When considering vaccination, the question of whether the type of vaccine matters is a crucial one, as different vaccines utilize varying technologies and mechanisms to elicit an immune response. From traditional inactivated or live-attenuated vaccines to modern mRNA and viral vector-based options, each type has unique advantages, limitations, and potential side effects. Factors such as efficacy, duration of protection, storage requirements, and accessibility can significantly influence the choice of vaccine, particularly in diverse populations with varying health needs and infrastructure capabilities. Understanding these differences is essential for informed decision-making, ensuring optimal protection against diseases while addressing individual and public health concerns.
Explore related products





What You'll Learn
- Efficacy Comparison: Different vaccines' effectiveness against COVID-19 variants and overall prevention rates
- Side Effects: Varying common and rare side effects across vaccine types
- Dosage Requirements: Single-dose vs. multi-dose vaccines and their impact on immunity
- Storage Needs: How vaccine storage requirements affect distribution and accessibility
- Immune Response: Differences in how vaccines stimulate the immune system
![]()
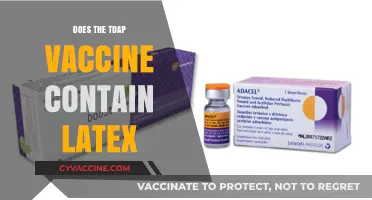
Efficacy Comparison: Different vaccines' effectiveness against COVID-19 variants and overall prevention rates
The COVID-19 pandemic has underscored the importance of vaccine efficacy, particularly as new variants emerge. Not all vaccines are created equal, and their effectiveness can vary significantly against different strains of the virus. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna have demonstrated high efficacy rates—around 95% against the original SARS-CoV-2 strain—but their performance against variants like Delta and Omicron has shown slight reductions. In contrast, viral vector vaccines such as AstraZeneca and Johnson & Johnson have lower initial efficacy rates (around 60–70%) but still provide robust protection against severe illness and hospitalization. Understanding these differences is crucial for informed decision-making, especially in regions with limited vaccine options.
Consider the dosage and administration schedules, as these can influence efficacy. mRNA vaccines typically require two doses, with a 3–4 week interval, while Johnson & Johnson’s single-dose approach offers convenience but slightly lower overall protection. Booster shots have become essential to maintain immunity, particularly against variants. Studies show that a third dose of an mRNA vaccine can restore efficacy to over 75% against symptomatic Omicron infection, compared to a significant drop in protection after just two doses. For older adults and immunocompromised individuals, timely boosters are not just recommended—they are critical for sustained defense against severe outcomes.
A comparative analysis reveals that vaccine efficacy is not solely about preventing infection but also about reducing severity and mortality. For example, while Sinovac’s inactivated virus vaccine has lower efficacy rates (around 50–60%) against symptomatic infection, it has consistently shown strong protection against hospitalization and death across multiple variants. This highlights the importance of defining what "effectiveness" means in practical terms. A vaccine that prevents severe disease and death is invaluable, even if it allows for mild breakthrough infections. Public health strategies must therefore prioritize vaccines based on their ability to minimize strain on healthcare systems.
Practical tips for individuals navigating vaccine choices include staying updated on local variant prevalence and vaccine availability. If multiple vaccines are accessible, consider factors like age, health status, and convenience. For instance, younger, healthy individuals might opt for a two-dose mRNA series for higher initial efficacy, while those in urgent need of protection might prefer a single-dose viral vector vaccine. Always follow local health guidelines for booster timing, as delays can reduce effectiveness. Finally, regardless of the vaccine type, layering protections—such as masking and testing—remains essential in high-risk settings. The type of vaccine does matter, but its impact is maximized when paired with informed, proactive measures.
Vaccination Status: A Factor for Jury Duty?
You may want to see also
Explore related products






![]()
Side Effects: Varying common and rare side effects across vaccine types
Vaccine side effects are not one-size-fits-all. Different vaccine types, from mRNA to viral vector, come with distinct profiles of common and rare reactions. Understanding these variations empowers individuals to make informed decisions and manage expectations. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna frequently cause fatigue, headache, and muscle pain after the second dose, with symptoms typically peaking within 24–48 hours and resolving within a few days. In contrast, viral vector vaccines such as Johnson & Johnson may trigger flu-like symptoms but are less likely to cause severe systemic reactions in younger adults.
Consider the age factor: adolescents and young adults often experience more pronounced side effects from mRNA vaccines due to their robust immune responses. For example, a 16-year-old might report fever and chills post-vaccination, while a 70-year-old may only experience mild arm soreness. Dosage also plays a role; pediatric formulations of mRNA vaccines contain lower mRNA concentrations (e.g., 10 μg for Pfizer in children 5–11 vs. 30 μg for adults), reducing the likelihood of severe side effects in younger age groups.
Rare side effects further highlight the importance of vaccine type. For instance, the Johnson & Johnson vaccine has been linked to a rare but serious clotting disorder called thrombosis with thrombocytopenia syndrome (TTS), occurring in approximately 7 per 1 million vaccinated women aged 18–49. Conversely, mRNA vaccines are associated with rare cases of myocarditis, primarily in adolescent males and young adults, with rates estimated at 10–100 cases per million doses. These risks, though low, underscore the need for tailored vaccine recommendations based on individual health profiles.
Practical tips can mitigate side effects regardless of vaccine type. Hydration, over-the-counter pain relievers like acetaminophen or ibuprofen, and rest are universally beneficial. However, timing matters: avoid preemptive use of pain relievers before vaccination, as it may interfere with immune response. Instead, take them only if symptoms become bothersome. For those concerned about rare side effects, monitoring for persistent or unusual symptoms (e.g., severe headache, chest pain, or shortness of breath) and seeking prompt medical attention is crucial.
In conclusion, the type of vaccine does matter when considering side effects. Common reactions vary in intensity and duration across vaccine platforms, while rare side effects differ in nature and risk groups. By recognizing these distinctions, individuals can better prepare for their vaccination experience and contribute to a more informed public dialogue on vaccine safety.
Should You Wake Your Baby to Feed After Vaccinations?
You may want to see also
Explore related products





![]()
Dosage Requirements: Single-dose vs. multi-dose vaccines and their impact on immunity
The number of doses required for a vaccine to confer immunity varies widely depending on the pathogen targeted and the vaccine’s mechanism of action. Single-dose vaccines, such as the Johnson & Johnson COVID-19 vaccine, are designed to elicit a robust immune response with just one administration, often appealing for their convenience and simplicity. In contrast, multi-dose vaccines, like the Pfizer-BioNTech and Moderna COVID-19 vaccines, require two or more doses spaced weeks apart to achieve full immunity. This difference isn’t arbitrary—it’s rooted in how the immune system learns to recognize and combat threats. Single-dose vaccines typically rely on proven platforms like adenovirus vectors, which deliver genetic material directly to cells, while multi-dose vaccines often use newer technologies like mRNA, which may require priming and boosting to ensure lasting protection.
Consider the practical implications for different populations. For children, multi-dose schedules can be challenging due to the need for multiple clinic visits, which may lead to missed doses and incomplete immunity. For example, the measles, mumps, and rubella (MMR) vaccine requires two doses, typically administered at 12–15 months and 4–6 years of age. Missing the second dose leaves individuals vulnerable, as evidenced by outbreaks in communities with low vaccination rates. Adults, too, face barriers with multi-dose vaccines, particularly in low-resource settings or among populations with limited access to healthcare. Single-dose vaccines, therefore, offer a critical advantage in such scenarios, ensuring broader coverage with fewer logistical hurdles.
From an immunological perspective, the impact of dosage frequency on immunity is nuanced. Multi-dose vaccines often produce higher antibody titers and more durable memory responses because they allow the immune system to "rehearse" its defense. For instance, the hepatitis B vaccine series (typically three doses over 6 months) provides long-term protection by gradually building immunity. Single-dose vaccines, while effective, may rely on rapid, intense immune activation, which can wane over time. Booster doses are sometimes recommended for single-dose vaccines, as seen with the Johnson & Johnson COVID-19 vaccine, which showed improved efficacy after a second dose.
When choosing between single-dose and multi-dose vaccines, healthcare providers must weigh efficacy, convenience, and population-specific needs. For travelers or individuals in outbreak zones, a single-dose vaccine might be the only feasible option. However, for long-term protection in stable populations, multi-dose regimens may be preferable despite their complexity. Practical tips include using reminder systems for multi-dose schedules, ensuring proper storage of vaccines (especially mRNA types, which require ultra-cold temperatures), and educating patients about the importance of completing all doses. Ultimately, the type of vaccine—and its dosage requirements—matters profoundly in shaping immunity and public health outcomes.
Is the COVID-19 Vaccine Truly a Vaccine? Debunking the Myths
You may want to see also
Explore related products






![]()
Storage Needs: How vaccine storage requirements affect distribution and accessibility
Vaccine storage isn’t just a logistical detail—it’s a critical factor shaping who gets vaccinated and when. Take the Pfizer-BioNTech COVID-19 vaccine, for instance. It requires ultra-cold storage at -70°C (-94°F), a condition that demands specialized freezers and precise handling. In contrast, the Moderna vaccine can be stored at -20°C (-4°F), making it more accessible in regions with less advanced infrastructure. These differences highlight how storage needs directly influence distribution, particularly in low-resource settings where ultra-cold chains are impractical.
Consider the practical implications for rural or remote areas. A vaccine that requires constant refrigeration, like the measles-mumps-rubella (MMR) vaccine (stored at 2–8°C or 36–46°F), may still pose challenges in regions with unreliable electricity. Solar-powered refrigerators or passive cooling systems can help, but they add complexity and cost. For vaccines like the oral polio vaccine, which can be stored at the same temperature range but has a shorter shelf life once opened, timely administration becomes critical. These storage demands often dictate where vaccines can be distributed and how quickly they must be used, limiting accessibility in underserved communities.
From a logistical standpoint, storage requirements also affect transportation. Vaccines needing ultra-cold storage, such as Pfizer’s, often require dry ice or specialized containers during transit. This increases costs and complicates delivery, especially in regions with poor road networks or extreme climates. In contrast, vaccines like Johnson & Johnson’s, which can be stored at standard refrigerator temperatures, are easier to transport and distribute widely. These differences underscore why some vaccines become more prevalent in certain regions while others remain out of reach.
The takeaway is clear: storage needs aren’t just a technicality—they’re a barrier or enabler of vaccine accessibility. For global health initiatives, choosing vaccines with less stringent storage requirements can mean the difference between reaching millions or leaving them unprotected. For local health providers, understanding these needs ensures vaccines remain effective from vial to injection. As new vaccines emerge, balancing efficacy with storage practicality will be key to equitable distribution. After all, a vaccine’s impact isn’t just in its formula—it’s in how easily it can reach those who need it most.
Vaccine Updates: How Are They Adapting to New COVID Variants?
You may want to see also
Explore related products






![]()
Immune Response: Differences in how vaccines stimulate the immune system
Vaccines are not one-size-fits-all; their design dictates how they engage the immune system, leading to varying responses in terms of speed, duration, and type of immunity. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna introduce genetic material that instructs cells to produce a viral protein, triggering a robust antibody and T-cell response within days. In contrast, viral vector vaccines such as AstraZeneca and Johnson & Johnson use a modified virus to deliver genetic instructions, eliciting a more gradual immune reaction that peaks around week 2 post-vaccination. Understanding these mechanisms is crucial for tailoring vaccine strategies to specific populations, such as the elderly or immunocompromised, who may require a particular type of immune stimulation.
Consider the role of adjuvants, substances added to vaccines to enhance immune response. For example, the shingles vaccine Shingrix contains a proprietary adjuvant system (AS01B) that amplifies both antibody and cellular immunity, making it over 90% effective in adults over 50. This is a stark contrast to earlier shingles vaccines like Zostavax, which lacked adjuvants and offered only 50-60% protection. Adjuvants can also modulate the type of immune response; aluminum salts, commonly used in vaccines like DTaP, primarily boost antibody production, while newer adjuvants like those in Shingrix stimulate a broader immune activation, including memory T-cells. This specificity in immune stimulation highlights why vaccine type matters in achieving optimal protection.
The route of administration further influences immune response. Intramuscular injections, standard for COVID-19 vaccines, deliver antigens directly to muscle tissue, where they are taken up by local immune cells, leading to systemic immunity. In contrast, oral vaccines like the rotavirus vaccine (Rotarix) stimulate mucosal immunity in the gut, producing IgA antibodies that prevent viral attachment to intestinal cells. This localized response is critical for protecting against pathogens that enter through mucosal surfaces. Similarly, intranasal vaccines, such as the FluMist influenza vaccine, induce both systemic and mucosal immunity, offering dual protection. The choice of administration route thus aligns the immune response with the pathogen’s entry point, underscoring the importance of vaccine type in targeted defense.
Practical considerations also arise when comparing vaccine types. Live-attenuated vaccines, like the MMR (measles, mumps, rubella), provide long-lasting immunity but are contraindicated in immunocompromised individuals due to the risk of viral replication. Inactivated vaccines, such as the injectable polio vaccine, are safer for this group but often require multiple doses and boosters to maintain immunity. For example, the hepatitis B vaccine (an inactivated type) typically requires a 3-dose series over 6 months, with antibody levels waning after 5-10 years, necessitating periodic titers and boosters for at-risk individuals. These differences emphasize the need to match vaccine type to both the pathogen and the recipient’s immune status, ensuring both safety and efficacy.
Finally, the concept of heterologous prime-boost strategies—using different vaccine types for initial and subsequent doses—illustrates how vaccine type can be leveraged to optimize immune response. Studies during the COVID-19 pandemic showed that combining an adenoviral vector vaccine (e.g., AstraZeneca) with an mRNA vaccine (e.g., Pfizer) for the second dose produced higher neutralizing antibody titers and broader T-cell responses compared to homologous regimens. This approach exploits the unique strengths of each vaccine platform, enhancing both the magnitude and diversity of immunity. Such innovations demonstrate that the type of vaccine not only matters but can be strategically combined to maximize protective outcomes, particularly in the face of evolving pathogens.
Protecting Health: The Critical Importance of MMR Vaccination
You may want to see also
Frequently asked questions
Yes, different types of vaccines (e.g., mRNA, viral vector, protein subunit) may have varying levels of effectiveness against specific diseases, but all approved vaccines meet rigorous safety and efficacy standards.
Yes, the type of vaccine can influence the type and severity of side effects. For example, mRNA vaccines like Pfizer and Moderna are more commonly associated with fatigue and muscle pain, while viral vector vaccines like Johnson & Johnson may cause more flu-like symptoms.
The duration of immunity can vary by vaccine type. Some vaccines, like mRNA vaccines, may require boosters sooner, while others, like inactivated vaccines, might provide longer-lasting immunity depending on the disease.
Yes, certain vaccines are recommended over others for specific populations. For example, mRNA vaccines are often preferred for pregnant individuals, while specific formulations may be tailored for children based on safety and efficacy data. Always consult healthcare providers for personalized advice.