The question of whether the polio vaccine prevents acute flaccid myelitis (AFM) has gained attention in recent years due to the rise in AFM cases, a rare but serious condition causing muscle weakness and paralysis. While the polio vaccine effectively protects against poliovirus, the exact cause of AFM remains unclear, with some cases potentially linked to non-polio enteroviruses. Although the polio vaccine does not directly target these other viruses, it plays a crucial role in preventing polio-related paralysis, which shares similarities with AFM symptoms. Researchers continue to investigate the relationship between the polio vaccine, AFM, and other viral triggers to better understand prevention strategies and public health implications.
| Characteristics | Values |
|---|---|
| Does Polio Vaccine Prevent AFM? | No direct evidence; polio vaccine does not specifically prevent Acute Flaccid Myelitis (AFM). |
| AFM Relationship to Polio | AFM is a rare but serious condition affecting the spinal cord, similar to polio in symptoms but not caused by the poliovirus. |
| Polio Vaccine Efficacy | Protects against poliovirus, which causes polio, but not against other viruses or pathogens linked to AFM. |
| Known Causes of AFM | Often associated with non-polio enteroviruses (e.g., EV-D68), but the exact cause remains unclear. |
| CDC Stance | The CDC states there is no evidence linking AFM to the polio vaccine or suggesting the vaccine prevents AFM. |
| Prevention of AFM | No specific vaccine for AFM; general preventive measures include avoiding mosquito bites and practicing good hygiene. |
| Research Status | Ongoing research to understand AFM causes and potential preventive measures, but no direct link to polio vaccination. |
| Public Health Advice | Continue polio vaccination to prevent polio, but it does not protect against AFM. |
Explore related products






What You'll Learn
- AFM and Polio Vaccine Link: Exploring potential connections between acute flaccid myelitis (AFM) and polio vaccination
- Vaccine Efficacy Against AFM: Investigating if the polio vaccine offers protection against AFM cases
- AFM Causes and Triggers: Identifying primary causes of AFM, including non-polio enteroviruses
- Vaccine Safety Concerns: Addressing public fears about polio vaccines causing AFM
- Scientific Studies and Data: Reviewing research on polio vaccines and AFM incidence rates
![]()
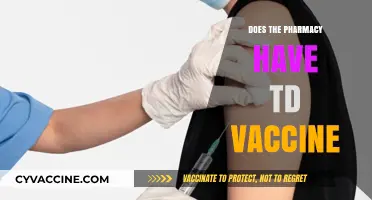
AFM and Polio Vaccine Link: Exploring potential connections between acute flaccid myelitis (AFM) and polio vaccination
Acute flaccid myelitis (AFM) is a rare but serious condition affecting the spinal cord, leading to muscle weakness and paralysis. Its symptoms resemble those of polio, raising questions about the role of the polio vaccine in preventing or, conversely, potentially triggering AFM. While the polio vaccine has eradicated paralytic polio in many regions, AFM cases have emerged as a modern concern, prompting investigations into their relationship. Understanding this link requires examining epidemiological data, vaccine mechanisms, and the broader context of viral infections.
From an analytical perspective, studies have explored whether the polio vaccine, particularly the inactivated polio vaccine (IPV), offers protection against AFM. IPV, administered in multiple doses starting at 2 months of age, targets the poliovirus but does not confer direct immunity to non-polio enteroviruses (NPEVs), which are often implicated in AFM cases. Research suggests that while IPV effectively prevents polio, its impact on AFM remains inconclusive. For instance, a 2018 CDC report found no direct causal link between IPV and AFM, but some experts hypothesize that the vaccine’s success in eliminating polio may have shifted the burden of paralytic illnesses to NPEVs. This highlights the complexity of attributing AFM cases to vaccination or other factors.
Instructively, parents and healthcare providers should remain vigilant about AFM symptoms, such as sudden limb weakness or facial drooping, especially in children under 5. While the polio vaccine does not explicitly prevent AFM, maintaining high vaccination rates is crucial to avoid polio resurgence, which could exacerbate paralytic conditions. Practical tips include adhering to the recommended IPV schedule (four doses by age 6) and monitoring for any unusual neurological symptoms post-vaccination. Reporting suspected AFM cases to health authorities aids in tracking and research efforts, ensuring a proactive approach to public health.
Persuasively, the absence of a direct link between the polio vaccine and AFM should not deter vaccination efforts. The polio vaccine’s success in eradicating a once-devastating disease underscores its importance. Instead, the focus should shift to identifying the true causes of AFM, such as NPEV infections or environmental triggers. Investing in research to develop broader-spectrum vaccines or antiviral treatments could address both polio and AFM, offering a more comprehensive solution. Until then, the polio vaccine remains a vital tool in preventing paralytic diseases, even if its role in AFM is limited.
Comparatively, the relationship between AFM and the polio vaccine mirrors broader challenges in vaccine science. Just as the measles vaccine does not prevent all viral encephalitides, the polio vaccine does not shield against all causes of flaccid paralysis. This underscores the need for nuanced public health messaging, avoiding oversimplification while emphasizing proven benefits. By acknowledging the vaccine’s limitations in AFM prevention, health authorities can build trust and focus on evidence-based strategies to combat emerging neurological conditions.
Meningitis B Vaccine: US Release Date and Impact
You may want to see also
Explore related products






![]()
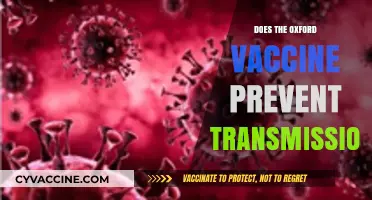
Vaccine Efficacy Against AFM: Investigating if the polio vaccine offers protection against AFM cases
Acute flaccid myelitis (AFM), a rare but serious condition affecting the nervous system, has sparked debates about its relationship with poliovirus and the polio vaccine. While AFM shares symptoms with polio—such as limb weakness and paralysis—its causes remain less understood. One critical question emerges: Can the polio vaccine, which has eradicated polio in most regions, also protect against AFM? This inquiry is particularly urgent given AFM’s sudden rise in cases since 2014, primarily among children under 5. Understanding the polio vaccine’s role in AFM prevention requires examining its mechanism, efficacy, and potential limitations.
The polio vaccine, available in two forms—the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV)—targets the poliovirus, a known cause of paralysis. IPV, administered as an injection, is widely used in developed countries due to its safety and efficacy. OPV, delivered orally, confers gut immunity but carries a rare risk of vaccine-derived poliovirus. Both vaccines have successfully eliminated wild poliovirus in most countries, but their impact on AFM is less clear. Studies suggest AFM may be linked to non-polio enteroviruses, particularly EV-D68 and EV-A71, raising questions about whether the polio vaccine’s cross-protection extends to these pathogens.
Investigating the polio vaccine’s efficacy against AFM involves analyzing epidemiological data and immunological responses. A 2019 study in *The Lancet* found no significant association between polio vaccination rates and AFM incidence, suggesting the vaccine may not prevent AFM. However, another study in *Vaccine* highlighted that IPV could potentially reduce the severity of AFM cases by boosting overall immune responses. Practical considerations include ensuring complete vaccination schedules—typically four doses of IPV starting at 2 months of age—to maximize protection against poliovirus and possibly mitigate AFM risks. Parents and healthcare providers should remain vigilant for AFM symptoms, such as sudden limb weakness or facial droop, even in vaccinated children.
A comparative analysis of AFM outbreaks in vaccinated and unvaccinated populations could provide clearer insights. For instance, regions with high polio vaccination coverage but persistent AFM cases, like the United States, indicate that the vaccine’s protective effect against AFM is limited. Conversely, areas with low vaccination rates and higher AFM incidence might suggest indirect benefits of herd immunity. However, such comparisons must account for confounding factors, including exposure to non-polio enteroviruses and environmental triggers. Until definitive evidence emerges, public health strategies should focus on surveillance, early diagnosis, and supportive care for AFM patients.
Persuasively, while the polio vaccine remains a cornerstone of global health, its role in AFM prevention is not yet established. Ongoing research, including clinical trials and serological studies, is essential to determine whether modifying vaccine formulations or developing new vaccines could address AFM. In the interim, healthcare professionals should educate communities about AFM risks, emphasize the importance of polio vaccination for its primary purpose, and advocate for continued investment in infectious disease research. The quest to understand AFM underscores the complexity of vaccine efficacy and the need for tailored public health responses.
Australia's Vaccine Rollout: Why the March Delay Explained
You may want to see also
Explore related products





![]()
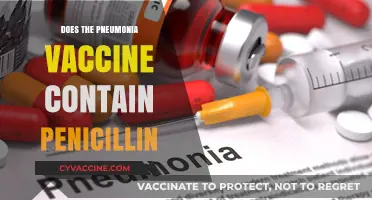
AFM Causes and Triggers: Identifying primary causes of AFM, including non-polio enteroviruses
Acute flaccid myelitis (AFM) is a rare but serious condition that affects the nervous system, particularly the spinal cord, leading to muscle weakness and paralysis. While the exact causes of AFM remain under investigation, a growing body of evidence points to non-polio enteroviruses, especially enterovirus D68 (EV-D68), as primary triggers. Unlike polio, which is caused by the poliovirus and effectively prevented by the polio vaccine, AFM’s association with non-polio enteroviruses means the polio vaccine does not protect against it. This distinction is critical for understanding prevention strategies and public health responses.
Non-polio enteroviruses are common and typically cause mild symptoms like fever, runny nose, and cough, particularly in children. However, in rare cases, these viruses can lead to severe complications, including AFM. EV-D68, in particular, has been strongly linked to AFM outbreaks in the United States since 2014, often occurring in biennial cycles. The virus spreads through respiratory droplets, making it highly contagious in settings like schools and daycare centers. While most infections are asymptomatic or mild, the risk of AFM underscores the need for vigilance, especially in children under 5 years old, who are most vulnerable.
Identifying the role of non-polio enteroviruses in AFM has shifted the focus from vaccination to infection control measures. Unlike polio, which has been nearly eradicated globally due to widespread vaccination, non-polio enteroviruses lack a specific vaccine. Instead, prevention relies on hygiene practices such as frequent handwashing, avoiding close contact with sick individuals, and disinfecting surfaces. Parents and caregivers should monitor children for sudden weakness in the arms or legs, difficulty moving the face, or trouble swallowing, as these are hallmark symptoms of AFM requiring immediate medical attention.
The relationship between non-polio enteroviruses and AFM also highlights gaps in our understanding of viral pathogenesis. Researchers are exploring why only a small fraction of enterovirus infections progress to AFM and whether genetic or immunological factors play a role. This knowledge could inform targeted therapies or preventive measures in the future. For now, public health efforts must balance awareness with reassurance, as the risk of AFM remains low compared to the prevalence of enterovirus infections.
In summary, while the polio vaccine has been a triumph in disease prevention, it does not protect against AFM, which is primarily linked to non-polio enteroviruses like EV-D68. Prevention hinges on reducing exposure to these viruses through hygiene and early recognition of symptoms. As research continues, understanding the unique triggers of AFM is essential for developing effective strategies to combat this rare but devastating condition.
Understanding the Purpose of a Vaccine: A Doctor's Insight
You may want to see also
![]()
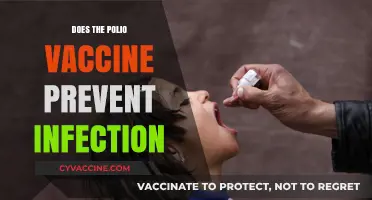
Vaccine Safety Concerns: Addressing public fears about polio vaccines causing AFM
The public's trust in vaccines is a cornerstone of global health, yet fears and misconceptions can erode this trust, leading to dangerous consequences. One such concern that has emerged in recent years is the alleged link between the polio vaccine and acute flaccid myelitis (AFM), a rare but serious condition affecting the nervous system. This fear, though unfounded, has sparked anxiety among parents and caregivers, prompting a critical need for clear, evidence-based communication.
Debunking the Myth: A Scientific Perspective
Scientific research unequivocally refutes the claim that the polio vaccine causes AFM. The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) have extensively studied this issue, finding no causal relationship. In fact, the inactivated poliovirus vaccine (IPV), the only polio vaccine used in the US since 2000, is highly effective in preventing polio without increasing the risk of AFM. A 2019 study published in the *Journal of Infectious Diseases* analyzed over 1.7 million vaccine doses and found no association between IPV and AFM. This evidence underscores the importance of relying on peer-reviewed research rather than anecdotal reports or misinformation.
Addressing Public Fears: A Practical Approach
To alleviate concerns, healthcare providers must engage in transparent, empathetic communication. Start by acknowledging the fear as valid, then gently correct misconceptions with factual information. For instance, explain that AFM is likely caused by non-polio enteroviruses, particularly EV-D68, and that the polio vaccine protects against a different virus entirely. Provide concrete examples, such as the near-eradication of polio globally due to vaccination campaigns, to build trust. Additionally, emphasize the rigorous testing and monitoring vaccines undergo before approval, including ongoing surveillance for adverse effects.
Empowering Parents with Knowledge
Parents often feel overwhelmed by conflicting information, so equipping them with reliable resources is key. Direct them to trusted sources like the CDC, WHO, or their pediatrician’s office for accurate data. Encourage questions and offer age-appropriate explanations for children, such as, "The polio vaccine is like a shield that protects your body from a very bad virus." For older children, discuss the history of polio and its devastating effects before vaccines were available. Practical tips, such as scheduling vaccine appointments during calm times of day and bringing a comfort item, can also ease anxiety.
Strengthening Community Trust
Community engagement plays a vital role in dispelling vaccine myths. Host town hall meetings, webinars, or social media campaigns featuring local healthcare providers, scientists, and families who have benefited from vaccination. Share personal stories of polio survivors or AFM patients to humanize the issue. Collaborate with schools and community centers to distribute educational materials in multiple languages, ensuring accessibility. By fostering a dialogue rooted in empathy and evidence, we can rebuild trust and protect public health.
Moving Forward: A Call to Action
Addressing vaccine safety concerns requires a collective effort. Policymakers must invest in public health education and combat misinformation through legislation and media literacy programs. Healthcare providers should prioritize ongoing training in communication skills and vaccine science. Parents and caregivers, armed with knowledge, can advocate for their communities and model informed decision-making. Together, we can ensure that fear does not overshadow the life-saving power of vaccines, safeguarding current and future generations from preventable diseases.
Ring Vaccination vs. Herd Immunity: Understanding Key Differences in Disease Control
You may want to see also
![]()
Scientific Studies and Data: Reviewing research on polio vaccines and AFM incidence rates
The relationship between polio vaccines and acute flaccid myelitis (AFM) has sparked intense scientific inquiry, with researchers dissecting data to determine if the vaccine might offer protective benefits against this rare but serious condition. Studies have explored whether the inactivated polio vaccine (IPV) or the oral polio vaccine (OPV) could influence AFM incidence rates, given their distinct mechanisms of action. For instance, IPV, administered as part of routine childhood immunizations (typically at 2, 4, and 6–18 months), provides systemic immunity without the risk of vaccine-derived poliovirus (VDPV) associated with OPV. This distinction is critical, as VDPV has been hypothesized to play a role in AFM cases, particularly in regions where OPV is still used.
Analyzing epidemiological trends reveals a complex interplay between polio vaccination strategies and AFM occurrence. A 2018 CDC investigation found that AFM cases peaked in the United States during OPV phase-out periods, raising questions about whether the transition to IPV alone might inadvertently increase susceptibility to non-polio enteroviruses, such as EV-D68, which is strongly linked to AFM. However, definitive causation remains elusive. For example, a 2021 study published in *The Lancet* compared AFM incidence in countries using IPV versus OPV, finding no statistically significant difference in rates, though sample size limitations and regional variability complicate interpretation.
Instructively, healthcare providers should remain vigilant for AFM symptoms—sudden limb weakness, facial droop, and difficulty swallowing—particularly during peak enterovirus seasons (late summer to early fall). While no direct preventive measure for AFM exists, ensuring complete polio vaccination (three doses of IPV followed by a booster at 4–6 years) remains critical. Parents should be counseled that IPV’s proven efficacy against poliomyelitis far outweighs speculative concerns about AFM, especially given the latter’s rarity (approximately 1–2 cases per million children).
Comparatively, the debate mirrors broader discussions on vaccine-preventable diseases and emerging conditions. Just as the measles vaccine does not prevent all encephalitis cases, polio vaccines do not claim to shield against AFM. Yet, their role in eradicating poliovirus—a historically devastating pathogen—cannot be overstated. A 2019 WHO report highlighted that countries maintaining high IPV coverage (above 90%) saw fewer AFM clusters, though confounding factors like healthcare infrastructure and surveillance quality must be considered.
Practically, public health campaigns should emphasize the dual benefits of polio vaccination: direct protection against poliomyelitis and potential indirect effects on AFM risk reduction. For travelers to OPV-using regions, the CDC recommends a single lifetime IPV booster dose for adults, balancing immunity with VDPV exposure risks. Ultimately, while research continues, the evidence underscores that polio vaccines remain a cornerstone of global health, with their impact on AFM likely secondary to broader immunological and epidemiological dynamics.
Does the Meningococcal Conjugate Vaccine Cause Pain? What to Expect
You may want to see also
Frequently asked questions
There is no definitive evidence that the polio vaccine prevents AFM, as AFM is not caused by the poliovirus. However, the polio vaccine protects against poliovirus, which can cause similar symptoms to AFM.
No, AFM is not caused by the poliovirus. While AFM has similarities to polio, its exact cause is often unknown, though it is believed to be linked to non-polio enteroviruses, particularly EV-D68.
The polio vaccine does not directly reduce the risk of AFM since AFM is not caused by the poliovirus. However, vaccination against polio is still crucial to prevent polio-related paralysis.
No, the polio vaccine does not protect against AFM. AFM is a separate condition with different causes, and its prevention strategies are still under investigation.
This misconception arises because AFM and polio share similar symptoms, such as limb weakness and paralysis. However, they are distinct conditions with different causes, and the polio vaccine does not target the viruses associated with AFM.