The AstraZeneca COVID-19 vaccine, also known as ChAdOx1 nCoV-19 or Vaxzevria, is a viral vector-based vaccine designed to protect against COVID-19. Unlike mRNA vaccines, which directly deliver genetic material encoding the SARS-CoV-2 spike protein, the AstraZeneca vaccine uses a modified chimpanzee adenovirus (ChAdOx1) to deliver the gene for the spike protein into cells. Once inside the cells, this gene instructs them to produce the spike protein, which then triggers an immune response, preparing the body to fight off the actual virus. Therefore, while the AstraZeneca vaccine does not contain the spike protein itself, it enables the body to produce it as part of its mechanism to build immunity against COVID-19.
| Characteristics | Values |
|---|---|
| Vaccine Type | Viral vector-based (uses a modified chimpanzee adenovirus, ChAdOx1) |
| Target Antigen | SARS-CoV-2 Spike Protein (S protein) |
| Mechanism | Delivers genetic material encoding the spike protein to cells |
| Spike Protein Role | Induces immune response to neutralize the virus |
| Does it contain the spike protein? | No, it contains the genetic instructions to produce the spike protein |
| Spike Protein Production | Produced by human cells after vaccination |
| Immune Response | Triggers antibody and T-cell responses against the spike protein |
| Efficacy Against COVID-19 | ~60-90% depending on dosing regimen and variant |
| Storage Requirements | Refrigerated (2°C to 8°C or 36°F to 46°F) |
| Dosing Schedule | Two doses, typically 4-12 weeks apart |
| Approval Status | Approved or authorized in many countries, including the EU, UK, and WHO |
| Side Effects | Common: Injection site pain, fatigue, headache, fever, muscle pain |
| Rare Side Effects | Thrombosis with thrombocytopenia syndrome (TTS), very rare |
| Variant Coverage | Effective against original strain, reduced efficacy against some variants like Omicron |
| Pregnancy and Breastfeeding | Considered safe, but consult healthcare provider |
| Age Group | Approved for adults (18+), some countries approve for adolescents |
| Manufacturer | AstraZeneca in collaboration with the University of Oxford |
Explore related products






What You'll Learn
- Vaccine Composition: AstraZeneca uses a modified adenovirus to deliver the SARS-CoV-2 spike protein gene
- Spike Protein Role: The spike protein triggers immune response, preparing the body to fight COVID-19
- Safety Concerns: Rare side effects like blood clots linked to spike protein production
- Efficacy Studies: Clinical trials confirm AstraZeneca’s spike protein approach is effective against COVID-19
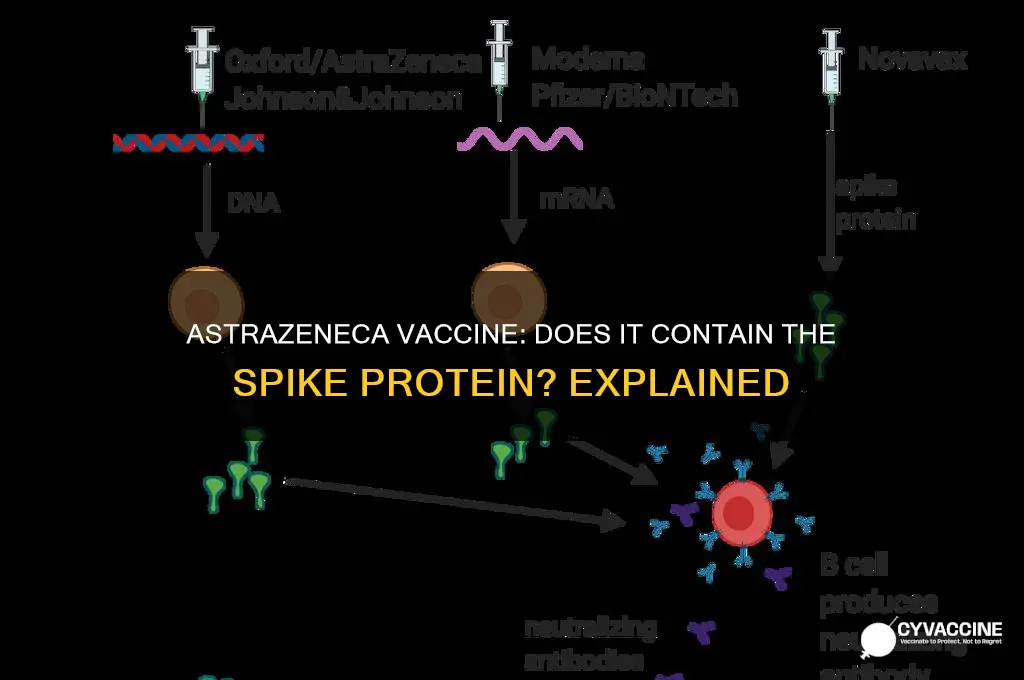
- Comparison to mRNA: AstraZeneca’s viral vector method differs from mRNA vaccines’ direct spike protein coding
![]()
Vaccine Composition: AstraZeneca uses a modified adenovirus to deliver the SARS-CoV-2 spike protein gene
The AstraZeneca COVID-19 vaccine, known as Vaxzevria or AZD1222, employs a unique delivery system to introduce the SARS-CoV-2 spike protein gene into the body. Unlike mRNA vaccines, which use genetic material to instruct cells to produce the spike protein, AstraZeneca’s vaccine utilizes a modified adenovirus—specifically, a chimpanzee adenovirus (ChAdOx1)—as a vector. This adenovirus is engineered to be non-replicating, meaning it cannot cause disease in humans, but it effectively transports the spike protein gene into cells. Once inside, the gene prompts the production of the spike protein, triggering an immune response without exposing the recipient to the actual virus.
This method of delivery is both innovative and practical. Adenoviruses are well-studied and have been used in gene therapy for decades, making them a reliable choice for vaccine development. The ChAdOx1 vector is particularly advantageous because it has a low prevalence in human populations, reducing the likelihood of pre-existing immunity that could hinder its effectiveness. For individuals aged 18 and older, a standard regimen involves two doses, typically administered 4 to 12 weeks apart, depending on local health guidelines. This dosing interval allows the immune system to mount a robust response while minimizing the risk of side effects.
One of the key benefits of AstraZeneca’s approach is its stability and ease of storage. Unlike mRNA vaccines, which require ultra-cold temperatures, Vaxzevria can be stored at standard refrigerator temperatures (2°C to 8°C). This makes it a more accessible option for low- and middle-income countries with limited cold chain infrastructure. However, it’s important to note that the vaccine should not be frozen, as this can compromise its efficacy. Healthcare providers should adhere to storage guidelines to ensure the vaccine remains potent and safe for administration.
While the vaccine’s composition is highly effective in eliciting an immune response, it has been associated with rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS). These cases are extremely uncommon, occurring in approximately 1 in 50,000 to 1 in 100,000 recipients, primarily in younger age groups. As a result, some countries have recommended alternative vaccines for individuals under 30 or 40, depending on local risk assessments. Patients should be informed of these risks and monitored for symptoms such as severe headaches, abdominal pain, or unusual bruising after vaccination.
In summary, AstraZeneca’s vaccine composition leverages a modified adenovirus to deliver the SARS-CoV-2 spike protein gene, offering a practical and effective immunization strategy. Its storage advantages and established dosing regimen make it a valuable tool in global vaccination efforts, particularly in regions with limited resources. However, awareness of rare side effects is crucial for informed decision-making and patient safety. By understanding its unique mechanism and practical considerations, healthcare providers and recipients can maximize the benefits of this vaccine while minimizing risks.
The Golden Age of Vaccines: A 20th Century Revolution
You may want to see also
Explore related products






![]()
Spike Protein Role: The spike protein triggers immune response, preparing the body to fight COVID-19
The AstraZeneca COVID-19 vaccine, like several other vaccines, utilizes a key component of the SARS-CoV-2 virus to elicit an immune response: the spike protein. This protein is crucial to the virus's ability to infect cells, as it binds to the ACE2 receptor on human cells, facilitating viral entry. By incorporating a modified, non-infectious version of the spike protein, the AstraZeneca vaccine teaches the immune system to recognize and combat the virus without exposing the individual to the risks of COVID-19. This approach is both innovative and effective, leveraging the body’s natural defenses to build immunity.
To understand the spike protein’s role, consider it as a blueprint for immune preparedness. When the AstraZeneca vaccine is administered, typically in two doses given 4 to 12 weeks apart, it delivers genetic material (in the form of a chimpanzee adenovirus vector) encoding the spike protein. The immune system identifies this protein as foreign, prompting the production of antibodies and activation of T-cells. This dual response not only neutralizes the virus but also creates a memory of it, enabling a faster and more robust reaction if the individual encounters the actual virus later. For adults aged 18 and older, this mechanism has proven highly effective in preventing severe illness, hospitalization, and death from COVID-19.
One practical tip for maximizing the vaccine’s efficacy is to ensure timely administration of both doses. While a single dose provides partial protection, the second dose significantly enhances immunity, particularly against emerging variants. Additionally, individuals should monitor for mild side effects, such as fatigue, headache, or injection site pain, which are normal signs of the immune system responding to the vaccine. These symptoms typically resolve within a few days and can be managed with rest and over-the-counter pain relievers like acetaminophen.
Comparatively, the AstraZeneca vaccine’s use of the spike protein differs from mRNA vaccines like Pfizer and Moderna, which deliver genetic instructions directly to cells to produce the spike protein. Despite these differences, all these vaccines share the common goal of triggering a targeted immune response. The AstraZeneca vaccine’s adenovirus vector approach offers advantages such as easier storage and distribution, making it a valuable tool in global vaccination efforts, especially in regions with limited access to ultra-cold storage facilities.
In conclusion, the spike protein’s role in the AstraZeneca vaccine is pivotal, serving as the catalyst for a robust immune response that prepares the body to fight COVID-19. By understanding its function and following practical guidelines for vaccination, individuals can maximize the benefits of this life-saving intervention. Whether through adenovirus vectors or mRNA technology, the focus on the spike protein underscores its centrality in the battle against the pandemic.
NJ Vaccine Eligibility: Who Qualifies and How to Register
You may want to see also
Explore related products






![]()
Safety Concerns: Rare side effects like blood clots linked to spike protein production
The AstraZeneca COVID-19 vaccine, like other adenovirus vector-based vaccines, delivers genetic material encoding the SARS-CoV-2 spike protein into cells, prompting the immune system to recognize and combat the virus. While this mechanism has proven effective in preventing severe illness, rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), have raised safety concerns. TTS involves unusual blood clots combined with low platelet counts, typically occurring 4 to 28 days after vaccination, predominantly in individuals under 60 years old. Understanding this risk is crucial for informed decision-making, especially for those weighing vaccination benefits against potential adverse reactions.
Analyzing the data, the incidence of TTS is extremely low, estimated at approximately 1 in 50,000 to 1 in 100,000 doses administered. Symptoms may include severe headache, blurred vision, chest pain, or persistent abdominal pain, requiring immediate medical attention. While the exact mechanism linking spike protein production to TTS remains under investigation, it is hypothesized that the immune response may trigger antibodies targeting platelet factor 4, leading to clot formation. This rare event underscores the importance of monitoring post-vaccination symptoms and seeking prompt care if unusual signs appear.
From a practical standpoint, healthcare providers should educate patients about TTS symptoms and emphasize the importance of timely reporting. For individuals at higher risk, alternative vaccines, such as mRNA-based options, may be recommended. In regions with limited vaccine availability, however, the benefits of AstraZeneca’s vaccine in preventing severe COVID-19 outcomes often outweigh the minimal TTS risk. Public health campaigns should balance transparency about risks with clear communication of the vaccine’s efficacy, ensuring trust and informed consent.
Comparatively, the risk of blood clots from COVID-19 infection itself is significantly higher than that associated with the AstraZeneca vaccine. Studies show that COVID-19 patients are 100 times more likely to develop blood clots than those vaccinated with AstraZeneca. This comparison highlights the vaccine’s role in reducing overall clotting risks, particularly in populations with high viral transmission rates. By framing TTS within this broader context, individuals can make decisions grounded in both relative and absolute risk assessments.
In conclusion, while rare side effects like TTS linked to spike protein production are a valid concern, they represent a small fraction of vaccine recipients. Vigilance in symptom monitoring, coupled with evidence-based risk communication, can mitigate fears and maximize vaccination benefits. As research continues, ongoing surveillance and transparent reporting will remain essential in maintaining public confidence in vaccine safety.
Essential Horse Vaccination Schedule: Protecting Equine Health Year-Round
You may want to see also
Explore related products




![]()
Efficacy Studies: Clinical trials confirm AstraZeneca’s spike protein approach is effective against COVID-19
The AstraZeneca COVID-19 vaccine, known as AZD1222 or ChAdOx1 nCoV-19, leverages a unique approach by using a modified adenovirus to deliver the genetic code for the SARS-CoV-2 spike protein into cells. This design prompts the immune system to recognize and combat the virus effectively. Clinical trials have rigorously evaluated its efficacy, providing robust evidence of its ability to prevent COVID-19, particularly severe cases and hospitalizations. These studies, involving tens of thousands of participants across diverse populations, have confirmed that AstraZeneca’s spike protein-based strategy is both safe and effective.
One of the key findings from these trials is the vaccine’s efficacy rate, which varies slightly depending on dosing intervals. When administered with a 12-week gap between doses, the vaccine demonstrated an efficacy of up to 81% in preventing symptomatic COVID-19. This extended interval not only enhances immune response but also aligns with practical considerations for global vaccination campaigns. For individuals aged 18 and older, the standard regimen involves two doses of 0.5 mL each, administered intramuscularly. Adhering to this schedule maximizes the vaccine’s protective effects, as evidenced by reduced infection rates and milder symptoms in breakthrough cases.
Comparative analyses of AstraZeneca’s vaccine against other COVID-19 vaccines highlight its unique advantages. Unlike mRNA vaccines, which require ultra-cold storage, AstraZeneca’s vaccine can be stored at standard refrigerator temperatures (2°C to 8°C), making it more accessible in low-resource settings. Additionally, its efficacy against severe disease and hospitalization remains consistently high across age groups, including older adults who are often at higher risk. This makes it a valuable tool in global vaccination efforts, particularly in regions with limited infrastructure.
Practical considerations for recipients include monitoring for common side effects, such as fatigue, headache, and injection site pain, which typically resolve within a few days. It’s essential to follow healthcare provider instructions regarding dosing intervals and to report any severe or persistent symptoms promptly. For those with specific medical conditions or concerns, consulting a healthcare professional ensures personalized guidance. The vaccine’s proven efficacy, combined with its logistical advantages, underscores its role as a critical component in the fight against COVID-19.
In conclusion, clinical trials have unequivocally confirmed that AstraZeneca’s spike protein approach is effective in preventing COVID-19, particularly severe outcomes. Its flexible dosing schedule, high efficacy rates, and practical storage requirements make it a versatile option for global vaccination strategies. By understanding its mechanisms and adhering to recommended guidelines, individuals can confidently benefit from this vaccine’s protective effects, contributing to broader public health goals.
US Vaccination Rates: Tracking the Number of Vaccinated Americans
You may want to see also
Explore related products
![]()
Comparison to mRNA: AstraZeneca’s viral vector method differs from mRNA vaccines’ direct spike protein coding
The AstraZeneca vaccine, unlike mRNA vaccines, employs a viral vector method to deliver genetic instructions to cells. This approach hinges on a modified adenovirus, typically from chimpanzees, which acts as a Trojan horse, carrying the genetic code for the SARS-CoV-2 spike protein into human cells. Once inside, the cell’s machinery reads this code and produces the spike protein, triggering an immune response. This contrasts sharply with mRNA vaccines like Pfizer-BioNTech and Moderna, which directly inject mRNA molecules encoding the spike protein, bypassing the need for a viral intermediary.
From a practical standpoint, the viral vector method offers distinct advantages and challenges. For instance, AstraZeneca’s vaccine can be stored at standard refrigerator temperatures (2°C–8°C), making it more accessible for distribution in low-resource settings compared to mRNA vaccines, which require ultra-cold storage (-70°C for Pfizer, -20°C for Moderna). However, the viral vector approach may elicit a stronger immune reaction to the vector itself, potentially reducing the vaccine’s efficacy with repeated doses. This is why AstraZeneca’s regimen typically involves a two-dose schedule spaced 4–12 weeks apart, with careful consideration of dosing intervals to optimize immune response.
Analytically, the difference in delivery mechanisms influences not only storage and distribution but also immunogenicity and safety profiles. mRNA vaccines have demonstrated slightly higher efficacy rates in clinical trials (around 95% for Pfizer and Moderna vs. 70–80% for AstraZeneca), partly due to their direct and transient introduction of mRNA into cells. However, AstraZeneca’s vaccine has shown robust effectiveness in preventing severe disease and hospitalization, particularly in older age groups (e.g., >80% efficacy in those over 70). This highlights the importance of tailoring vaccine choice to specific populations and logistical constraints.
Persuasively, the choice between viral vector and mRNA vaccines often boils down to context. For regions with limited infrastructure, AstraZeneca’s ease of storage and lower cost ($3–4 per dose compared to $15–20 for mRNA vaccines) make it a pragmatic option. Conversely, mRNA vaccines’ higher efficacy and well-defined side effect profiles (e.g., transient fatigue, headache) may be preferred in settings where cold chain management is feasible. For individuals, consulting healthcare providers to weigh risks and benefits—such as rare blood clotting events associated with AstraZeneca in younger populations—is crucial.
Descriptively, the viral vector method’s reliance on a modified virus introduces a layer of biological complexity. The adenovirus, stripped of its ability to cause disease, still retains enough functionality to deliver the spike protein gene. This process mimics a natural viral infection, albeit in a controlled manner, which may explain the vaccine’s ability to stimulate a strong T-cell response alongside antibody production. In contrast, mRNA vaccines focus primarily on antibody generation, though both ultimately aim to prepare the immune system for a real SARS-CoV-2 encounter. Understanding these nuances empowers individuals to make informed decisions about their vaccination options.
Navigating the Vaccination Question: A Guide to Responding Confidently
You may want to see also
Frequently asked questions
The AstraZeneca vaccine does not contain the spike protein itself. Instead, it uses a modified adenovirus (ChAdOx1) to deliver genetic instructions to cells, allowing them to produce the SARS-CoV-2 spike protein temporarily.
The AstraZeneca vaccine introduces a harmless adenovirus carrying the gene for the SARS-CoV-2 spike protein. Once inside cells, this gene is expressed, prompting the cells to produce the spike protein, which then triggers an immune response.
No, the spike protein produced by the AstraZeneca vaccine is not dangerous. It is a temporary and harmless component that helps the immune system recognize and build protection against COVID-19 without causing illness.
No, the spike protein produced by the AstraZeneca vaccine does not stay in the body permanently. It is broken down and cleared by the immune system within days or weeks after vaccination.