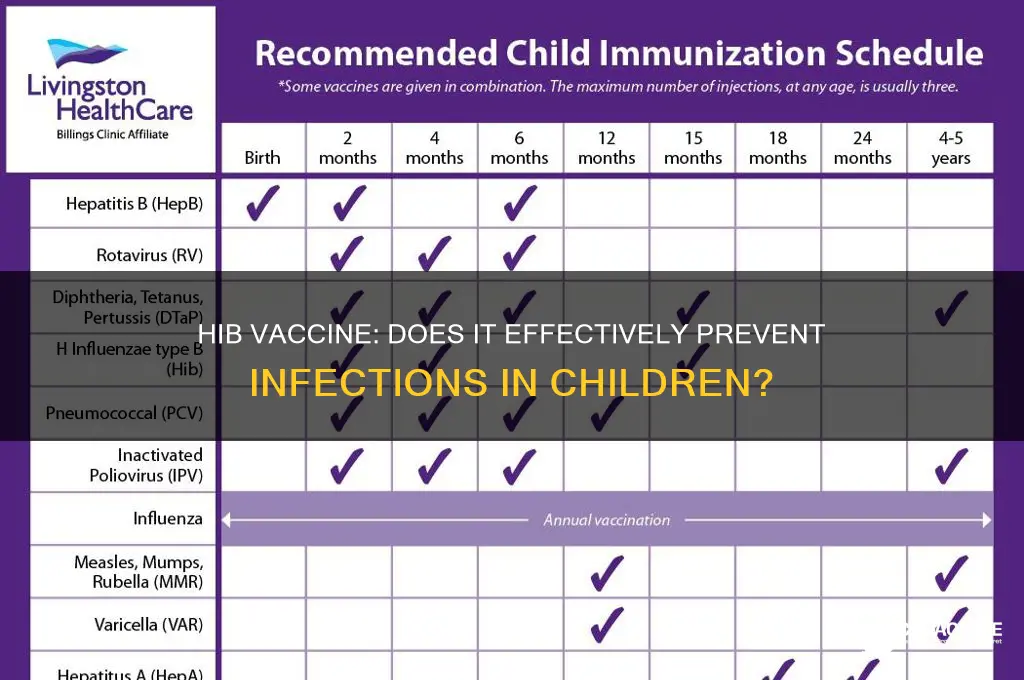
The Hib vaccine, designed to protect against *Haemophilus influenzae* type b (Hib), a bacterium that can cause severe infections such as meningitis, pneumonia, and epiglottitis, is a cornerstone of childhood immunization programs worldwide. While the vaccine is highly effective in preventing invasive Hib diseases, its ability to prevent all forms of Hib infection remains a topic of interest. Studies have shown that the Hib vaccine significantly reduces the incidence of serious Hib-related illnesses, particularly in young children who are most vulnerable. However, it may not entirely eliminate the risk of asymptomatic or mild infections, as the bacterium can still colonize the nasopharynx without causing disease. Understanding the vaccine’s limitations and its role in preventing severe outcomes is crucial for public health strategies and informed decision-making.
| Characteristics | Values |
|---|---|
| Vaccine Name | Haemophilus influenzae type b (Hib) vaccine |
| Primary Purpose | Prevents invasive Hib diseases such as meningitis, pneumonia, and epiglottitis |
| Effectiveness in Preventing Infection | Reduces Hib disease incidence by 95-100% in vaccinated populations |
| Effect on Asymptomatic Carriage | Does not significantly reduce Hib colonization in the nasopharynx |
| Herd Immunity Effect | Reduces disease incidence in both vaccinated and unvaccinated individuals |
| Duration of Protection | Long-lasting immunity after completion of the primary vaccine series |
| Target Population | Infants and young children (primary focus), with catch-up vaccination for older children in some regions |
| Vaccine Types | Conjugate vaccines (e.g., PRP-T, PRP-OMP, PRP-D, HbOC) |
| Dosing Schedule | Typically 2-3 doses in infancy, with a booster dose in the second year of life |
| Side Effects | Generally mild (e.g., fever, irritability, injection site reactions) |
| Global Impact | Near elimination of Hib diseases in countries with high vaccination coverage |
| WHO Recommendation | Included in the routine immunization schedule for all infants |
| Limitations | Does not protect against non-type b strains of Haemophilus influenzae |
| Latest Data (as of 2023) | Sustained low incidence of Hib diseases in vaccinated populations |
Explore related products






What You'll Learn
![]()
Hib vaccine effectiveness in infants
The Hib vaccine has been a cornerstone in preventing invasive Haemophilus influenzae type b (Hib) diseases, such as meningitis and pneumonia, in infants since its introduction in the 1990s. Clinical trials and real-world data consistently show that the vaccine is highly effective, reducing Hib-related diseases by over 95% in vaccinated populations. Infants, who are particularly vulnerable to Hib infections due to their developing immune systems, receive the vaccine in a series of doses starting at 2 months of age, followed by boosters at 4 months and 6 months, with a final dose between 12 and 15 months. This schedule ensures robust immunity during the critical early years of life.
While the Hib vaccine is remarkably effective in preventing invasive diseases, it does not entirely eliminate the possibility of Hib colonization in the nasopharynx. This means vaccinated infants can still carry the bacteria without developing symptoms, though they are far less likely to progress to severe infections. Studies indicate that the vaccine’s efficacy in preventing meningitis, for instance, is approximately 94–100%, depending on the region and vaccine formulation. However, its impact on reducing overall Hib transmission in communities is equally significant, as vaccinated individuals are less likely to spread the bacteria to others.
One critical aspect of the Hib vaccine’s effectiveness is its ability to induce immunological memory, ensuring long-term protection. Infants who complete the full vaccination series develop antibodies that persist for years, reducing the need for frequent boosters. However, timely adherence to the vaccination schedule is essential. Delayed doses can leave infants susceptible during the window when they are most at risk. Parents and caregivers should consult healthcare providers to ensure their child receives the vaccine at the recommended ages: 2, 4, 6, and 12–15 months, with slight variations depending on the specific vaccine brand.
Comparatively, the Hib vaccine’s success in infants stands out when contrasted with other childhood vaccines. Unlike some vaccines that require annual boosters, the Hib vaccine provides durable immunity with just a few doses. Its introduction has led to a dramatic decline in Hib-related hospitalizations and deaths globally, making it a public health triumph. For example, in the United States, Hib meningitis cases in children under 5 dropped from 20,000 annually in the pre-vaccine era to fewer than 100 cases per year post-vaccination. This underscores the vaccine’s transformative impact on infant health.
Practical tips for parents include ensuring infants receive all doses on time, monitoring for mild side effects like fever or soreness at the injection site, and staying informed about local vaccination programs. While rare, severe allergic reactions can occur, so caregivers should be aware of symptoms like difficulty breathing or swelling. The Hib vaccine is often administered in combination with other vaccines (e.g., DTaP, IPV) to streamline the immunization process, reducing the number of injections needed. This approach not only enhances convenience but also improves overall vaccine uptake, further protecting infants from preventable diseases.
Strong Vaccine Reactions: What They Mean for Your Immune Response
You may want to see also
Explore related products





![]()
Prevention of Hib meningitis cases
The Hib vaccine has been a game-changer in the fight against Haemophilus influenzae type b (Hib) infections, particularly in preventing Hib meningitis, a severe and potentially life-threatening condition. Before the vaccine’s introduction in the 1990s, Hib was the leading cause of bacterial meningitis in children under 5, with devastating consequences. Today, the vaccine’s impact is undeniable: in countries with high vaccination rates, Hib meningitis cases have plummeted by over 95%. This dramatic reduction underscores the vaccine’s efficacy in not just preventing infection but specifically targeting the most severe outcomes.
Administering the Hib vaccine according to recommended schedules is critical for maximizing protection. In the U.S., the CDC advises a series of doses starting at 2 months of age, with additional shots at 4 months, 6 months (depending on the brand), and a booster at 12–15 months. This regimen ensures robust immunity during the period when children are most vulnerable. For example, the ActHIB vaccine requires three primary doses at 2, 4, and 6 months, followed by a booster, while PedvaxHIB is given in two doses at 2 and 4 months, plus a booster. Adhering to these schedules is essential, as incomplete vaccination leaves children at higher risk for Hib meningitis.
While the Hib vaccine is highly effective, it’s not a standalone solution. Parents and caregivers must remain vigilant for symptoms of Hib meningitis, such as fever, severe headache, neck stiffness, and irritability, especially in unvaccinated or partially vaccinated children. Early diagnosis and treatment with antibiotics are crucial for preventing long-term complications like hearing loss, developmental delays, or death. Combining vaccination with awareness ensures a comprehensive approach to prevention, particularly in regions with lower vaccine coverage or emerging Hib strains.
Comparatively, the success of the Hib vaccine in preventing meningitis highlights the importance of global vaccination efforts. In low-income countries where vaccine access remains a challenge, Hib meningitis persists as a significant public health threat. Initiatives like Gavi, the Vaccine Alliance, have played a pivotal role in expanding access, but disparities remain. For instance, while high-income countries have nearly eradicated Hib meningitis, some African nations still report incidence rates of up to 70 cases per 100,000 children annually. Bridging this gap requires sustained investment in vaccine distribution, healthcare infrastructure, and community education.
In conclusion, the Hib vaccine stands as a cornerstone in preventing Hib meningitis, offering unparalleled protection when administered correctly. However, its full potential can only be realized through strict adherence to dosing schedules, global equity in vaccine access, and continued surveillance of Hib strains. By combining these strategies, we can further reduce the burden of this preventable disease and safeguard the health of future generations.
Live Virus Vaccines: Which Shots Contain Weakened Pathogens?
You may want to see also
Explore related products






![]()
Impact on pneumonia incidence rates
The introduction of the Hib vaccine has significantly altered the landscape of pneumonia incidence rates, particularly among children under five years old. Before the vaccine's widespread use, *Haemophilus influenzae* type b (Hib) was a leading cause of bacterial pneumonia in this age group, accounting for up to 20% of cases in some regions. Post-vaccination data reveals a dramatic decline: studies in developed countries show a 60-80% reduction in Hib-related pneumonia cases within a decade of vaccine implementation. This shift underscores the vaccine’s direct impact on preventing not just meningitis and epiglottitis, but also pneumonia, a major contributor to childhood mortality globally.
Consider the mechanism: the Hib vaccine primes the immune system to recognize and neutralize the polysaccharide capsule of the Hib bacterium, preventing it from colonizing the respiratory tract. For optimal protection, the World Health Organization (WHO) recommends a 2- or 3-dose primary series for infants, starting at 6 weeks of age, followed by a booster dose at 12-15 months. Adherence to this schedule is critical, as partial vaccination may leave children susceptible to infection, particularly in settings with high disease prevalence. In low-resource areas, where pneumonia remains a leading cause of death, the Hib vaccine’s inclusion in routine immunization programs has been a game-changer, reducing the overall pneumonia burden and easing the strain on healthcare systems.
A comparative analysis highlights the vaccine’s broader implications. In countries like the United States and the United Kingdom, where Hib vaccination has been routine since the early 1990s, pneumonia incidence rates have plummeted, with Hib-specific cases becoming rare. Contrast this with regions where vaccine coverage is inconsistent, such as parts of sub-Saharan Africa and Southeast Asia, where Hib remains a significant pneumonia pathogen. This disparity emphasizes the need for equitable vaccine distribution and strengthened healthcare infrastructure to maximize the vaccine’s impact. For parents and caregivers, ensuring timely vaccination is a practical step to protect children from this preventable cause of pneumonia.
Finally, the Hib vaccine’s role in reducing pneumonia incidence extends beyond direct prevention. By lowering the prevalence of Hib infections, the vaccine indirectly reduces the risk of secondary complications, such as pneumococcal pneumonia, which often co-occurs with Hib disease. This synergistic effect amplifies the vaccine’s public health value, making it a cornerstone of pneumonia prevention strategies. For healthcare providers, integrating Hib vaccination into broader pneumonia prevention campaigns—including promoting breastfeeding, reducing indoor air pollution, and encouraging timely treatment of respiratory infections—can further enhance outcomes. In the fight against pneumonia, the Hib vaccine is not just a tool; it’s a transformative intervention with far-reaching benefits.
Was There a Vaccine for the Last Pandemic? Uncovering the Truth
You may want to see also
Explore related products





![]()
Vaccine efficacy in high-risk groups
High-risk groups, such as infants, young children, and individuals with compromised immune systems, are particularly vulnerable to *Haemophilus influenzae* type b (Hib) infections. The Hib vaccine’s efficacy in these populations is critical, as they face higher risks of severe complications like meningitis and pneumonia. Studies show that the vaccine provides robust protection, with efficacy rates exceeding 95% in healthy infants who complete the recommended series. For high-risk groups, however, factors like immunodeficiency or underlying conditions can reduce this efficacy, making timely and complete vaccination even more essential.
For infants, the Hib vaccine is typically administered in a 2- or 3-dose series starting at 2 months of age, followed by a booster at 12–15 months. Premature infants, who are at increased risk due to underdeveloped immune systems, should follow the same schedule, as the vaccine’s immunogenicity remains effective in this population. Children with sickle cell disease or asplenia, who are at heightened risk of invasive Hib disease, may require additional doses or closer monitoring to ensure adequate protection. Adhering to the recommended schedule is non-negotiable for these groups, as delays can leave them exposed during critical developmental stages.
In immunocompromised individuals, such as those with HIV or undergoing chemotherapy, the Hib vaccine’s efficacy may wane due to reduced immune responses. For these groups, a higher-dose regimen or more frequent boosters may be considered, though evidence is limited. Practical tips include ensuring these individuals receive the vaccine during periods of optimal immune function, if possible, and coordinating with healthcare providers to assess antibody levels post-vaccination. Despite potential limitations, the vaccine remains a vital tool in reducing infection risk in this vulnerable population.
Comparatively, the Hib vaccine’s performance in high-risk groups underscores the importance of tailored vaccination strategies. While it may not achieve the same efficacy as in healthy individuals, it significantly lowers the incidence of severe disease. For example, in children with HIV, the vaccine reduces the risk of invasive Hib disease by approximately 80%, a substantial benefit despite being lower than the general population. This highlights the need for public health initiatives to prioritize these groups, ensuring equitable access to vaccination and follow-up care.
In conclusion, while the Hib vaccine is highly effective in preventing infection, its efficacy in high-risk groups requires careful consideration of individual health status and vaccination protocols. By adhering to age-specific schedules, exploring dose adjustments, and monitoring immune responses, healthcare providers can maximize protection for those most at risk. This targeted approach not only safeguards vulnerable populations but also contributes to broader herd immunity, reducing the overall burden of Hib disease.
Global Vaccine Rollout: Tracking Worldwide Administration Numbers and Impact
You may want to see also
Explore related products






![]()
Duration of Hib immunity post-vaccination
The Hib vaccine, a cornerstone of childhood immunization, significantly reduces the risk of invasive Haemophilus influenzae type b (Hib) diseases such as meningitis and pneumonia. However, the duration of immunity post-vaccination is a critical factor in its effectiveness. Studies indicate that the Hib vaccine provides robust protection for at least 5 to 10 years after the completion of the primary series, typically administered in infancy. This duration is supported by serological data showing sustained antibody levels in vaccinated individuals during this period. For children who receive the full course—usually three or four doses depending on the vaccine brand—the immune memory established is sufficient to prevent severe infections, even if antibody levels wane over time.
Booster doses are generally not recommended for healthy children after the primary series, as the initial vaccination confers long-lasting immunity. However, certain populations, such as those with asplenia or immunocompromising conditions, may require additional doses to maintain protective antibody levels. For example, children with sickle cell disease or those undergoing chemotherapy may need a booster dose to ensure continued protection. This tailored approach underscores the importance of considering individual health status when assessing the duration of Hib immunity.
Comparatively, the Hib vaccine’s immunity duration contrasts with other vaccines like the flu shot, which requires annual administration due to viral mutation and waning immunity. The Hib vaccine’s success in providing extended protection highlights its role in reducing disease burden globally. In countries with high vaccination coverage, Hib diseases have become rare, demonstrating the vaccine’s ability to confer long-term immunity at a population level. This sustained protection is a testament to the vaccine’s design and the immune system’s robust response to it.
Practical considerations for parents and healthcare providers include ensuring timely completion of the primary series, typically starting at 2 months of age. Delayed or missed doses can compromise immunity, so adherence to the recommended schedule is crucial. Additionally, monitoring antibody levels in at-risk individuals can help identify those who may need additional doses. While the Hib vaccine does not provide lifelong immunity, its decade-long protection is a significant public health achievement, reducing the need for frequent revaccination and minimizing disease outbreaks.
In summary, the Hib vaccine offers durable immunity for 5 to 10 years post-vaccination, effectively preventing severe infections in most recipients. While boosters are rarely needed for healthy individuals, specific populations may require additional doses. Understanding the duration of immunity and adhering to vaccination schedules are key to maximizing the vaccine’s impact. This long-term protection underscores the Hib vaccine’s role as a vital tool in global health, safeguarding children from life-threatening diseases.
Maryland's Vaccination Progress: Adult Coverage Rates and Insights
You may want to see also
Frequently asked questions
The Hib vaccine is highly effective in preventing invasive Hib diseases such as meningitis and pneumonia, but it does not guarantee 100% protection against all Hib infections. It significantly reduces the risk, especially in young children who are most vulnerable.
While rare, it is possible for a vaccinated child to still get a Hib infection. However, the vaccine greatly lowers the likelihood of severe complications and reduces the overall incidence of Hib-related illnesses.
The Hib vaccine specifically targets *Haemophilus influenzae* type b (Hib), which is the most common cause of severe infections. It does not protect against other types of *H. influenzae* (such as types a, c, d, or f), but Hib is responsible for the majority of serious cases in unvaccinated populations.