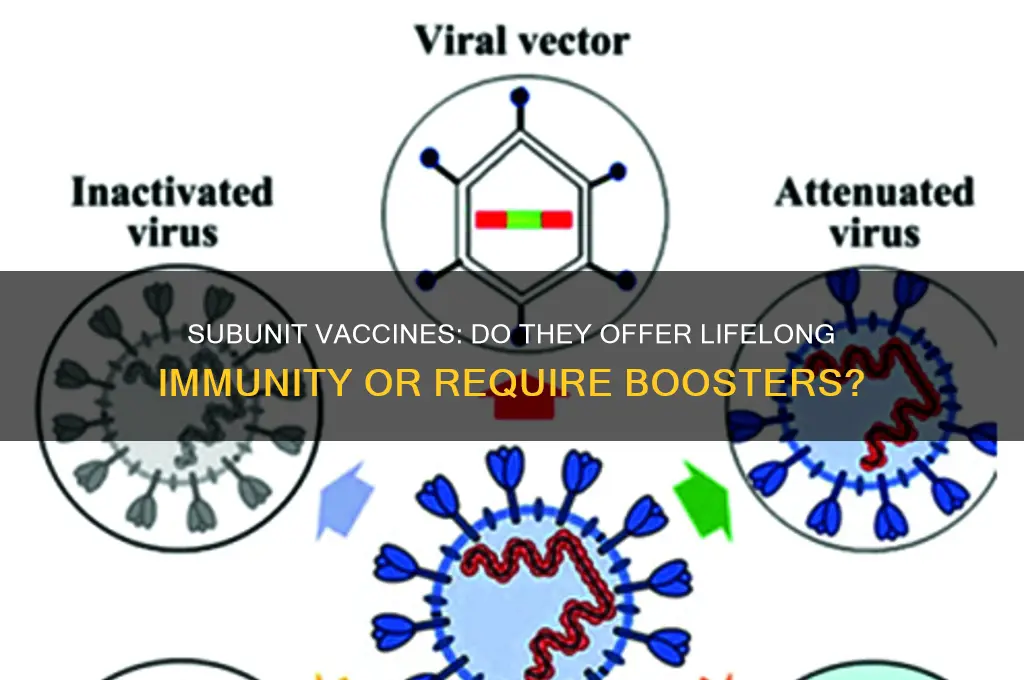
Subunit vaccines, which contain specific fragments of a pathogen rather than the entire organism, have gained attention for their targeted approach and safety profile. However, a common question arises regarding their ability to provide lifetime protection. Unlike live-attenuated or inactivated vaccines, subunit vaccines typically elicit a more focused immune response, which may not always result in long-lasting immunity. While they can offer robust protection for several years, booster doses are often required to maintain immunity, especially against rapidly evolving pathogens like influenza or SARS-CoV-2. Research continues to explore advancements in adjuvants and delivery systems to enhance the durability of subunit vaccines, but as of now, they generally do not provide lifetime protection without periodic reinforcement.
| Characteristics | Values |
|---|---|
| Lifetime Protection | Subunit vaccines generally do not provide lifetime protection. |
| Duration of Immunity | Protection typically lasts for several years, varying by vaccine type. |
| Booster Requirements | Boosters are often needed to maintain immunity over time. |
| Immune Response | Elicits a targeted immune response to specific antigens. |
| Safety Profile | Generally safer due to absence of live or whole pathogens. |
| Examples | Hepatitis B, HPV, COVID-19 (e.g., Novavax) vaccines. |
| Adjuvant Use | Often require adjuvants to enhance immune response. |
| Storage Requirements | Typically stable and easier to store compared to live vaccines. |
| Efficacy | High efficacy but may wane over time, necessitating boosters. |
| Side Effects | Mild to moderate side effects, such as soreness or fatigue. |
| Development Time | Faster to develop compared to live-attenuated or whole-cell vaccines. |
| Cost | Generally more expensive due to complex manufacturing processes. |
| Population Suitability | Suitable for immunocompromised individuals due to safety profile. |
| Antigen Specificity | Contains only specific antigens, not the entire pathogen. |
| Global Accessibility | Accessibility varies by region and healthcare infrastructure. |
| Research and Development | Ongoing research to improve duration of protection and reduce booster need. |
Explore related products






What You'll Learn
- Immune Memory Formation: How subunit vaccines stimulate long-term immune memory for potential lifelong protection
- Booster Requirements: Whether periodic boosters are needed to maintain immunity over time
- Antigen Stability: Role of stable antigens in subunit vaccines for sustained immune response
- Individual Variability: How age, health, and genetics affect lifelong protection from subunit vaccines
- Emerging Variants: Impact of pathogen mutations on the longevity of subunit vaccine protection
![]()
Immune Memory Formation: How subunit vaccines stimulate long-term immune memory for potential lifelong protection
Subunit vaccines, unlike live-attenuated or whole-pathogen vaccines, contain only specific fragments of a pathogen—such as proteins or polysaccharides—designed to trigger a targeted immune response. This precision engineering raises a critical question: Can these minimal components stimulate immune memory robust enough for lifelong protection? The answer lies in understanding how subunit vaccines interact with the immune system to form long-term memory cells.
Mechanisms of Immune Memory Formation
Subunit vaccines excel at priming the adaptive immune system by presenting antigenic components to antigen-presenting cells (APCs), which then activate T cells and B cells. B cells differentiate into plasma cells, producing antibodies, while a subset of B cells and T cells become memory cells. These memory cells persist in the body, ready to mount a rapid and robust response upon re-exposure to the pathogen. Unlike whole-pathogen vaccines, subunit vaccines often require adjuvants—substances like aluminum salts or lipid nanoparticles—to enhance immune activation and memory formation. For example, the hepatitis B vaccine, a recombinant subunit vaccine, achieves seroprotection in 95% of recipients after a 3-dose series, with studies showing immune memory lasting over 30 years in many individuals.
Comparative Analysis with Other Vaccine Types
While live-attenuated vaccines, such as the measles-mumps-rubella (MMR) vaccine, often confer lifelong immunity after one or two doses, subunit vaccines typically require multiple doses to build sufficient immune memory. This is because subunit vaccines present fewer immunogenic components, necessitating repeated exposure to ensure memory cell maturation. However, their safety profile—low risk of adverse reactions due to the absence of live pathogens—makes them ideal for vulnerable populations, such as the elderly or immunocompromised. For instance, the acellular pertussis vaccine (a subunit vaccine) requires a 5-dose series in children (2, 4, 6, 15–18 months, and 4–6 years) to establish durable immunity, though boosters are recommended every 10 years due to waning efficacy.
Practical Considerations for Long-Term Protection
To maximize the potential for lifelong protection, subunit vaccines must be administered according to precise schedules. For adults, the shingles vaccine (Shingrix), a subunit vaccine containing glycoprotein E and an adjuvant, requires two doses 2–6 months apart, achieving over 90% efficacy for at least 7 years. Adherence to dosing intervals is critical, as deviations can reduce immune memory formation. Additionally, combining subunit vaccines with novel adjuvants or delivery systems, such as mRNA technology, holds promise for enhancing memory responses. For example, mRNA-based subunit vaccines against respiratory syncytial virus (RSV) are in development, aiming to provide durable protection in older adults with a single dose.
Challenges and Future Directions
Despite their potential, subunit vaccines face challenges in achieving lifelong immunity. Pathogens with high mutation rates, like influenza, require frequent updates to subunit vaccine formulations, limiting long-term efficacy. Moreover, individual variability in immune responses—influenced by age, genetics, and comorbidities—can affect memory cell formation. Research into personalized vaccination strategies and next-generation adjuvants may address these limitations. For instance, a universal influenza vaccine targeting conserved viral proteins could provide broader and more enduring protection than current seasonal vaccines.
In summary, subunit vaccines stimulate immune memory through precise antigen presentation and adjuvant-enhanced activation, offering potential for lifelong protection in some cases. While challenges remain, advancements in vaccine design and delivery systems are paving the way for more durable immunity, particularly for vulnerable populations. Adherence to dosing schedules and ongoing research will be key to unlocking the full potential of subunit vaccines in immune memory formation.
The Evolution of Childhood Vaccinations in the UK: A Historical Overview
You may want to see also
Explore related products






![]()
Booster Requirements: Whether periodic boosters are needed to maintain immunity over time
Subunit vaccines, which contain only specific fragments of a pathogen, are designed to elicit a targeted immune response. Unlike live-attenuated or inactivated vaccines, they typically induce a more focused but potentially less durable immunity. This raises a critical question: how long does protection last, and are periodic boosters necessary? The answer varies depending on the vaccine and the pathogen it targets. For instance, the hepatitis B vaccine, a well-known subunit vaccine, provides long-lasting immunity in most individuals after a 3-dose series, often eliminating the need for boosters. However, this is not a universal rule, as other subunit vaccines, like the acellular pertussis vaccine (DTaP), show waning immunity over 5–10 years, necessitating booster doses.
To determine booster requirements, public health officials analyze immune response data, including antibody levels and real-world efficacy. For example, the COVID-19 subunit vaccines (e.g., Novavax) have demonstrated robust initial protection but face challenges from evolving variants. Studies suggest that immunity wanes after 6–12 months, prompting recommendations for boosters, particularly for vulnerable populations like the elderly or immunocompromised. Dosage and timing are critical: a half-dose booster of the Moderna vaccine has shown efficacy in maintaining immunity without excessive side effects. This highlights the need for tailored booster strategies based on individual risk factors and pathogen behavior.
A comparative analysis of subunit vaccines reveals that their booster needs are influenced by both the antigen’s stability and the immune system’s memory response. For instance, the human papillomavirus (HPV) vaccine, a subunit vaccine, provides protection for at least 10 years, with ongoing studies assessing the need for boosters. In contrast, the seasonal influenza subunit vaccine requires annual boosters due to rapid viral mutation. This underscores the importance of monitoring both the pathogen’s evolution and the host’s immune durability. Practical tips for individuals include staying informed about updated booster recommendations and maintaining vaccination records to track eligibility.
From a persuasive standpoint, periodic boosters for subunit vaccines are not merely a precautionary measure but a strategic tool to sustain herd immunity. Without timely boosters, pockets of susceptibility can emerge, allowing pathogens to circulate and mutate. For example, the resurgence of pertussis in some regions has been linked to waning immunity from acellular vaccines, emphasizing the role of boosters in preventing outbreaks. Policymakers must balance the logistical challenges of booster campaigns with the public health benefits, ensuring equitable access to doses. Individuals, too, play a role by adhering to booster schedules and advocating for vaccine education.
In conclusion, the need for periodic boosters with subunit vaccines hinges on a complex interplay of immunological, epidemiological, and practical factors. While some subunit vaccines offer prolonged protection, others require regular reinforcement to maintain efficacy. Tailored booster strategies, informed by data and individual risk, are essential to maximize the benefits of these vaccines. As new subunit vaccines emerge, ongoing research and surveillance will remain critical to defining optimal booster requirements, ensuring sustained immunity in an ever-changing landscape of infectious diseases.
Is Shingrix Vaccine Covered by Medicare Part D? Find Out
You may want to see also
Explore related products





![]()
Antigen Stability: Role of stable antigens in subunit vaccines for sustained immune response
Subunit vaccines, which contain specific fragments of a pathogen rather than the entire organism, hinge on the stability of their antigenic components to elicit a sustained immune response. Unlike live-attenuated or inactivated vaccines, subunit vaccines rely on precise molecular structures to trigger immunity, making antigen stability a critical factor in their efficacy and longevity. A stable antigen maintains its structural integrity over time, ensuring consistent presentation to the immune system and reducing the likelihood of degradation that could compromise vaccine potency. For instance, the hepatitis B vaccine, a well-known subunit vaccine, uses recombinant hepatitis B surface antigen (HBsAg) that remains stable under proper storage conditions, enabling long-term protection with a series of doses typically administered at 0, 1, and 6 months.
The role of stable antigens becomes particularly evident when considering the challenges of vaccine formulation and delivery. Adjuvants, which enhance immune responses, are often paired with subunit vaccines to compensate for their inherently weaker immunogenicity compared to whole-pathogen vaccines. However, the effectiveness of adjuvants depends on the antigen’s stability. For example, the AS04 adjuvant system used in the HPV vaccine Cervarix requires a stable HPV L1 protein antigen to form virus-like particles (VLPs) that mimic the virus’s structure without its genetic material. This stability ensures the VLPs remain intact, allowing for robust and sustained immune recognition. Without stable antigens, adjuvants alone cannot guarantee long-term protection, underscoring the antigen’s central role in vaccine durability.
Practical considerations for maintaining antigen stability include storage conditions, formulation techniques, and dosage regimens. Subunit vaccines often require refrigeration (2–8°C) to prevent antigen degradation, a factor that can limit their accessibility in resource-constrained settings. Innovations like lyophilization (freeze-drying) and the use of thermostable formulations are addressing these challenges, enabling vaccines to withstand higher temperatures without losing potency. For instance, a lyophilized version of the meningococcal serogroup A conjugate vaccine (MenAfriVac) has demonstrated stability at up to 40°C for four days, expanding its reach in regions with unreliable refrigeration. Such advancements highlight the interplay between antigen stability and vaccine accessibility, particularly in global health contexts.
From a clinical perspective, the stability of antigens directly influences dosing schedules and booster requirements. While subunit vaccines rarely provide lifelong immunity with a single dose, stable antigens enable predictable immune memory and effective boosting. The tetanus toxoid vaccine, for example, relies on a stable antigen that induces long-term immunity with periodic boosters every 10 years for adults. In contrast, vaccines with less stable antigens may require more frequent doses or higher concentrations to achieve comparable protection. Understanding antigen stability thus informs not only vaccine design but also public health strategies for immunization campaigns, ensuring that resources are allocated efficiently to maximize population-level immunity.
In conclusion, antigen stability is the linchpin of subunit vaccines’ ability to provide sustained immune responses. By preserving the structural integrity of antigenic components, these vaccines can reliably elicit immunity, even if boosters are needed to maintain protection. Advances in formulation and storage techniques are expanding the reach of subunit vaccines, particularly in challenging environments. As research continues to refine antigen stability, subunit vaccines hold promise as a versatile and effective tool in the fight against infectious diseases, bridging the gap between short-term immunity and long-term protection.
Fully Vaccinated and Close Contact: What You Need to Know
You may want to see also
Explore related products






![]()
Individual Variability: How age, health, and genetics affect lifelong protection from subunit vaccines
Subunit vaccines, designed to deliver specific antigens without live pathogens, are celebrated for their safety and targeted immune response. However, their ability to provide lifelong protection is not uniform across individuals. Age, health status, and genetic factors play pivotal roles in determining how long immunity lasts, creating a spectrum of outcomes that defy one-size-fits-all expectations.
Consider age as a primary determinant. In children, whose immune systems are still maturing, subunit vaccines often require multiple doses to establish robust immunity. For instance, the hepatitis B vaccine is administered in three doses over six months to ensure adequate protection. In contrast, older adults, particularly those over 65, may experience diminished immune responses due to immunosenescence—the gradual decline of immune function with age. This is why booster shots for vaccines like shingles (Shingrix) are recommended for this demographic. The same vaccine that confers decades of protection in a 30-year-old might wane significantly in a 70-year-old within five years.
Health status further complicates this variability. Individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, often mount weaker responses to subunit vaccines. For example, a study on the HPV vaccine found that immunocompromised individuals required higher antigen doses or additional boosters to achieve comparable antibody levels to healthy counterparts. Conversely, individuals with autoimmune disorders may exhibit heightened or unpredictable responses, necessitating personalized vaccination strategies. Practical advice for this group includes consulting specialists to tailor vaccine schedules and potentially incorporating serological testing to monitor immunity.
Genetics introduces another layer of complexity. Variations in genes like HLA (human leukocyte antigen) influence how effectively the body processes and responds to vaccine antigens. For instance, certain HLA types are associated with stronger immune responses to the influenza vaccine, while others may predispose individuals to rapid antibody decay. Emerging research in pharmacogenomics aims to identify genetic markers that predict vaccine efficacy, potentially enabling personalized dosing or alternative vaccine formulations. Until such advancements become mainstream, healthcare providers must rely on clinical history and risk factors to optimize protection.
In summary, while subunit vaccines are a cornerstone of modern immunization, their lifelong protective capacity is far from universal. Age-related immune changes, underlying health conditions, and genetic predispositions collectively shape individual outcomes. Tailoring vaccination strategies—whether through adjusted dosing, booster schedules, or monitoring—is essential to bridge the gap between theoretical efficacy and real-world protection. Understanding these variables empowers both providers and recipients to make informed decisions, ensuring the greatest possible benefit from these vital tools.
Hepatitis B Vaccines: Essential Immunizations for Prevention and Protection
You may want to see also
Explore related products






![]()
Emerging Variants: Impact of pathogen mutations on the longevity of subunit vaccine protection
Pathogen mutations are a relentless challenge to the longevity of subunit vaccine protection. Unlike live-attenuated or mRNA vaccines, subunit vaccines rely on specific antigenic components, making them particularly vulnerable to changes in the pathogen's structure. Emerging variants, such as those seen in SARS-CoV-2, can alter key epitopes targeted by the vaccine, reducing antibody recognition and neutralization efficacy. For instance, the Omicron variant's extensive spike protein mutations significantly diminished the protective efficacy of early COVID-19 subunit vaccines, necessitating booster doses to restore immunity.
To mitigate the impact of variants, vaccine developers are exploring strategies like multivalent formulations, which include antigens from multiple strains. For example, the AS03-adjuvanted COVID-19 subunit vaccine candidate by Sanofi and GSK is being tested in a bivalent format to broaden immune responses. Additionally, incorporating conserved viral regions, less prone to mutation, could enhance long-term protection. However, this approach requires precise identification of such regions, a task complicated by the pathogen's evolutionary dynamics.
Practical considerations for individuals include adhering to recommended booster schedules, especially for those over 65 or immunocompromised, as waning immunity and variant emergence increase susceptibility. Monitoring antibody levels through serological testing can also guide personalized vaccination strategies. For travelers or those in high-risk areas, staying informed about local variant prevalence and vaccine updates is crucial.
A comparative analysis of subunit vaccines across pathogens reveals a recurring theme: while they offer safety and stability, their protection is inherently tied to antigenic stability. For instance, the hepatitis B subunit vaccine provides long-lasting immunity due to the virus's slow mutation rate, whereas influenza subunit vaccines require annual updates to match circulating strains. This underscores the need for adaptive vaccine platforms capable of rapid reconfiguration in response to emerging variants.
In conclusion, the longevity of subunit vaccine protection is fundamentally threatened by pathogen mutations, necessitating proactive strategies in vaccine design, administration, and public health policy. By embracing multivalent formulations, targeting conserved antigens, and fostering global surveillance, we can enhance the resilience of subunit vaccines against the ever-evolving landscape of infectious diseases.
Medicare Part B: TDAP Vaccine Coverage Explained
You may want to see also
Frequently asked questions
Not necessarily. While subunit vaccines can offer long-lasting immunity, they may not always provide lifetime protection. Booster doses may be required to maintain immunity, depending on the vaccine and the disease.
Subunit vaccines use specific parts of a pathogen, which may not stimulate the same level of immune memory as a whole pathogen. Additionally, factors like individual immune response and pathogen evolution can affect the duration of protection.
Some subunit vaccines, like the hepatitis B vaccine, can provide long-term or even lifelong immunity for many individuals. However, this varies by vaccine and person, and monitoring or boosters may still be recommended.
Consult your healthcare provider or follow public health guidelines. Booster recommendations are based on factors like waning immunity, disease prevalence, and individual risk. Regular check-ups and antibody testing may also help determine the need for a booster.