As of October 2023, the United States has several approved and widely available vaccines for COVID-19, developed by pharmaceutical companies such as Pfizer-BioNTech, Moderna, and Novavax. These vaccines have undergone rigorous testing and have been authorized by the U.S. Food and Drug Administration (FDA) for emergency use or full approval, depending on the specific vaccine and age group. The vaccination campaign in the U.S. has been ongoing since December 2020, with millions of doses administered to protect individuals from severe illness, hospitalization, and death caused by the coronavirus. Booster shots have also been recommended to maintain immunity and address emerging variants, ensuring continued protection for the population.
| Characteristics | Values |
|---|---|
| Vaccine Availability | Yes, the U.S. has multiple FDA-approved and authorized COVID-19 vaccines. |
| Approved Vaccines | Pfizer-BioNTech, Moderna (both mRNA vaccines), Johnson & Johnson (viral vector vaccine). |
| Booster Shots | Available for eligible individuals, including updated bivalent boosters targeting Omicron subvariants. |
| Vaccine Distribution | Widely available through pharmacies, healthcare providers, and community clinics. |
| Vaccination Rate (as of Oct 2023) | Approximately 68% of the U.S. population fully vaccinated. |
| Age Eligibility | Vaccines available for individuals aged 6 months and older. |
| Cost | Free for all individuals, regardless of insurance or immigration status. |
| Efficacy | High efficacy against severe illness, hospitalization, and death; reduced protection against infection over time, especially with variants. |
| Side Effects | Mild to moderate (e.g., soreness, fatigue, fever); rare severe reactions (e.g., anaphylaxis, myocarditis). |
| Vaccine Mandates | Some states, employers, and institutions have mandates, but federal mandates vary by sector. |
| Global Contribution | The U.S. has donated over 600 million vaccine doses globally through initiatives like COVAX. |
Explore related products


$2.96 $24.95




What You'll Learn
- Vaccine Development Timeline: Key milestones in creating COVID-19 vaccines in the United States
- Approved Vaccines: List of FDA-approved or authorized COVID-19 vaccines in the U.S
- Vaccine Distribution: How COVID-19 vaccines are allocated and distributed across the U.S
- Vaccine Efficacy: Effectiveness of U.S.-approved COVID-19 vaccines against variants and symptoms
- Vaccine Mandates: Federal and state policies on COVID-19 vaccine requirements in the U.S
![]()
Vaccine Development Timeline: Key milestones in creating COVID-19 vaccines in the United States
The United States has not only developed but also distributed multiple COVID-19 vaccines at an unprecedented pace, thanks to a combination of scientific innovation, public-private partnerships, and emergency regulatory measures. The timeline of vaccine development highlights key milestones that transformed the fight against the pandemic. It began in January 2020, when the genetic sequence of SARS-CoV-2 was shared globally, enabling researchers to start designing vaccine candidates. By March 2020, Moderna and the National Institutes of Health (NIH) had already initiated Phase 1 clinical trials for their mRNA vaccine, mRNA-1273, marking the fastest-ever start to a vaccine trial for a novel pathogen.
One of the most critical milestones came in December 2020, when the U.S. Food and Drug Administration (FDA) issued Emergency Use Authorization (EUA) for Pfizer-BioNTech’s mRNA vaccine, BNT162b2, followed shortly by Moderna’s mRNA-1273. These vaccines demonstrated efficacy rates of 95% and 94.1%, respectively, in clinical trials involving tens of thousands of participants. The authorization process was expedited under Operation Warp Speed, a federal program launched in May 2020 to accelerate vaccine development, manufacturing, and distribution. This initiative invested billions of dollars in vaccine candidates, ensuring that production could begin before approvals were finalized, a risky but necessary gamble to save lives.
Another pivotal moment was the inclusion of diverse populations in clinical trials, addressing concerns about vaccine efficacy and safety across different age groups and ethnicities. For instance, Pfizer’s trials included participants as young as 12 years old, leading to the vaccine’s approval for adolescents in May 2021. Moderna’s trials also enrolled a significant number of older adults, as their risk of severe COVID-19 was higher. Dosage specifics varied: Pfizer’s vaccine required two 30-microgram doses for individuals aged 12 and older, while Moderna administered two 100-microgram doses for adults. Practical tips for recipients included scheduling doses 3–4 weeks apart and monitoring for common side effects like fatigue, headache, and soreness at the injection site.
The timeline also underscores the importance of adaptability in vaccine development. In late 2021, the emergence of the Omicron variant prompted the FDA to authorize booster shots for both Pfizer and Moderna vaccines, enhancing immunity against evolving strains. Additionally, Johnson & Johnson’s adenovirus-based vaccine, authorized in February 2021, offered a single-dose option, providing flexibility for individuals hesitant about a two-dose regimen. However, its rollout was temporarily paused in April 2021 to investigate rare blood clot cases, demonstrating the balance between speed and safety in vaccine deployment.
Finally, the U.S. vaccine development timeline serves as a testament to human ingenuity and collaboration. From the rapid sequencing of the virus to the deployment of over 200 million doses within the first six months of authorization, the process was a marathon of scientific achievement. Practical takeaways include the importance of staying informed about booster recommendations, especially for vulnerable populations, and following CDC guidelines for vaccine storage and administration. The U.S. not only answered the question of whether it had vaccines for coronavirus but also set a global standard for how quickly and effectively vaccines could be developed and distributed during a public health crisis.
Writing a Religious Exemption for Vaccines in Massachusetts: A Guide
You may want to see also
Explore related products

$13.53 $30

$18.99 $18.99




![]()
Approved Vaccines: List of FDA-approved or authorized COVID-19 vaccines in the U.S
The U.S. has multiple COVID-19 vaccines approved or authorized by the FDA, each with distinct characteristics tailored to different age groups and needs. As of the latest updates, the primary vaccines available are Pfizer-BioNTech, Moderna, and Novavax, with Johnson & Johnson’s Janssen vaccine no longer recommended due to rare but serious side effects. Understanding these options is crucial for making informed decisions about vaccination.
Pfizer-BioNTech (Comirnaty) stands out as the first FDA-approved COVID-19 vaccine for individuals aged 12 and older. For this age group, the dosage is 30 micrograms per shot, administered as a two-dose primary series separated by 3–8 weeks. Children aged 5–11 receive a lower dose of 10 micrograms, also given in two shots. A bivalent booster, targeting both the original virus and Omicron subvariants, is authorized for everyone aged 5 and older. Practical tip: Schedule your booster at least 2 months after the last dose to maximize protection against circulating strains.
Moderna’s vaccine, marketed as Spikevax, is FDA-approved for individuals aged 18 and older. The primary series consists of two 100-microgram doses given 4–8 weeks apart. For adolescents aged 6–17, a lower dosage is used, though it remains under emergency use authorization. Like Pfizer, Moderna offers a bivalent booster for adults and children aged 6 months and older. Caution: Moderna’s higher dosage can cause more pronounced side effects, such as fatigue or muscle pain, but these are typically short-lived and manageable with over-the-counter pain relievers.
Novavax’s protein-based vaccine provides an alternative for those hesitant about mRNA technology. Authorized for individuals aged 12 and older, it uses a more traditional approach by introducing a stabilized version of the SARS-CoV-2 spike protein. The primary series is two 5-microgram doses, administered 3–8 weeks apart. This vaccine is particularly appealing for those with mRNA vaccine allergies or preferences for protein-based formulations. Takeaway: Novavax broadens the U.S. vaccine portfolio, offering flexibility in vaccination strategies.
When choosing a vaccine, consider factors like age eligibility, dosage requirements, and personal health history. For instance, pregnant individuals are strongly encouraged to get vaccinated, with Pfizer and Moderna being the preferred options due to extensive safety data. Always consult a healthcare provider to determine the best vaccine for your specific situation. Staying updated with FDA guidelines ensures you receive the most effective protection against COVID-19.
Vaccine vs. Inoculation: Understanding the Key Differences and Similarities
You may want to see also
Explore related products






![]()
Vaccine Distribution: How COVID-19 vaccines are allocated and distributed across the U.S
The U.S. has not only developed multiple COVID-19 vaccines but has also established a complex system to ensure their equitable distribution. This process involves federal, state, and local coordination, with priorities shifting as vaccine availability and public health needs evolve. Initially, limited supplies meant strict allocation based on risk factors, but as production scaled up, distribution expanded to reach broader populations.
Allocation Strategies: From Scarcity to Abundance
During the early phases of vaccine rollout, the Centers for Disease Control and Prevention (CDC) prioritized healthcare workers, long-term care facility residents, and individuals aged 65 and older. This phased approach aimed to protect those most vulnerable to severe illness and death. For instance, the Pfizer-BioNTech vaccine, authorized for individuals aged 16 and older, required two doses spaced 21 days apart, while Moderna’s vaccine, for those 18 and older, followed a 28-day interval. As supply increased, eligibility expanded to include essential workers, then all adults by April 2021. Pediatric doses for children aged 5–11 were introduced later, with smaller dosages (10 micrograms compared to 30 micrograms for adults) to balance efficacy and safety.
Distribution Channels: A Multi-Pronged Approach
Vaccines are distributed through a network of providers, including pharmacies, hospitals, community health centers, and mass vaccination sites. Federal programs like the Pharmacy Partnership for Long-Term Care Program prioritized nursing homes, while state health departments allocated doses to local jurisdictions based on population size and need. For example, rural areas often relied on mobile clinics and pop-up sites to overcome geographic barriers. Pharmacies, such as CVS and Walgreens, played a pivotal role, administering over 50% of all vaccine doses at one point. Online platforms like VaccineFinder and state-specific registration systems helped individuals locate and schedule appointments, though early rollout was marred by technical glitches and inequitable access.
Equity Challenges: Addressing Disparities
Despite efforts, vaccine distribution highlighted existing health disparities. Minority communities, often disproportionately affected by COVID-19, faced barriers like limited access to technology, transportation, and mistrust rooted in historical injustices. To address this, initiatives like the Health Resources and Services Administration’s (HRSA) allocation to community health centers aimed to reach underserved populations. Additionally, targeted campaigns in languages other than English and partnerships with faith-based organizations helped improve uptake. However, data from the Kaiser Family Foundation showed that as of mid-2021, vaccination rates among Black and Hispanic populations lagged behind those of white populations in many states.
Practical Tips for Individuals: Navigating the System
For those seeking vaccination, staying informed is key. Check your state’s health department website for eligibility criteria and registration details. Use tools like VaccineFinder or call the CDC’s hotline (1-800-232-0233) for assistance. If you’re eligible for a booster, note that timing varies: Pfizer and Moderna boosters are recommended 5 months after the second dose, while Johnson & Johnson’s single-dose vaccine requires a booster after 2 months. Keep your vaccination card or digital record handy, as some venues or travel may require proof. Finally, be patient—while supply is no longer a major issue, local demand and logistics can still affect availability.
This system, though imperfect, has vaccinated hundreds of millions of Americans, demonstrating the power of coordinated public health efforts. As new variants emerge, ongoing adaptation will be crucial to sustaining progress.
Understanding France's Tdap Vaccine: Name, Purpose, and Importance Explained
You may want to see also
Explore related products






![]()
Vaccine Efficacy: Effectiveness of U.S.-approved COVID-19 vaccines against variants and symptoms
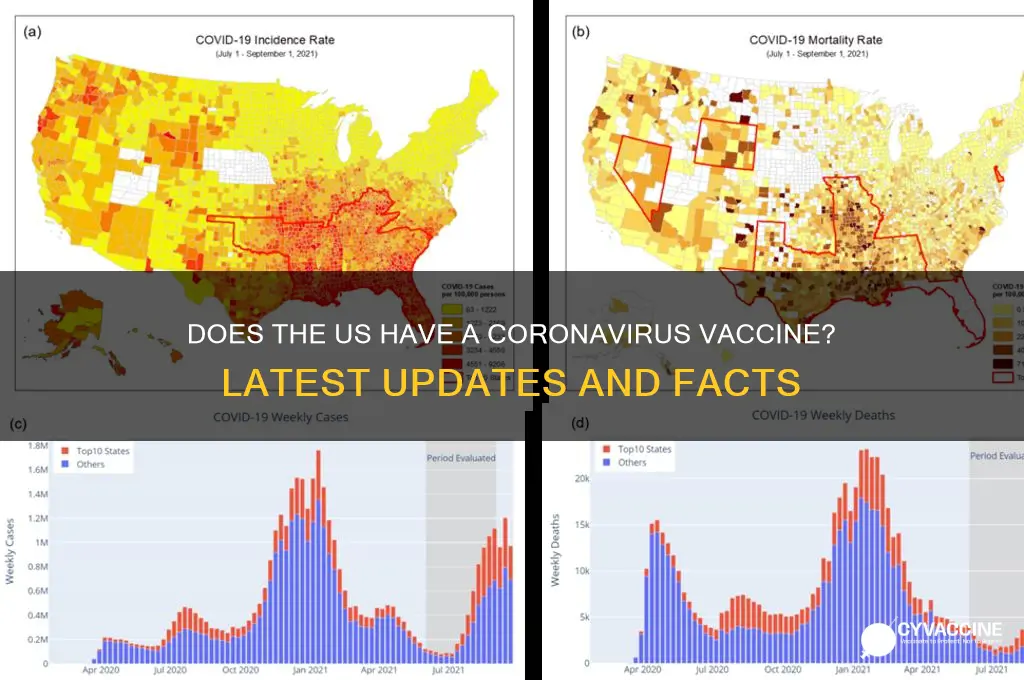
The U.S. has approved multiple COVID-19 vaccines, but their effectiveness against emerging variants and symptoms remains a critical concern. The Pfizer-BioNTech and Moderna mRNA vaccines, initially boasting 94-95% efficacy against symptomatic infection from the original strain, have faced challenges with variants like Delta and Omicron. Studies show that while these vaccines remain highly effective in preventing severe illness and hospitalization, their protection against infection wanes over time, particularly with Omicron subvariants. For instance, a CDC study found that three months after a second dose, Pfizer’s efficacy against infection dropped to 42%, though it remained 80% effective against hospitalization. Booster doses significantly restore protection, with a third shot increasing efficacy against symptomatic infection to around 70-75% for several months.
Analyzing vaccine efficacy by age group reveals disparities. Older adults, particularly those over 65, experience reduced vaccine effectiveness due to age-related immune decline. For example, a study in *The Lancet* showed that while two doses of Moderna provided 89% protection against hospitalization in adults under 65, efficacy dropped to 76% in those over 65. This underscores the importance of boosters for this demographic. Conversely, children aged 5-11 receive a lower dosage (10 micrograms for Pfizer compared to 30 micrograms for adults), tailored to balance efficacy and safety. Data indicate this regimen provides robust protection against severe disease, though its effectiveness against infection is lower than in adults, particularly with Omicron.
Practical tips for maximizing vaccine efficacy include adhering to recommended dosing intervals and staying updated with boosters. For Pfizer and Moderna, the optimal interval between the first and second dose is 3-4 weeks, with a booster at least 5 months later. Johnson & Johnson recipients should receive an mRNA booster 2 months after their initial dose for enhanced protection. Additionally, combining vaccines (e.g., a J&J primary dose followed by an mRNA booster) has shown superior efficacy compared to homologous boosting. Monitoring breakthrough infections and symptoms post-vaccination is crucial; while vaccines reduce severity, vaccinated individuals can still experience mild symptoms like fatigue, headache, or low-grade fever, particularly with variants like Omicron.
Comparing vaccine efficacy against symptoms highlights the importance of vaccination even in the face of variants. Unvaccinated individuals are 10 times more likely to be hospitalized and 11 times more likely to die from COVID-19 than those fully vaccinated, according to CDC data. While vaccines may not prevent all infections, they drastically reduce the risk of severe outcomes. For example, during the Omicron surge, unvaccinated individuals accounted for 60% of COVID-19 hospitalizations despite representing only 25% of the eligible population. This disparity emphasizes the vaccines’ role in mitigating the pandemic’s impact on healthcare systems and individual health.
In conclusion, U.S.-approved COVID-19 vaccines remain a cornerstone of public health defense, but their efficacy against variants and symptoms requires ongoing vigilance. Boosters are essential to maintain protection, particularly for vulnerable populations. Understanding age-specific responses and following dosing guidelines can optimize individual and community outcomes. While no vaccine offers 100% protection, their ability to prevent severe disease and death is undeniable, making them a critical tool in the fight against COVID-19.
Marianne Williamson's Controversial Stance on Vaccinations: A Deep Dive
You may want to see also
Explore related products






![]()
Vaccine Mandates: Federal and state policies on COVID-19 vaccine requirements in the U.S
The U.S. has authorized multiple COVID-19 vaccines, but the rollout of vaccine mandates has been a patchwork of federal and state policies, reflecting a complex interplay of public health goals, legal challenges, and political divides. At the federal level, President Biden’s September 2021 executive order mandated vaccination for federal employees and contractors, affecting over 4 million workers. Additionally, the Occupational Safety and Health Administration (OSHA) issued a rule requiring businesses with 100+ employees to implement vaccine-or-test policies, though this was later struck down by the Supreme Court. These federal efforts aimed to curb transmission and protect essential services but faced significant legal and logistical hurdles.
States, however, have taken vastly different approaches, creating a fragmented landscape of vaccine requirements. California, for instance, mandated vaccines for all healthcare workers and state employees, with no test alternative, while Florida banned vaccine mandates altogether, even prohibiting businesses from requiring proof of vaccination. These disparities highlight the tension between state autonomy and federal authority, as well as the role of local politics in shaping public health measures. For example, in New York City, private-sector employees were required to be vaccinated under the "Key to NYC" program, a policy that was both praised for its rigor and criticized for its economic impact on small businesses.
Practical implementation of mandates has also varied widely. Some states, like Connecticut, prioritized education, offering vaccine clinics in schools for students aged 12 and up, while others, like Texas, focused on voluntary compliance, leaving decisions to individual school districts. Dosage schedules further complicate mandates, as boosters became necessary for full compliance in many jurisdictions. For instance, the CDC recommends a second booster for adults over 50, but states like Arizona have not incorporated this into their mandate requirements, creating confusion among residents.
The legal battles surrounding mandates underscore their contentious nature. In *Biden v. Missouri*, the Supreme Court upheld federal vaccine mandates for healthcare workers at facilities receiving Medicare/Medicaid funding, affecting 10.3 million workers. Conversely, state-level mandates have faced challenges under the Tenth Amendment, with courts often siding with states’ rights. This legal ambiguity has left employers and individuals navigating a maze of rules, with compliance often dependent on location rather than uniform standards.
Despite the controversy, vaccine mandates have demonstrably increased vaccination rates in targeted populations. Federal data shows that 98% of federal employees complied with the mandate, while states with strict healthcare worker requirements, like Rhode Island, saw vaccination rates exceed 95%. However, mandates remain a double-edged sword, balancing public health benefits against concerns about individual liberty and economic disruption. As the pandemic evolves, policymakers must weigh these trade-offs, ensuring mandates are both effective and equitable.
Understanding When It's Acceptable to Opt Out of Childhood Vaccinations
You may want to see also
Frequently asked questions
Yes, the US has multiple FDA-approved and authorized vaccines for COVID-19, including Pfizer-BioNTech, Moderna, and Johnson & Johnson (Janssen).
Yes, COVID-19 vaccines are widely available across the US through pharmacies, healthcare providers, community clinics, and local health departments.
As of 2023, COVID-19 vaccines are available to everyone aged 6 months and older in the US, with specific recommendations varying by age and health status.
Yes, COVID-19 vaccines are free for everyone in the US, regardless of insurance or immigration status, under the federal government’s program.
COVID-19 vaccines in the US are highly effective at preventing severe illness, hospitalization, and death, though effectiveness may vary against different variants. Booster doses are recommended to maintain protection.