The Janssen (Johnson & Johnson) COVID-19 vaccine has faced several recalls and restrictions since its initial rollout. In April 2021, the U.S. temporarily paused its use after rare cases of a severe blood clotting disorder, thrombosis with thrombocytopenia syndrome (TTS), were reported. While the pause was lifted, the FDA later restricted the vaccine’s use to specific populations, such as adults who cannot receive other vaccines or those who prefer the Janssen option. Additionally, in May 2022, the FDA limited its use to adults who cannot access other vaccines or who prefer it due to ongoing concerns about TTS. These actions reflect ongoing efforts to balance the vaccine’s benefits against its rare but serious risks.
| Characteristics | Values |
|---|---|
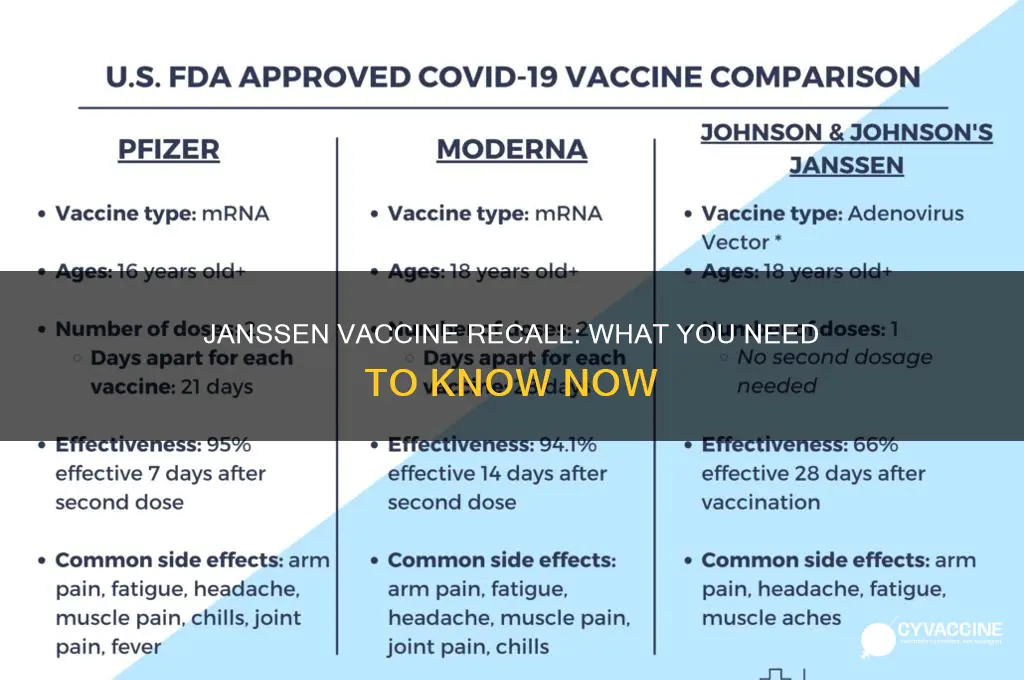
| Vaccine Name | Janssen (Johnson & Johnson) COVID-19 Vaccine |
| Recall Status (as of October 2023) | Not fully recalled; restricted use in the U.S. due to rare side effects |
| Reason for Restriction | Rare but serious blood clots (Thrombosis with Thrombocytopenia Syndrome, TTS) |
| Affected Population | Primarily adults under 50, though risk is very low across all ages |
| Current Use Guidelines | Recommended only for individuals who cannot receive Pfizer or Moderna, or prefer a single-dose vaccine |
| FDA and CDC Stance | Updated warnings and restrictions; not a complete recall |
| Global Status | Some countries continue unrestricted use; others follow U.S. guidance |
| Alternative Vaccines | Pfizer-BioNTech and Moderna mRNA vaccines recommended as primary options |
| Last Updated | October 2023 |
Explore related products






What You'll Learn
- FDA Pause and Investigation: Brief 2021 pause due to rare blood clots, thorough investigation followed
- Current Status: Janssen vaccine remains available with updated safety guidelines
- Rare Side Effects: Focus on thrombosis with thrombocytopenia syndrome (TTS) cases
- Alternative Vaccines: mRNA vaccines (Pfizer, Moderna) recommended over Janssen in many cases
- Global Usage: Some countries restricted or discontinued Janssen vaccine use post-review
![]()
FDA Pause and Investigation: Brief 2021 pause due to rare blood clots, thorough investigation followed
In April 2021, the U.S. Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) issued a joint statement recommending a pause in the use of the Janssen (Johnson & Johnson) COVID-19 vaccine. This decision was prompted by reports of a rare and severe type of blood clot, known as thrombosis with thrombocytopenia syndrome (TTS), in a small number of individuals who had received the vaccine. The pause was implemented out of an abundance of caution, allowing health authorities to investigate the cases thoroughly and assess the potential risks.
The investigation focused on six reported cases of TTS, all occurring in women between the ages of 18 and 48, within two weeks of vaccination. These cases were identified among approximately 6.8 million doses of the Janssen vaccine administered in the U.S. at the time. The rarity of the condition—estimated at roughly 7 per 1 million vaccinated women aged 18–49—highlighted the need for a careful risk-benefit analysis. The FDA and CDC convened an advisory committee meeting to review the data, ensuring transparency and scientific rigor in their decision-making process.
During the pause, healthcare providers were instructed to monitor for symptoms of TTS, which include severe headache, abdominal pain, leg pain, or shortness of breath, particularly if accompanied by easy bruising or tiny blood spots under the skin. Patients were advised to seek immediate medical attention if such symptoms arose within three weeks of receiving the Janssen vaccine. This proactive approach aimed to mitigate risks while the investigation proceeded.
Following a comprehensive review, the FDA and CDC lifted the pause after 10 days, reaffirming the vaccine’s safety and efficacy. They concluded that the benefits of the Janssen vaccine in preventing COVID-19 and its complications outweighed the potential risks of TTS. However, a warning about the rare risk of blood clots was added to the vaccine’s fact sheet, and healthcare providers were advised to discuss this risk with patients, particularly younger women. This episode underscored the robustness of the U.S. vaccine safety monitoring system, demonstrating its ability to swiftly identify and address rare adverse events.
For individuals considering the Janssen vaccine, it remains a viable single-dose option, especially for those who prefer a one-and-done approach or have limited access to multi-dose vaccines. However, awareness of the rare TTS risk is crucial. Patients should weigh this information against the significant protection the vaccine offers against severe COVID-19 outcomes, including hospitalization and death. As with any medical decision, consultation with a healthcare provider is recommended to determine the best vaccination strategy based on individual health needs and circumstances.
Vaccines and Kids: Debunking the Myth of Post-Shot Shedding
You may want to see also
Explore related products






![]()
Current Status: Janssen vaccine remains available with updated safety guidelines
The Janssen COVID-19 vaccine, developed by Johnson & Johnson, has not been universally recalled but remains available under specific conditions. Its status reflects a nuanced approach to balancing public health needs with safety concerns. Unlike mRNA vaccines, Janssen’s single-dose adenovirus-based formula offered logistical advantages, particularly in hard-to-reach populations. However, rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), prompted regulatory adjustments rather than a blanket withdrawal. This decision underscores the vaccine’s continued role in global immunization efforts, albeit with stricter guidelines.
From an analytical perspective, the Janssen vaccine’s availability hinges on targeted risk mitigation. The U.S. Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA) updated recommendations in 2022, advising its use primarily for individuals aged 18 and older who cannot access other vaccines or prefer a single-dose option. This shift acknowledges the vaccine’s benefits while addressing TTS risks, which occur at a rate of approximately 7 per 1 million doses in women aged 18–49. For men and older adults, the risk is significantly lower, making Janssen a viable choice in these demographics.
Practically, healthcare providers must now screen patients for contraindications before administering the Janssen vaccine. This includes inquiring about a history of blood clots or low platelets, as these conditions increase TTS susceptibility. If Janssen is the only available vaccine, providers should educate patients about TTS symptoms, such as severe headache, abdominal pain, or bruising beyond the injection site, which typically appear 1–2 weeks post-vaccination. Prompt medical attention is critical if these symptoms arise, as early treatment improves outcomes.
Comparatively, the Janssen vaccine’s updated guidelines contrast with the broader availability of mRNA vaccines like Pfizer-BioNTech and Moderna. While mRNA vaccines dominate due to their higher efficacy and lower risk profiles, Janssen fills a niche for vaccine-hesitant individuals or those in regions with limited refrigeration capabilities. Its single-dose regimen also simplifies vaccination campaigns in underserved areas. This comparative advantage ensures its continued relevance, despite safety concerns.
In conclusion, the Janssen vaccine’s current status exemplifies adaptive public health policy. By restricting its use to specific populations and enhancing safety protocols, regulators preserve its utility while minimizing risks. For individuals and providers, understanding these guidelines is essential to making informed decisions. The vaccine remains a tool in the fight against COVID-19, but its deployment now requires careful consideration of both benefits and potential harms.
Faith, Fear, and Freedom: Why Some Christians Oppose Vaccines
You may want to see also
Explore related products


![]()
Rare Side Effects: Focus on thrombosis with thrombocytopenia syndrome (TTS) cases
The Janssen (Johnson & Johnson) COVID-19 vaccine, a single-dose viral vector vaccine, has been under scrutiny due to its association with a rare but serious side effect: thrombosis with thrombocytopenia syndrome (TTS). This condition, characterized by blood clots in combination with low platelet counts, has raised concerns among healthcare providers and the public alike. While the vaccine has not been fully recalled, its distribution and use have been significantly restricted in many regions, particularly for specific age groups and populations.
TTS typically occurs within 1 to 2 weeks after receiving the Janssen vaccine, with symptoms including severe headache, abdominal pain, leg pain, or shortness of breath. The risk of developing TTS is estimated at approximately 7 per 1 million vaccinated women aged 18–49, and 2 per 1 million vaccinated women aged 50–64. For men, the risk is lower but still present, with about 2 cases per 1 million vaccinated individuals. These statistics highlight the rarity of the condition but underscore the importance of awareness and prompt medical attention if symptoms arise.
Healthcare providers are advised to consider TTS in patients presenting with thrombosis or thrombocytopenia following Janssen vaccination, particularly if symptoms emerge within 3 weeks of receiving the dose. Treatment for TTS differs from typical blood clot management; heparin, a common anticoagulant, should be avoided due to the risk of exacerbating thrombocytopenia. Instead, non-heparin anticoagulants and intravenous immune globulin (IVIG) are recommended. Patients should also be monitored closely for complications such as stroke or organ damage.
For individuals who have received the Janssen vaccine, it’s crucial to remain vigilant for potential TTS symptoms. If severe headache, persistent abdominal pain, leg swelling, or unusual bruising occur, immediate medical evaluation is necessary. While the overall risk remains low, early detection and appropriate treatment can significantly improve outcomes. Public health agencies continue to monitor TTS cases, balancing the vaccine’s benefits against its risks, particularly in regions with high COVID-19 transmission where the vaccine’s single-dose convenience remains advantageous.
In response to TTS concerns, many countries have adjusted their vaccination strategies. For instance, the U.S. Centers for Disease Control and Prevention (CDC) now recommends mRNA vaccines (Pfizer-BioNTech or Moderna) over the Janssen vaccine for primary and booster doses, especially for younger individuals. However, the Janssen vaccine may still be considered for those with mRNA vaccine contraindications or in settings where a single-dose option is preferred. This nuanced approach reflects the ongoing effort to maximize vaccine safety while addressing global health needs.
Weekly Global Vaccine Rollout: Tracking Administration Rates and Progress
You may want to see also
![]()
Alternative Vaccines: mRNA vaccines (Pfizer, Moderna) recommended over Janssen in many cases
The Janssen (Johnson & Johnson) vaccine, a one-dose viral vector option, faced scrutiny due to rare but serious blood clotting events, prompting its recall in some regions and restricted use in others. This has shifted focus to mRNA vaccines like Pfizer and Moderna, which are now preferred in many cases. These vaccines, requiring two doses (three for immunocompromised individuals), have demonstrated higher efficacy rates and a safer side effect profile, particularly in preventing severe COVID-19 outcomes.
For individuals aged 12 and older, Pfizer’s mRNA vaccine is administered in two 30-microgram doses, spaced 3–8 weeks apart, while Moderna offers a 100-microgram dose for adults 18 and older, with a 4–8 week interval. Both vaccines have been authorized for booster shots, with Pfizer approved for ages 5 and up and Moderna for 18 and older. The mRNA technology, which instructs cells to produce a harmless protein triggering an immune response, has proven both effective and adaptable, with updated formulations targeting emerging variants.
When comparing the two, Pfizer’s lower dosage and broader age approval make it a versatile choice, particularly for adolescents and younger adults. Moderna’s higher dosage may offer slightly stronger immunity in some studies, though both vaccines provide robust protection against hospitalization and death. For those with a history of blood disorders or who prefer a two-dose regimen, mRNA vaccines are the clear recommendation over Janssen.
Practical tips for recipients include scheduling doses well in advance to ensure timely administration and monitoring for side effects like fatigue, headache, or fever, which are typically mild and short-lived. Staying hydrated and resting post-vaccination can alleviate discomfort. For those hesitant about mRNA vaccines, understanding their rigorous testing and real-world success may ease concerns, as billions of doses have been administered globally with minimal serious adverse events.
In summary, the shift from Janssen to mRNA vaccines reflects a prioritization of safety and efficacy in public health strategies. Pfizer and Moderna’s mRNA vaccines, with their proven track record and adaptability, are now the cornerstone of COVID-19 prevention efforts, offering reliable protection across diverse populations.
Understanding Feline FVRC-P: Decoding Your Cat's First Vaccine
You may want to see also
![]()
Global Usage: Some countries restricted or discontinued Janssen vaccine use post-review
The Janssen COVID-19 vaccine, a single-dose viral vector-based option, faced varying levels of scrutiny and regulatory action across the globe following post-authorization reviews. While not universally recalled, its usage was notably restricted or discontinued in several countries due to safety concerns, particularly regarding rare but serious side effects such as thrombosis with thrombocytopenia syndrome (TTS). This clotting disorder, though uncommon (occurring in approximately 7 per 1 million vaccinated women aged 18–49), prompted health authorities to reevaluate the vaccine’s risk-benefit profile, especially in regions with alternative vaccine options.
Analyzing the global response reveals a pattern of cautious decision-making. For instance, the United States initially paused Janssen’s distribution in April 2021 to investigate TTS cases, resuming it with updated guidelines, including a warning for women under 50. In contrast, South Africa, which relied heavily on the Janssen vaccine due to its single-dose convenience and efficacy against the Beta variant, maintained its use but implemented stricter monitoring protocols. Conversely, European countries like Denmark and Austria discontinued its use entirely, prioritizing mRNA vaccines with lower TTS risks. These divergent approaches highlight the interplay between local healthcare infrastructure, variant prevalence, and public health priorities.
Instructively, countries that restricted Janssen’s use often did so based on age and gender stratification. For example, Australia limited its administration to individuals over 60, while Canada recommended it only for those who could not access mRNA vaccines or had a contraindication to them. Such targeted restrictions aimed to maximize benefits while minimizing risks, particularly for younger populations more susceptible to TTS. Practical tips for healthcare providers included ensuring informed consent, discussing alternative vaccines, and monitoring recipients for symptoms like severe headache or abdominal pain within three weeks post-vaccination.
Persuasively, the Janssen vaccine’s global restrictions underscore the importance of context-specific decision-making in public health. While its single-dose regimen offered logistical advantages in low-resource settings, the availability of safer alternatives in wealthier nations rendered its risks less acceptable. This dichotomy raises questions about equitable access to vaccines and the ethical implications of exporting products deemed suboptimal for domestic use. For instance, African countries, which received significant Janssen doses through COVAX, faced the challenge of balancing immediate vaccination needs with long-term safety concerns.
Comparatively, the Janssen vaccine’s trajectory contrasts with that of mRNA vaccines, which faced fewer post-authorization restrictions despite their own rare side effects, such as myocarditis. This disparity reflects not only the vaccines’ safety profiles but also the influence of public perception and regulatory frameworks. While mRNA vaccines benefited from robust clinical trial data and early adoption in high-income countries, Janssen’s viral vector technology faced greater scrutiny due to its association with TTS. This comparison highlights the need for transparent communication and adaptive regulatory strategies in vaccine deployment.
Descriptively, the Janssen vaccine’s restricted use paints a picture of a global health landscape navigating trade-offs between speed, safety, and accessibility. Its single 0.5 mL dose, administered intramuscularly, offered a practical solution for mass vaccination campaigns, particularly in regions with limited storage capacity. However, the emergence of TTS cases led to a recalibration of its role, with some countries relegating it to a niche option for specific populations. This evolution reflects the dynamic nature of vaccine policy, shaped by emerging data, local contexts, and evolving public health goals.
Pet Vaccines for Child Safety: Essential Shots for Foster Homes
You may want to see also
Frequently asked questions
No, the Janssen vaccine has not been fully recalled. However, its use has been limited in the United States due to rare but serious risks of blood clots with low platelets (TTS). It is now recommended primarily for individuals who cannot receive other vaccines or in situations where other vaccines are unavailable.
The Janssen vaccine was restricted due to a rare side effect called Thrombosis with Thrombocytopenia Syndrome (TTS), which involves blood clots combined with low platelets. The CDC and FDA determined that the risks of TTS outweighed the benefits for most individuals, especially when safer alternatives like mRNA vaccines (Pfizer and Moderna) are available.
Yes, the Janssen vaccine is still available in the U.S., but its use is limited. It may be offered to individuals aged 18 and older who cannot receive other vaccines, have had a severe reaction to an mRNA vaccine, or prefer the Janssen vaccine after being informed of the risks. Consult your healthcare provider to discuss the best option for your situation.