior research agreements (PRAs) with manufacturers like Moderna streamlined the approval process by establishing safety and efficacy benchmarks for these platforms. Similarly, the EMA’s Innovation Task Force provided early scientific advice to developers, reducing regulatory uncertainty. These frameworks are now being extended to vaccines for diseases like malaria, where BioNTech’s mRNA-based candidate is leveraging lessons from COVID-19 development.
However, fast-tracking is not without challenges. The FDA’s EUA pathway, while effective for COVID-19, requires post-authorization studies to confirm long-term safety and efficacy. For example, rare cases of thrombosis with thrombocytopenia syndrome (TTS) linked to the Johnson & Johnson vaccine were identified post-EUA, prompting updated guidelines. Regulators must balance expedited approvals with robust pharmacovigilance, ensuring that shortcuts in process do not compromise patient safety.
In practice, these adaptations are reshaping vaccine development globally. For instance, the Coalition for Epidemic Preparedness Innovations (CEPI) is using rolling reviews and platform technologies to accelerate vaccines for diseases like Nipah and MERS. Manufacturers are also investing in modular manufacturing facilities, capable of switching between vaccine types based on regulatory feedback. For policymakers and healthcare providers, understanding these changes is crucial for planning immunization campaigns and maintaining public trust in vaccine safety.
Ultimately, the regulatory adaptations seen during COVID-19 have set a new standard for vaccine approvals. While not all vaccines will—or should—be fast-tracked, the lessons learned have equipped agencies like the FDA and EMA with tools to respond swiftly to future threats. The challenge now lies in institutionalizing these innovations without sacrificing the rigor that ensures vaccines are both safe and effective.
California's Stance on Philosophical Vaccine Exemptions: What You Need to Know
You may want to see also
Frequently asked questions
Yes, several vaccines have been fast-tracked in the past, such as those for Ebola, H1N1 swine flu, and Zika, using expedited regulatory processes without compromising safety standards.
No, fast-tracking focuses on accelerating administrative and review processes, not skipping safety trials. All vaccines must still meet rigorous safety and efficacy standards before approval.
Historically, vaccine development has taken years, but advancements in technology and global collaboration have enabled faster development, as seen with COVID-19 vaccines.
Examples include the H1N1 influenza vaccine in 2009, Ebola vaccines in 2019, and Zika vaccine candidates, all of which were prioritized due to urgent public health needs.