The question of whether the United States has a vaccine is a critical and multifaceted one, particularly in the context of public health crises such as the COVID-19 pandemic. As of recent developments, the U.S. has indeed developed, authorized, and distributed multiple vaccines to combat COVID-19, with leading examples including those produced by Pfizer-BioNTech, Moderna, and Johnson & Johnson. These vaccines have undergone rigorous testing and have been approved by the Food and Drug Administration (FDA) for emergency use, playing a pivotal role in reducing severe illness, hospitalizations, and deaths. Beyond COVID-19, the U.S. has a robust history of vaccine development and distribution for diseases like influenza, measles, and polio, supported by extensive research, public health initiatives, and partnerships with pharmaceutical companies. However, the availability and accessibility of vaccines can vary depending on factors such as geographic location, socioeconomic status, and public health infrastructure, highlighting ongoing challenges in ensuring equitable vaccine distribution nationwide.
| Characteristics | Values |
|---|---|
| Vaccine Availability | Yes, the US has multiple COVID-19 vaccines available. |
| Approved Vaccines | Pfizer-BioNTech, Moderna, Johnson & Johnson (J&J)/Janssen (Note: J&J vaccine use is limited due to rare blood clot risks) |
| Eligibility | Everyone aged 6 months and older is eligible for vaccination. |
| Booster Shots | Recommended for everyone aged 5 and older, with specific timing and dosage depending on age and initial vaccine series. |
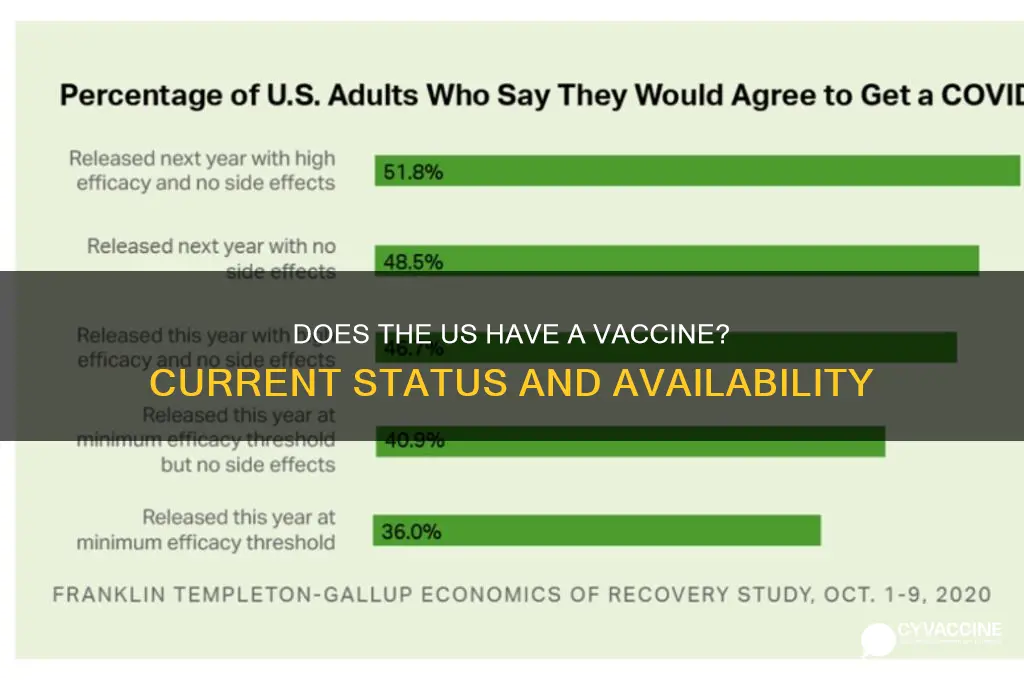
| Vaccination Rate (as of October 2023) | Approximately 68% of the total US population is fully vaccinated. |
| Vaccine Distribution | Distributed through pharmacies, healthcare providers, community clinics, and mobile units. |
| Cost | Free for all individuals, regardless of insurance status. |
| Vaccine Development | Developed and authorized under Emergency Use Authorization (EUA) or full FDA approval. |
| Efficacy | High efficacy in preventing severe illness, hospitalization, and death from COVID-19. |
| Side Effects | Generally mild to moderate, including pain at the injection site, fatigue, headache, and muscle pain. |
Explore related products






What You'll Learn
- FDA Approval Process: Steps and timeline for FDA approval of vaccines in the United States
- Vaccine Availability: Distribution and access to vaccines across different U.S. states
- Vaccine Types: Overview of COVID-19 vaccines (Pfizer, Moderna, Johnson & Johnson) available in the U.S
- Vaccine Mandates: Federal and state policies on vaccine requirements for work, travel, and schools
- Vaccine Hesitancy: Factors contributing to vaccine skepticism and efforts to address public concerns
![]()
FDA Approval Process: Steps and timeline for FDA approval of vaccines in the United States
The FDA's approval process for vaccines is a rigorous, multi-stage journey designed to ensure safety, efficacy, and quality. It begins with preclinical testing, where potential vaccines are studied in labs and animal models to assess their basic safety and immune response. This phase, though not involving humans, is critical for identifying red flags before advancing to clinical trials. For instance, the COVID-19 vaccines underwent extensive preclinical testing to evaluate their ability to neutralize the SARS-CoV-2 virus, a step that paved the way for human trials.
Once preclinical data is promising, the process moves to three phases of clinical trials. Phase 1 involves a small group (20–100 volunteers) to test safety, dosage, and immune response. Phase 2 expands to several hundred participants to further evaluate safety and efficacy, often including diverse age groups. For vaccines like Pfizer’s COVID-19 shot, Phase 2 included participants aged 12 and older to gather data on adolescent responses. Phase 3 is the largest, involving thousands to tens of thousands of people, to confirm efficacy and monitor side effects. For example, the Pfizer-BioNTech COVID-19 vaccine’s Phase 3 trial included over 43,000 participants, demonstrating 95% efficacy in preventing symptomatic infection.
After successful clinical trials, manufacturers submit a Biologics License Application (BLA) to the FDA, a comprehensive package including all data from preclinical and clinical studies, manufacturing details, and proposed labeling. The FDA reviews this submission, often taking 6–10 months for standard approvals. However, during public health emergencies, the FDA can issue Emergency Use Authorizations (EUAs) based on less complete data, as seen with COVID-19 vaccines. EUAs require at least two months of safety data post-vaccination, while full approval demands six months or more.
Post-approval, the FDA continues to monitor vaccines through programs like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). These systems track rare or long-term side effects, ensuring ongoing safety. For instance, the rare link between the Johnson & Johnson COVID-19 vaccine and thrombosis with thrombocytopenia syndrome (TTS) was identified through post-approval surveillance, leading to updated guidelines.
Understanding this process highlights the balance between speed and safety. While EUAs expedited COVID-19 vaccine availability, full FDA approval, as granted to Pfizer’s Comirnaty in August 2021, provides additional confidence in long-term safety and efficacy. For the public, this means trusting that approved vaccines have met stringent criteria, while remaining informed about ongoing monitoring efforts.
J&J Vaccine Ingredients: Understanding What's Inside the Johnson & Johnson Shot
You may want to see also
Explore related products






![]()
Vaccine Availability: Distribution and access to vaccines across different U.S. states
The United States has authorized multiple vaccines for various diseases, including COVID-19, influenza, and measles, but their distribution and accessibility vary significantly across states. For instance, during the COVID-19 pandemic, states like California and New York received larger vaccine allocations due to their higher populations, while rural states like Wyoming and Vermont faced logistical challenges in reaching dispersed communities. This disparity highlights the complexity of vaccine distribution, which is influenced by population density, infrastructure, and state-specific policies. Understanding these differences is crucial for ensuring equitable access to life-saving vaccines.
To address distribution challenges, the U.S. government implemented a phased approach during the COVID-19 vaccine rollout, prioritizing healthcare workers, the elderly, and those with underlying conditions. However, states had autonomy in defining eligibility criteria, leading to inconsistencies. For example, while some states strictly followed federal guidelines, others expanded eligibility to essential workers earlier. This flexibility allowed states to adapt to local needs but also created confusion among residents. Practical tips for individuals include checking state health department websites for eligibility updates and using tools like VaccineFinder to locate nearby vaccination sites.
A comparative analysis reveals that states with robust public health infrastructure, such as Massachusetts and Minnesota, achieved higher vaccination rates compared to states with limited resources. These states invested in community outreach, mobile clinics, and multilingual campaigns to overcome barriers like hesitancy and transportation. In contrast, states with lower vaccination rates often lacked funding for such initiatives. This underscores the importance of federal and state collaboration in strengthening public health systems to ensure consistent vaccine access nationwide.
Persuasively, it’s essential to recognize that vaccine availability isn’t just about supply—it’s about accessibility. Rural areas, for instance, often face shortages of healthcare providers and pharmacies, making it difficult for residents to receive doses. Solutions like deploying mobile vaccination units and partnering with local pharmacies can bridge this gap. Additionally, addressing vaccine hesitancy through culturally sensitive education campaigns can improve uptake. By focusing on both distribution and acceptance, states can maximize the impact of available vaccines and protect more lives.
Finally, a descriptive look at specific vaccines, such as the annual influenza vaccine, reveals seasonal fluctuations in availability and access. States like Florida and Texas, with larger elderly populations, often experience higher demand during flu season, requiring careful inventory management. Practical steps for individuals include getting vaccinated early in the season, typically starting in September, and utilizing workplace or school-based clinics for convenience. Understanding these patterns can help both states and individuals plan effectively, ensuring that vaccines reach those who need them most when they need them most.
Plague Vaccinations: Are They Effective Against Bubonic Strain?
You may want to see also
Explore related products






![]()
Vaccine Types: Overview of COVID-19 vaccines (Pfizer, Moderna, Johnson & Johnson) available in the U.S
The U.S. has authorized three primary COVID-19 vaccines: Pfizer-BioNTech, Moderna, and Johnson & Johnson (J&J). Each vaccine has distinct characteristics, including technology, dosage, and administration guidelines, making them suitable for different populations and preferences. Understanding these differences is crucial for informed decision-making.
Pfizer-BioNTech: The mRNA Pioneer
Pfizer’s vaccine, developed with BioNTech, was the first to receive emergency use authorization (EUA) in the U.S. It uses mRNA technology, delivering genetic instructions to cells to produce the SARS-CoV-2 spike protein, triggering an immune response. The primary series consists of two doses, 30 micrograms each, administered 21 days apart for individuals aged 12 and older. For children 5–11, the dosage is reduced to 10 micrograms per shot, with a 21-day interval. Booster shots are recommended for all age groups, with specific timing based on age and immunocompromised status. Storage at ultra-cold temperatures initially posed logistical challenges, but refrigerated stability for up to 10 days has eased distribution. Pfizer’s vaccine has demonstrated high efficacy, particularly against severe disease and hospitalization.
Moderna: A Close mRNA Cousin
Moderna’s vaccine also employs mRNA technology, similar to Pfizer’s, but with a key difference: it uses a higher dosage. The primary series includes two 100-microgram doses, administered 28 days apart for individuals aged 18 and older. For adolescents 12–17, a lower dosage is under evaluation. Booster shots, half the original dose (50 micrograms), are recommended for adults. Moderna’s vaccine has shown robust efficacy, often slightly higher than Pfizer’s in some studies, particularly in older adults. Its storage requirements are similar, though it can remain stable in a refrigerator for up to 30 days, offering slightly more flexibility in distribution.
Johnson & Johnson: The One-and-Done Option
J&J’s vaccine stands out as the only single-dose option authorized in the U.S. It uses a viral vector platform, delivering genetic material via a modified adenovirus. This vaccine is approved for individuals aged 18 and older. While its initial efficacy against symptomatic disease was lower than the mRNA vaccines (around 66–72%), it has proven highly effective against severe illness and hospitalization. A booster shot is recommended for enhanced protection, particularly against variants. J&J’s vaccine is easier to store, requiring standard refrigeration, and its single-dose regimen simplifies administration, making it a practical choice for hard-to-reach populations or those hesitant to commit to a two-dose series.
Practical Tips for Vaccine Selection
Choosing a vaccine depends on individual factors such as age, health status, and personal preference. For adolescents and younger children, Pfizer is currently the only option. Adults may opt for J&J if they prefer a single dose or have concerns about mRNA technology. However, mRNA vaccines remain the preferred choice due to their higher efficacy and lower risk of rare side effects like thrombosis with thrombocytopenia syndrome (TTS) associated with J&J. Always consult healthcare providers for personalized advice, and stay updated on evolving guidelines, including booster recommendations and variant-specific formulations.
Takeaway: A Diverse Toolkit for Protection
The availability of multiple vaccine types in the U.S. ensures flexibility and broad coverage. Pfizer and Moderna offer high efficacy with mRNA technology, while J&J provides a convenient single-dose option. Each vaccine plays a vital role in the fight against COVID-19, and widespread vaccination remains the most effective strategy to curb the pandemic.
Medical Exemptions for Vaccinations: How Common Are They?
You may want to see also
Explore related products






![]()
Vaccine Mandates: Federal and state policies on vaccine requirements for work, travel, and schools
The United States has implemented a patchwork of vaccine mandates, with federal and state policies dictating requirements for work, travel, and schools. At the federal level, President Biden’s 2021 executive order required COVID-19 vaccination for federal employees and contractors, affecting over 4 million workers. This mandate included a series of doses—typically two primary shots of Pfizer or Moderna (or one Johnson & Johnson) followed by boosters as recommended by the CDC. Non-compliance could result in disciplinary action, including termination. While this policy faced legal challenges, it underscored the federal government’s authority to enforce public health measures in specific sectors.
States, however, have taken vastly different approaches, creating a complex landscape for individuals and employers. For instance, California mandates COVID-19 vaccination for all healthcare workers, with exemptions only for medical or religious reasons. In contrast, Florida prohibits private employers from enforcing vaccine mandates without allowing opt-outs, reflecting a broader anti-mandate stance. These disparities highlight the tension between state autonomy and federal guidance, leaving businesses and residents navigating conflicting rules. For travelers, this means checking state-specific requirements before crossing borders, as some states may require proof of vaccination for certain activities, while others do not.
In schools, vaccine mandates are even more varied, often tied to historical precedents for diseases like measles and mumps. While no state currently requires COVID-19 vaccination for K-12 students, some universities, like Rutgers in New Jersey, mandate it for enrollment. Age categories play a role here: Pfizer’s vaccine is approved for children as young as 6 months, but school mandates typically target older age groups. Parents should verify local policies, as some districts may require vaccinations for in-person learning, while others leave it optional. Practical tips include keeping vaccination records handy and staying updated on booster recommendations, especially for students living in dorms or participating in high-contact activities.
The debate over vaccine mandates raises questions about individual rights versus public health. Proponents argue mandates curb outbreaks and protect vulnerable populations, while opponents cite concerns over personal freedom and medical choice. A comparative analysis shows that countries with stricter mandates, like France’s health pass system, have seen higher vaccination rates but also public backlash. In the U.S., the takeaway is clear: mandates work best when paired with education and accessibility. Employers and schools can encourage compliance by offering on-site vaccination clinics, providing paid time off for doses, and addressing misinformation through trusted sources.
For those affected by mandates, understanding exemptions is crucial. Medical exemptions require documentation from a healthcare provider, while religious exemptions often demand a written statement of belief. However, these exemptions are not guaranteed and vary by state and employer. Travelers should also note that international destinations may have stricter vaccine requirements than domestic policies. For example, some countries require proof of vaccination for entry, regardless of U.S. mandates. Practical advice includes carrying digital vaccine cards, verifying requirements well in advance, and considering travel insurance that covers pandemic-related issues. Navigating this landscape requires vigilance, but with the right information, individuals can comply with mandates while protecting their health and plans.
Vaccination and Allergies: Safeguarding Health Through Immunization Strategies
You may want to see also
Explore related products






![]()
Vaccine Hesitancy: Factors contributing to vaccine skepticism and efforts to address public concerns
The United States has developed and distributed multiple vaccines, including those for COVID-19, yet vaccine hesitancy remains a significant barrier to public health. This skepticism is fueled by a complex interplay of factors, from historical mistrust in medical institutions to the rapid spread of misinformation on social media. For instance, the Tuskegee Syphilis Study, where Black men were intentionally left untreated, has left a lasting legacy of distrust among minority communities. Similarly, the speed at which COVID-19 vaccines were developed, though a testament to scientific advancement, has raised concerns about safety and efficacy among some individuals. Addressing these concerns requires understanding the root causes of hesitancy and tailoring communication strategies to build trust.
One of the primary contributors to vaccine hesitancy is the overwhelming amount of conflicting information available online. A single search for "COVID-19 vaccine side effects" can yield results ranging from peer-reviewed studies to unverified personal anecdotes, making it difficult for the average person to discern fact from fiction. For example, myths about vaccines causing infertility or altering DNA persist despite scientific evidence to the contrary. Public health campaigns must combat this by providing clear, accessible information. Practical tips include directing individuals to trusted sources like the CDC or WHO, offering localized data on vaccine efficacy, and using relatable messengers, such as community leaders or healthcare workers, to deliver messages.
Another factor is the politicization of vaccines, which has polarized public opinion and eroded trust in scientific institutions. During the COVID-19 pandemic, vaccine mandates and public health measures became divisive issues, with some viewing them as infringements on personal freedom. To bridge this divide, efforts should focus on depoliticizing health messaging and emphasizing shared values, such as protecting vulnerable populations. For instance, framing vaccination as an act of community responsibility rather than individual obligation can resonate more broadly. Additionally, addressing logistical barriers, such as ensuring vaccine accessibility in underserved areas, can reduce skepticism by demonstrating a commitment to equity.
Efforts to combat vaccine hesitancy must also consider the role of personal experiences and cultural beliefs. For parents, concerns about childhood vaccines often stem from fears of adverse reactions, even though the risk is extremely low. For example, the recommended MMR vaccine for children aged 12–15 months has a side effect rate of less than 1 in 1 million doses for severe allergic reactions. Healthcare providers can alleviate these fears by engaging in open, non-judgmental conversations, explaining the rigorous testing vaccines undergo, and sharing real-world data on safety. Cultural sensitivity is equally important; in some communities, religious or traditional beliefs may influence vaccine acceptance, requiring tailored approaches that respect these perspectives while promoting public health.
Finally, building trust in vaccines is a long-term endeavor that requires sustained investment in health literacy and community engagement. Programs like town hall meetings, vaccine clinics in schools or workplaces, and partnerships with local organizations can foster dialogue and address specific concerns. For example, offering flu vaccine clinics alongside COVID-19 boosters can normalize vaccination as a routine part of healthcare. By combining evidence-based communication with empathetic, culturally informed strategies, public health officials can gradually reduce hesitancy and increase vaccination rates, ultimately protecting both individuals and communities.
China's COVID-19 Vaccine: Development, Efficacy, and Global Impact
You may want to see also
Frequently asked questions
Yes, the US has multiple COVID-19 vaccines available, including those developed by Pfizer-BioNTech, Moderna, and Johnson & Johnson. These vaccines have been authorized for emergency use by the FDA and are widely distributed.
Yes, COVID-19 vaccines are free for everyone in the US, regardless of insurance or immigration status. The cost is covered by the federal government.
Yes, the US has vaccines for numerous diseases, including measles, mumps, rubella, influenza, hepatitis, polio, and more. These vaccines are part of routine immunization schedules and are widely available through healthcare providers and pharmacies.