The timing between vaccine doses has become a critical aspect of public health discussions, particularly in the context of global vaccination campaigns against diseases like COVID-19. While vaccine manufacturers provide recommended intervals based on clinical trial data, real-world scenarios often involve deviations due to supply constraints, logistical challenges, or individual health considerations. The question of whether the time between doses significantly impacts vaccine efficacy, immune response, or safety remains a subject of ongoing research. Studies suggest that while adhering to the recommended schedule is ideal, slight delays may not necessarily compromise the overall effectiveness of the vaccine. However, extended intervals could potentially leave individuals more vulnerable during the waiting period or alter the immune response dynamics. Understanding the implications of dose spacing is essential for optimizing vaccination strategies and ensuring broad protection against infectious diseases.
| Characteristics | Values |
|---|---|
| Optimal Interval | Varies by vaccine type and manufacturer recommendations. For example, mRNA COVID-19 vaccines (Pfizer, Moderna) recommend 3-4 weeks between doses for initial series, while AstraZeneca recommends 4-12 weeks. |
| Immune Response | Longer intervals (e.g., 8-12 weeks) often enhance immune response and antibody production, particularly for COVID-19 and other viral vaccines. |
| Efficacy | Extended intervals can improve vaccine efficacy. For instance, a 12-week gap between AstraZeneca doses showed higher efficacy compared to shorter intervals. |
| Side Effects | Longer intervals may reduce side effects like fatigue, headache, and fever, as the immune system has more time to adjust. |
| Flexibility | Some vaccines allow flexibility in dosing intervals (e.g., 4-12 weeks) without compromising efficacy, providing logistical advantages. |
| Booster Doses | Timing between primary series and booster doses matters; longer intervals (e.g., 6+ months) often yield stronger immune responses. |
| Age Considerations | Intervals may vary by age group. For example, older adults might benefit from longer intervals for certain vaccines. |
| Vaccine Type | Live attenuated vaccines (e.g., MMR) typically require longer intervals (4-6 weeks) between doses compared to inactivated or mRNA vaccines. |
| Public Health Context | During outbreaks, shorter intervals may be prioritized to achieve faster population immunity, even if efficacy is slightly reduced. |
| Research Findings | Studies show that longer intervals between doses can lead to higher neutralizing antibody titers and longer-lasting immunity. |
Explore related products





What You'll Learn
![]()
Optimal Timing for Vaccine Efficacy
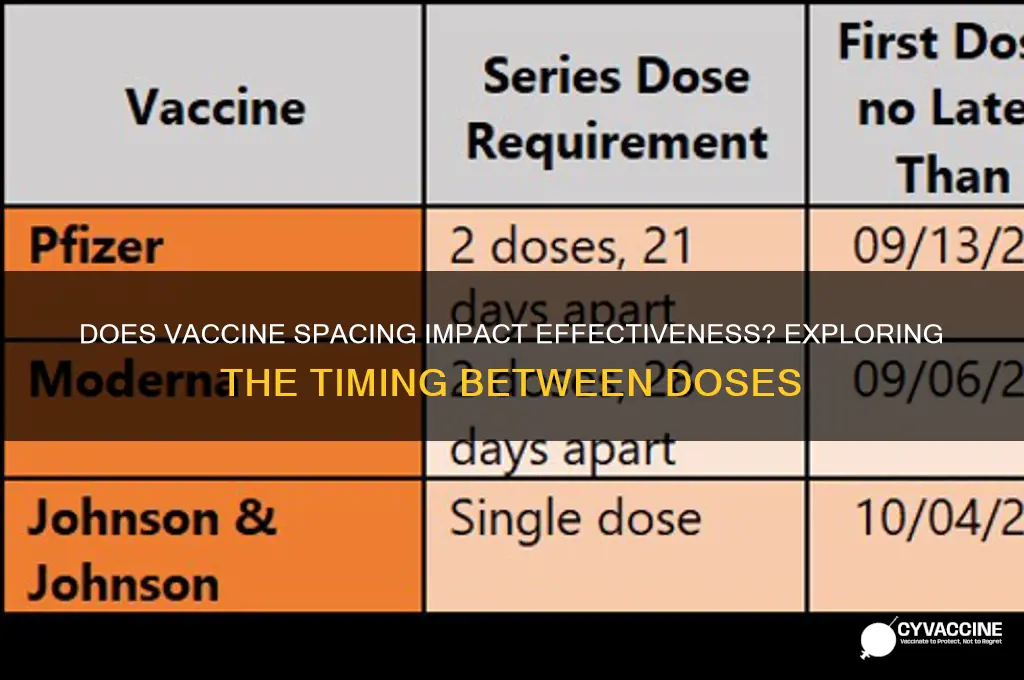
The interval between vaccine doses can significantly impact immune response, with optimal timing varying by vaccine type and individual factors. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) demonstrate enhanced efficacy when the second dose is administered 3–4 weeks after the first, as per clinical trial data. This timing maximizes the production of neutralizing antibodies while minimizing the risk of adverse reactions. Deviating from this schedule—either shortening or prolonging the interval—may reduce immunogenicity, underscoring the importance of adhering to recommended timelines.
Consider the influenza vaccine, which operates on a different principle. Annual flu shots are typically administered in a single dose, but for children under 9 receiving it for the first time, two doses spaced 4 weeks apart are required. This staggered approach ensures robust immune memory in a demographic with less mature immune systems. In contrast, the HPV vaccine (Gardasil 9) follows a 0-2-6 month schedule for individuals aged 9–14, while those 15 and older require a 0-2-6 month or 0-1-6 month regimen. These variations highlight how age and vaccine formulation dictate optimal dosing intervals.
Practical considerations also play a role in determining the best timing. For travelers requiring accelerated protection, some vaccines, like hepatitis A, offer a rapid schedule (0-7-21 days plus a booster at 12 months). However, this approach may compromise long-term immunity compared to the standard 6-month interval. Similarly, catch-up schedules for missed doses often involve shorter intervals to expedite protection, but these must balance efficacy with safety, as rapid dosing can increase side effects. Always consult healthcare providers to tailor timing to individual needs.
A comparative analysis of vaccine intervals reveals a trade-off between rapid immunity and sustained protection. For example, the shingles vaccine (Shingrix) requires two doses spaced 2–6 months apart, with studies showing higher antibody levels when administered at the 2-month mark. Yet, delaying the second dose slightly can accommodate individuals with scheduling constraints without significantly compromising efficacy. This flexibility contrasts with vaccines like MMR, where strict adherence to the 4-week minimum interval is critical to ensure proper immune priming.
In conclusion, optimal vaccine timing is a delicate balance of science and practicality. Healthcare providers must weigh factors like age, vaccine type, and individual health status when recommending dosing intervals. Patients should follow prescribed schedules closely but communicate any challenges to adjust plans without sacrificing efficacy. As research evolves, so too will guidelines, emphasizing the dynamic nature of vaccine administration protocols.
Understanding the Proper Administration of the Polio Vaccine: A Guide
You may want to see also
Explore related products






![]()
Impact of Delayed Second Dose
The timing between vaccine doses can significantly influence immune response, particularly for vaccines requiring multiple administrations. Delayed second doses, whether intentional or due to logistical challenges, have been studied across various vaccines, including COVID-19, HPV, and hepatitis B. For instance, the COVID-19 vaccine trials initially tested a 3- to 4-week interval between doses, but real-world scenarios often extended this gap. Research indicates that a longer interval can enhance antibody production in some cases, such as with the AstraZeneca and Pfizer vaccines, where a 12-week delay showed higher efficacy compared to shorter intervals. However, this benefit is not universal; the optimal timing depends on the vaccine type, individual health status, and the urgency of protection needed.
From a practical standpoint, delaying the second dose can be a strategic decision in resource-constrained settings or during vaccine shortages. For example, the UK extended the interval between COVID-19 doses to maximize first-dose coverage, prioritizing partial immunity for a larger population. This approach requires careful consideration, as prolonged delays may reduce overall efficacy or leave individuals vulnerable during the interim period. For vaccines like HPV, which typically follow a 0-2-6 month schedule, deviations of a few weeks are generally acceptable but should not exceed manufacturer recommendations. Always consult healthcare providers for personalized advice, especially for immunocompromised individuals or those with specific health conditions.
A comparative analysis of delayed dosing reveals both advantages and risks. Longer intervals between doses can lead to a more robust immune response, as seen in studies where participants received their second COVID-19 dose after 6–12 weeks instead of 3–4 weeks. However, this delay may not be suitable for high-risk populations, such as the elderly or those with comorbidities, who require rapid protection. For instance, a delayed second dose of the hepatitis B vaccine could compromise immunity in healthcare workers exposed to the virus. Balancing these factors requires a nuanced approach, considering both individual and public health needs.
To navigate delayed second doses effectively, follow these steps: first, adhere to the recommended schedule whenever possible, as it is based on clinical trial data. If a delay is unavoidable, ensure it does not exceed the maximum interval specified by the vaccine manufacturer (e.g., 6 weeks for Moderna or 8 weeks for Pfizer). Second, monitor for symptoms or exposure risks during the extended gap, especially in high-transmission settings. Finally, document the delay and communicate it to healthcare providers to ensure accurate immunization records and future dosing decisions. While flexibility in dosing can be beneficial, it should be approached with caution and informed by scientific evidence.
Ovarian Cancer Vaccine: Key Questions to Ask Before Getting Vaccinated
You may want to see also
Explore related products






![]()
Immune Response and Interval Length
The timing between vaccine doses can significantly influence the strength and durability of the immune response. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) initially recommended a 3- to 4-week interval between doses, but studies showed that extending this to 6–8 weeks could enhance antibody production in some age groups, particularly those over 65. This phenomenon, known as immune memory boosting, occurs because a longer interval allows the body to mature its immune cells more effectively, leading to a robust and sustained response. However, this isn’t a one-size-fits-all rule; the optimal interval varies by vaccine type, age, and underlying health conditions.
Consider the measles, mumps, and rubella (MMR) vaccine, which typically requires a 4-week minimum interval between doses. Administering the second dose too soon can result in immune interference, where the first dose’s response suppresses the second, reducing overall efficacy. Conversely, the HPV vaccine (Gardasil 9) demonstrates flexibility, with intervals ranging from 1–13 months for the second dose and up to 12 months for the third dose in individuals aged 9–14. This variability highlights the importance of adhering to manufacturer guidelines, as they are based on clinical trials that balance immune response optimization with practical administration schedules.
From a practical standpoint, healthcare providers must weigh the benefits of extended intervals against the risks of delayed protection, especially in outbreak scenarios. For example, during a measles outbreak, the CDC recommends reducing the MMR interval to 4 weeks for immediate protection, even if it means slightly compromising long-term immunity. Similarly, for travelers needing accelerated protection, some vaccines, like hepatitis A, allow for a 0- to 7-day interval between doses in specific circumstances, though this is an exception rather than the rule. These adjustments underscore the need for individualized vaccine scheduling based on risk factors and public health priorities.
To maximize immune response, patients should follow these actionable steps: first, confirm the recommended interval for their specific vaccine and age group with their healthcare provider. Second, avoid self-adjusting intervals without medical advice, as this can undermine efficacy. Third, keep a record of vaccination dates and share them with all healthcare providers to ensure continuity of care. Finally, stay informed about updates to vaccine schedules, as guidelines evolve with new research. By understanding the interplay between immune response and interval length, individuals can make informed decisions to optimize their protection.
Can a Vaccine Prevent Croup? Exploring Protection Against This Respiratory Illness
You may want to see also
Explore related products






![]()
Scheduling Flexibility in Vaccination
The timing between vaccine doses can significantly impact their effectiveness, but life often gets in the way of rigid schedules. Scheduling flexibility in vaccination protocols acknowledges this reality, allowing individuals to complete their vaccine series without starting over, even if doses are delayed. This approach is particularly crucial for multi-dose vaccines like the COVID-19 mRNA vaccines, where the recommended interval between doses is 3-4 weeks, but delays are common due to supply shortages, personal circumstances, or adverse reactions.
Health organizations like the CDC and WHO have recognized the need for flexibility, providing guidelines that allow for extended intervals between doses without compromising immunity. For instance, the Pfizer-BioNTech COVID-19 vaccine can be administered up to 6 weeks apart, while the Moderna vaccine allows for an interval of up to 8 weeks. This flexibility ensures that individuals can still achieve optimal protection, even if they miss their initial appointment.
Consider a scenario where a 35-year-old individual receives their first dose of the Moderna COVID-19 vaccine but experiences a severe adverse reaction, requiring a 6-week delay before receiving the second dose. In this case, scheduling flexibility allows them to complete the vaccine series without restarting, as the extended interval is within the recommended range. To ensure optimal protection, healthcare providers should educate patients on the importance of completing the vaccine series, even if doses are delayed, and provide clear instructions on rescheduling missed appointments.
A comparative analysis of vaccination schedules reveals that some vaccines, like the HPV vaccine, have more stringent timing requirements, with a recommended interval of 6-12 months between doses. In contrast, others, like the influenza vaccine, are administered annually and do not require a specific interval between doses. This highlights the need for a nuanced approach to scheduling flexibility, taking into account the unique characteristics of each vaccine. For example, individuals aged 50 and above receiving the shingles vaccine (Shingrix) should aim for a 2- to 6-month interval between doses, but a delay of up to 12 months is still considered acceptable.
To maximize the benefits of scheduling flexibility, individuals should: (1) keep a record of their vaccination history, including dates and types of vaccines received; (2) communicate any delays or concerns with their healthcare provider; and (3) prioritize rescheduling missed appointments as soon as possible. Healthcare providers can support this process by offering reminder systems, providing clear instructions on rescheduling, and educating patients on the importance of completing the vaccine series. By embracing scheduling flexibility, we can ensure that more individuals achieve optimal protection, even in the face of unpredictable circumstances. This approach not only improves individual health outcomes but also contributes to herd immunity, reducing the spread of vaccine-preventable diseases.
Booster Shot Timeline: When Are You Fully Vaccinated After the Dose?
You may want to see also
Explore related products






![]()
Safety of Extended Dose Intervals
Extended dose intervals for vaccines have become a focal point in immunization strategies, particularly during vaccine shortages or logistical challenges. For instance, the COVID-19 pandemic prompted countries like the UK and Canada to extend the interval between mRNA vaccine doses from 3–4 weeks to 8–12 weeks. This decision was driven by the need to maximize first-dose coverage and provide immediate partial protection to a larger population. Research from *The Lancet* suggests that longer intervals between doses can enhance immune responses, particularly for certain vaccines like the Oxford-AstraZeneca and Pfizer-BioNTech formulations, where antibody levels were observed to be higher with extended intervals.
However, the safety of extended dose intervals hinges on balancing immunogenicity with vulnerability. For example, in the case of the Pfizer-BioNTech vaccine, a 12-week interval was found to produce a stronger immune response compared to a 3-week interval, but this approach may not be suitable for high-risk populations, such as the elderly or immunocompromised individuals, who require rapid protection. Pediatric vaccines, like the MMR series, typically require a 4-week minimum interval, and deviating from this could compromise efficacy. Always consult vaccine-specific guidelines, such as those from the CDC or WHO, before adjusting intervals, as these recommendations are based on rigorous clinical trials.
Practical implementation of extended intervals requires careful planning. For instance, if a second dose of a vaccine is delayed beyond the recommended window, it does not necessitate restarting the series. Instead, administer the dose as soon as feasible. For combination vaccines, such as DTaP-IPV-Hib, adherence to the 4–8 week interval is critical to ensure proper immune memory formation. In resource-limited settings, extending intervals can be a strategic tool, but it must be paired with robust tracking systems to ensure completion of the vaccine series. Mobile health apps or community health workers can play a vital role in reminding recipients of their follow-up appointments.
Critics argue that extended intervals may increase the risk of breakthrough infections during the gap between doses, particularly in regions with high disease transmission. For example, during the COVID-19 vaccine rollout, some countries experienced higher case rates among partially vaccinated individuals awaiting their second dose. To mitigate this, public health measures like masking and social distancing should remain in place until full vaccination is achieved. Additionally, serological testing can be used to assess immune responses in individuals with extended intervals, though this is not yet standard practice.
In conclusion, the safety of extended dose intervals is context-dependent and requires a nuanced approach. While longer intervals can enhance immune responses for certain vaccines, they must be tailored to the specific vaccine, population, and epidemiological setting. Policymakers and healthcare providers should weigh the benefits of increased immunogenicity against the risks of delayed protection, ensuring that any deviation from standard intervals is evidence-based and supported by robust monitoring systems. Practical tools, such as digital reminders and community outreach, can help maintain vaccine series completion rates, even with extended schedules.
Varicella Vaccine Introduction in Australia: A Historical Overview
You may want to see also
Frequently asked questions
Yes, the timing between vaccine doses can impact effectiveness. Many vaccines are designed to be administered in specific intervals to optimize the immune response. Deviating from the recommended schedule may reduce immunity or require additional doses.
It’s generally not recommended to get a vaccine dose earlier than the advised interval. The timing is based on clinical trials to ensure maximum protection and safety. Early dosing may not provide the intended immune response.
Delaying a vaccine dose beyond the recommended interval is usually acceptable, but it may temporarily reduce protection. However, once the delayed dose is administered, the immune response is expected to catch up, providing full protection.
Yes, the timing of booster shots is important. Boosters are scheduled to maintain immunity levels over time. Receiving a booster too early or too late may affect its effectiveness in enhancing protection against the targeted disease.