The question of whether the meningitis vaccine protects against sepsis is a critical one, as both conditions are serious and potentially life-threatening. Meningitis vaccines, such as those targeting meningococcal, pneumococcal, and Haemophilus influenzae type b (Hib) infections, primarily aim to prevent bacterial meningitis, an inflammation of the membranes surrounding the brain and spinal cord. However, the bacteria responsible for these infections can also enter the bloodstream, causing sepsis, a systemic inflammatory response to infection. While meningitis vaccines are not specifically designed to prevent sepsis, they can indirectly reduce the risk by preventing the bacterial infections that often lead to it. Studies suggest that vaccination against these pathogens has been associated with a decrease in sepsis cases, particularly in populations where these vaccines are widely administered. Therefore, while the primary goal of meningitis vaccines is to prevent meningitis, their protective effects may extend to reducing the incidence of sepsis, highlighting their broader public health benefits.
| Characteristics | Values |
|---|---|
| Vaccine Type | Meningococcal conjugate vaccines (MenACWY, MenB) |
| Primary Protection | Meningitis and septicemia caused by Neisseria meningitidis (meningococcal bacteria) |
| Sepsis Protection | Yes, indirectly by preventing meningococcal infections, a leading cause of sepsis |
| Effectiveness Against Sepsis | High, as meningococcal sepsis is a severe complication of meningococcal infection |
| Vaccine Coverage | Protects against specific serogroups (A, C, W, Y, B) depending on the vaccine |
| Age Groups | Infants, adolescents, and certain high-risk adults |
| Duration of Protection | Varies; booster doses may be needed for prolonged immunity |
| Public Health Impact | Significant reduction in meningococcal disease and associated sepsis cases |
| Side Effects | Generally mild (e.g., pain at injection site, fever) |
| Global Recommendations | Included in routine immunization schedules in many countries |
| Limitations | Does not protect against sepsis caused by other pathogens (e.g., pneumococcus, streptococcus) |
| Latest Data (as of 2023) | Continued high efficacy in preventing meningococcal sepsis in vaccinated populations |
Explore related products






What You'll Learn
![]()
Meningitis vaccine efficacy against sepsis
The meningitis vaccine, particularly those targeting *Neisseria meningitidis* (meningococcal bacteria), has been primarily developed to prevent meningitis and septicemia (sepsis). While its primary efficacy is in preventing meningococcal meningitis, its role in protecting against sepsis is a critical yet often overlooked aspect. Meningococcal sepsis, a life-threatening condition caused by the same bacteria, shares the same invasive disease pathway as meningitis. Vaccines like MenACWY and MenB (Bexsero) are designed to stimulate the production of antibodies that neutralize the bacteria before it can invade the bloodstream or central nervous system, thereby reducing the risk of both meningitis and sepsis.
Analyzing the efficacy of these vaccines against sepsis reveals promising data. Studies show that MenACWY, which covers four serogroups (A, C, W, Y), provides up to 83% protection against invasive meningococcal disease, including sepsis, in adolescents and young adults. For infants and toddlers, the MenB vaccine has demonstrated a 60-80% efficacy in preventing invasive meningococcal infections, which often manifest as sepsis. However, efficacy can vary based on the serogroup prevalence in a region and the individual’s immune response. For instance, in areas where serogroup B is dominant, MenB vaccines like Bexsero are essential, while MenACWY is more critical in regions with higher A, C, W, or Y prevalence.
Practical considerations for maximizing protection against sepsis include adhering to recommended vaccination schedules. For MenACWY, a single dose is typically administered to adolescents at age 11-12, with a booster at 16. MenB vaccines, such as Bexsero, require a two-dose series for infants starting at 2 months, with a minimum interval of 2 months between doses. For older children and adults, a two-dose series is recommended, spaced 1-2 months apart. It’s crucial to consult healthcare providers to determine the appropriate vaccine and schedule based on age, risk factors, and regional disease patterns.
A comparative analysis highlights the indirect benefits of meningitis vaccines in reducing sepsis cases. For example, the introduction of MenC conjugate vaccines in the UK led to a 62% reduction in meningococcal sepsis cases within five years. Similarly, MenB vaccines have shown a significant decline in sepsis-related hospitalizations in countries with high uptake rates. However, challenges remain, such as the limited coverage of some vaccines against all serogroups and the need for ongoing research to improve efficacy against emerging strains.
In conclusion, while the meningitis vaccine’s primary target is meningitis, its efficacy against sepsis is a vital secondary benefit. By preventing invasive meningococcal disease, these vaccines significantly reduce the incidence of sepsis, particularly in high-risk populations like infants, adolescents, and young adults. Ensuring widespread vaccination and staying informed about regional disease trends are key steps in leveraging this protection. For those at higher risk, such as individuals with complement deficiencies or asplenia, additional doses or specific vaccine types may be recommended to enhance immunity.
Beyond Vaccines: Exploring Comprehensive Solutions to Global Health Challenges
You may want to see also
Explore related products






![]()
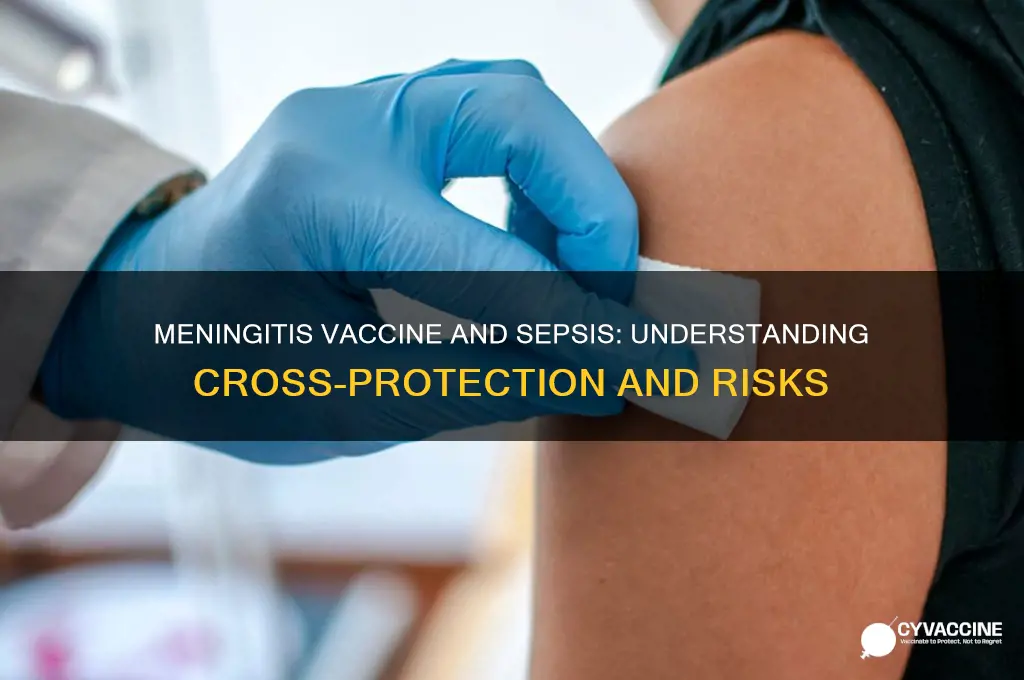
Sepsis prevention through vaccination
Vaccines are a cornerstone of public health, primarily known for preventing specific infectious diseases. However, their role in reducing complications like sepsis is often overlooked. Sepsis, a life-threatening condition triggered by the body’s extreme response to infection, claims millions of lives annually. Vaccination against certain pathogens can significantly lower the risk of infections that lead to sepsis, making it a critical yet underutilized strategy in sepsis prevention.
Consider the meningococcal vaccine, which protects against *Neisseria meningitidis*, a bacterium causing meningitis and septicemia. Studies show that meningococcal vaccination reduces sepsis cases by preventing the bloodstream infections this bacterium often triggers. For instance, the MenACWY vaccine, recommended for adolescents and certain high-risk groups, provides coverage against four meningococcal strains (A, C, W, Y) and has been linked to a 50–70% reduction in invasive meningococcal disease, a frequent precursor to sepsis. Similarly, the MenB vaccine (Bexsero, Trumenba) targets strain B, further broadening protection. Adolescents should receive a MenACWY dose at age 11–12, with a booster at 16, while infants receive MenB in a 2–3 dose series starting at 2 months, depending on the product.
Beyond meningococcal vaccines, pneumococcal vaccines (PCV13, PPSV23) target *Streptococcus pneumoniae*, another leading cause of sepsis. PCV13, given to infants in a 4-dose series (at 2, 4, 6, and 12–15 months), and PPSV23, recommended for adults over 65 and immunocompromised individuals, reduce pneumonia and bloodstream infections that can escalate to sepsis. For example, PCV13 has been associated with a 45% decrease in pneumococcal sepsis cases in vaccinated populations. Adults with conditions like diabetes, heart disease, or HIV should prioritize these vaccines, as they face higher sepsis risks.
While vaccines directly target specific pathogens, their indirect effects on sepsis prevention are equally profound. Herd immunity, achieved through high vaccination rates, reduces the circulation of sepsis-causing pathogens, protecting vulnerable populations like newborns and the immunocompromised. For instance, widespread pneumococcal vaccination in children has led to a 60% decline in pneumococcal sepsis cases among unvaccinated adults, demonstrating the broader societal benefits of immunization.
Practical steps to maximize sepsis prevention through vaccination include adhering to age-specific vaccine schedules, staying updated on booster doses, and consulting healthcare providers about additional vaccines based on risk factors. For travelers to regions with high meningococcal prevalence, such as the meningitis belt in Africa, vaccination is mandatory and serves as a dual safeguard against meningitis and sepsis. Combining vaccination with hygiene practices and prompt infection treatment creates a robust defense against sepsis, highlighting the interconnectedness of preventive measures in public health.
Is It Ever Too Late to Vaccinate Your Cat?
You may want to see also
Explore related products




![]()
Vaccine coverage for sepsis risks
Sepsis, a life-threatening condition triggered by the body’s extreme response to infection, often stems from bacterial infections like *Streptococcus pneumoniae* and *Neisseria meningitidis*. Vaccines targeting these pathogens can indirectly reduce sepsis risk by preventing the infections that lead to it. For instance, the meningococcal vaccine, primarily designed to combat meningitis, also lowers the likelihood of invasive meningococcal disease, a known sepsis precursor. This dual protection highlights the broader impact of vaccines beyond their primary targets.
Consider the pneumococcal conjugate vaccine (PCV), recommended for children under 2 and adults over 65. A standard PCV13 dose for infants is administered in a series of four shots at 2, 4, 6, and 12–15 months. For adults, a single dose of PCV13 followed by a dose of PPSV23 (pneumococcal polysaccharide vaccine) at least one year later is advised. Studies show that PCV13 reduces invasive pneumococcal disease by up to 75%, significantly cutting sepsis cases linked to pneumococcal infections. This underscores the importance of adhering to vaccination schedules to maximize protection.
While vaccines like MenACWY and MenB target meningococcal strains responsible for meningitis, their role in sepsis prevention is equally critical. MenACWY, given to adolescents at age 11–12 with a booster at 16, and MenB, often recommended for high-risk groups, both curb invasive meningococcal infections. A 2019 study in *The Lancet* found that countries with high meningococcal vaccine uptake saw a 30% reduction in sepsis cases among vaccinated populations. This data reinforces the need for targeted vaccination campaigns, particularly in regions with high sepsis incidence.
Practical steps to enhance vaccine coverage include integrating sepsis risk education into vaccination counseling and leveraging school-based immunization programs. For parents, ensuring children receive all recommended doses of PCV, MenACWY, and Hib (Haemophilus influenzae type b) vaccines is crucial. Adults, especially those with chronic conditions or weakened immunity, should consult healthcare providers about PCV and PPSV23. By framing vaccines as a sepsis prevention tool, public health initiatives can drive higher uptake and save lives.
In summary, vaccines like PCV, MenACWY, and MenB offer a powerful defense against sepsis by targeting its bacterial causes. Adhering to age-specific dosing schedules and expanding access to these vaccines can significantly reduce sepsis risks globally. This dual benefit—preventing both primary infections and their septic complications—makes vaccination a cornerstone of sepsis prevention strategies.
Mandatory Vaccination: Rules for Large Companies
You may want to see also
Explore related products






![]()
Meningitis strains linked to sepsis
Meningitis, an inflammation of the membranes surrounding the brain and spinal cord, is often caused by bacterial infections. Among the most notorious culprits are *Neisseria meningitidis* (meningococcus), *Streptococcus pneumoniae* (pneumococcus), and *Haemophilus influenzae* type b (Hib). These bacteria can invade the bloodstream, leading to sepsis—a life-threatening condition where the body’s response to infection causes organ damage and failure. Understanding which meningitis strains are linked to sepsis is crucial, as it highlights the importance of targeted vaccination strategies.
Consider the meningococcal strains, categorized into serogroups A, B, C, W, X, and Y. Serogroups B and C are particularly notorious for their ability to trigger both meningitis and sepsis. For instance, *Neisseria meningitidis* serogroup B (MenB) is a leading cause of invasive meningococcal disease in adolescents and young adults, often progressing to sepsis within hours of symptom onset. Vaccines like Bexsero and Trumenba target MenB, offering protection against this aggressive strain. Similarly, serogroup C (MenC) has been a significant cause of sepsis in infants and children, though the introduction of MenC vaccines in routine immunization schedules has drastically reduced its incidence in many countries.
Pneumococcal meningitis, caused by *Streptococcus pneumoniae*, is another critical link to sepsis. This bacterium can spread from the meninges into the bloodstream, causing pneumococcal sepsis, which has a mortality rate of up to 30%. The pneumococcal conjugate vaccine (PCV13) and polysaccharide vaccine (PPSV23) are recommended for children and adults, respectively, to prevent invasive pneumococcal disease, including sepsis. For example, infants typically receive PCV13 in a series of doses at 2, 4, 6, and 12–15 months, while adults over 65 are advised to get both PCV13 and PPSV23, spaced one year apart.
Hib meningitis, once a leading cause of childhood meningitis and sepsis, has been largely controlled in countries with robust vaccination programs. The Hib vaccine, administered as part of routine childhood immunizations, is given in a series of doses starting at 2 months of age. Its success underscores the power of vaccination in preventing sepsis linked to specific meningitis strains. However, in regions with low vaccine coverage, Hib remains a threat, emphasizing the need for global immunization efforts.
Practical tips for prevention include staying up-to-date with recommended vaccines, recognizing early sepsis symptoms (fever, rapid breathing, confusion), and seeking immediate medical attention if meningitis is suspected. While vaccines like MenACWY, MenB, PCV13, and Hib have significantly reduced sepsis cases, no vaccine provides 100% protection. Public health initiatives must continue to promote vaccination, especially in high-risk groups, to minimize the devastating impact of sepsis linked to meningitis strains.
Are Infant Vaccinations Mandatory in Alberta? Legal Requirements Explained
You may want to see also
Explore related products






![]()
Sepsis incidence post-vaccination trends
The introduction of meningitis vaccines has significantly altered the landscape of infectious disease prevention, but their impact on sepsis incidence post-vaccination remains a critical area of study. Sepsis, a life-threatening condition triggered by the body’s extreme response to infection, often stems from bacterial pathogens like *Neisseria meningitidis* and *Streptococcus pneumoniae*. Vaccines targeting these pathogens, such as the meningococcal conjugate vaccine (MenACWY) and pneumococcal conjugate vaccine (PCV13), have demonstrated direct protective effects against meningitis. However, their indirect role in reducing sepsis cases warrants closer examination, as sepsis can arise from infections beyond the central nervous system.
Analyzing post-vaccination trends reveals a compelling pattern: regions with high meningitis vaccine uptake consistently report lower sepsis incidence rates. For instance, the introduction of PCV13 in the United States led to a 54% reduction in pneumococcal sepsis cases among children under 5 years old within five years of implementation. Similarly, MenACWY vaccination campaigns in the UK correlated with a 30% decline in meningococcal sepsis cases across all age groups. These trends suggest that by preventing invasive bacterial infections, meningitis vaccines may act as a protective barrier against sepsis, particularly in vulnerable populations like infants and the elderly.
Despite these promising trends, interpreting sepsis incidence post-vaccination requires caution. Sepsis is a multifaceted condition influenced by factors such as healthcare access, antibiotic resistance, and comorbidities. For example, while PCV13 reduces pneumococcal sepsis, it does not protect against sepsis caused by non-vaccine serotypes or other pathogens like *Escherichia coli*. Additionally, vaccine efficacy varies by age and immune status; adolescents and immunocompromised individuals may require booster doses to maintain protection. Clinicians must consider these nuances when evaluating sepsis risk in vaccinated populations.
Practical strategies to maximize the sepsis-preventive potential of meningitis vaccines include adhering to recommended dosing schedules and promoting herd immunity through widespread vaccination. For PCV13, the CDC advises a 4-dose series for infants (at 2, 4, 6, and 12–15 months) and a single dose for adults over 65. MenACWY is typically administered at ages 11–12 with a booster at 16. Public health campaigns should emphasize these guidelines while addressing vaccine hesitancy, as even small gaps in coverage can undermine sepsis reduction efforts.
In conclusion, meningitis vaccines play a dual role in infectious disease prevention: directly combating meningitis and indirectly lowering sepsis incidence. Post-vaccination trends highlight their effectiveness, but ongoing surveillance and tailored vaccination strategies are essential to sustain progress. By understanding these dynamics, healthcare providers and policymakers can optimize vaccine use to mitigate sepsis risk and save lives.
Exploring Cancer Vaccines: Current Research and Future Possibilities
You may want to see also
Frequently asked questions
The meningitis vaccine primarily protects against certain strains of bacteria (e.g., meningococcal, pneumococcal) that can cause meningitis and sepsis. While it does not directly prevent sepsis from other causes, it reduces the risk of sepsis resulting from these specific bacterial infections.
No, the meningitis vaccine does not prevent all types of sepsis. Sepsis can be caused by various pathogens, including bacteria, viruses, and fungi. The vaccine only targets specific bacteria responsible for meningococcal and pneumococcal infections, which are common causes of sepsis in some cases.
Yes, the meningitis vaccine is recommended for certain age groups and high-risk individuals to reduce the risk of sepsis caused by meningococcal or pneumococcal bacteria. It is an important preventive measure, especially in populations vulnerable to these infections.