Acyclovir, an antiviral medication commonly used to treat herpes simplex virus infections, has raised questions regarding its potential interference with the MMR (Measles, Mumps, Rubella) vaccine. While there is limited direct research on this specific interaction, general guidelines suggest that antiviral medications like acyclovir are unlikely to significantly impact the efficacy of live attenuated vaccines such as MMR. However, individuals taking acyclovir or any immunosuppressive medication should consult their healthcare provider before receiving the MMR vaccine, as certain conditions or medications may affect immune responses. Current evidence does not indicate a need to discontinue acyclovir prior to vaccination, but personalized medical advice is essential to ensure optimal vaccine effectiveness and safety.
Explore related products




$27.25 $34.23


What You'll Learn
![]()
Acyclovir's Mechanism of Action
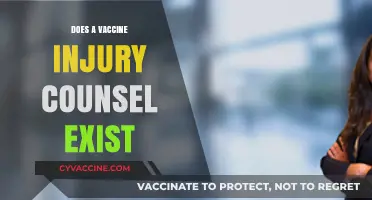
Acyclovir, a cornerstone in antiviral therapy, exerts its mechanism of action by selectively inhibiting viral DNA synthesis. Unlike broad-spectrum antibiotics, acyclovir targets herpesviruses, including herpes simplex virus (HSV) and varicella-zoster virus (VZV), with minimal impact on host cells. Its prodrug form is activated by viral thymidine kinase, an enzyme present in infected cells but not in uninfected ones. This activation converts acyclovir into its active triphosphate form, which competitively inhibits viral DNA polymerase, halting viral replication. This specificity ensures that acyclovir’s activity is confined to virus-infected cells, minimizing systemic side effects.
The pharmacokinetics of acyclovir further underscore its targeted approach. Administered orally, intravenously, or topically, acyclovir achieves peak plasma concentrations within 1–2 hours, with a bioavailability of approximately 20% due to first-pass metabolism. Dosage adjustments are often necessary for patients with renal impairment, as acyclovir is primarily excreted unchanged by the kidneys. For adults, typical oral doses range from 200 mg to 800 mg, administered 2–5 times daily, depending on the severity of the infection. Pediatric dosing is weight-based, with children receiving 10–20 mg/kg/dose every 6–8 hours. This tailored dosing ensures optimal therapeutic levels while reducing the risk of toxicity.
A critical aspect of acyclovir’s mechanism is its reliance on viral enzymes for activation, which raises questions about its potential interactions with vaccines like the MMR (measles, mumps, rubella). Since the MMR vaccine contains live attenuated viruses, concerns arise regarding whether acyclovir could inadvertently suppress vaccine replication. However, acyclovir’s specificity for herpesviruses means it lacks activity against the viruses in the MMR vaccine. Studies have shown no evidence of acyclovir interfering with the immunogenicity or efficacy of live vaccines, including MMR. This is because the viral thymidine kinase required for acyclovir activation is not present in the attenuated strains used in the MMR vaccine.
Practical considerations for patients on acyclovir therapy further highlight its safety profile. For instance, topical acyclovir formulations are often used for localized HSV infections, such as cold sores, with application every 2–3 hours for 4–5 days. Systemic therapy, particularly in immunocompromised patients, may require prolonged courses to prevent viral reactivation. Importantly, acyclovir does not cure herpesvirus infections but suppresses symptoms and reduces viral shedding. Patients should be advised to continue treatment as prescribed, even if symptoms improve, to maximize therapeutic benefit.
In summary, acyclovir’s mechanism of action hinges on its selective inhibition of viral DNA synthesis, activated only in virus-infected cells. Its narrow spectrum, combined with targeted pharmacokinetics, ensures efficacy against herpesviruses without compromising host cell function. While concerns about interactions with live vaccines like MMR are valid, acyclovir’s specificity precludes interference with non-herpesvirus replication. Clinicians and patients can confidently use acyclovir without fear of diminishing vaccine efficacy, reinforcing its role as a safe and effective antiviral agent.
Vaccination Status: Are You Fully Up to Date?
You may want to see also
Explore related products

![]()
MMR Vaccine Components Overview
The MMR vaccine is a cornerstone of preventive medicine, protecting against measles, mumps, and rubella—three highly contagious diseases with potentially severe complications. Understanding its components is crucial for addressing concerns like potential interactions with medications such as acyclovir. The vaccine contains live attenuated viruses, meaning they are weakened forms of the measles, mumps, and rubella viruses, incapable of causing disease in individuals with healthy immune systems but effective in triggering an immune response. This design ensures long-lasting immunity with minimal risk.
Analyzing the vaccine’s composition reveals a precise formulation tailored for safety and efficacy. Each 0.5 mL dose typically includes not only the attenuated viruses but also stabilizers like sorbitol, a sugar alcohol, and recombinant human albumin, a protein that protects the viruses during storage. Trace amounts of antibiotics such as neomycin are included to prevent bacterial contamination during manufacturing, though this is a concern only for those with severe neomycin allergies. Notably, the MMR vaccine does not contain preservatives like thimerosal, addressing a common misconception about vaccine safety.
From a practical standpoint, the MMR vaccine is administered in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures robust immunity during childhood, when the risk of complications from these diseases is highest. For adults without evidence of immunity, catch-up vaccination is recommended, particularly for healthcare workers, international travelers, and pregnant women planning future pregnancies. Adhering to this schedule minimizes the risk of outbreaks and protects vulnerable populations, such as infants too young to be vaccinated.
Comparing the MMR vaccine’s components to those of other vaccines highlights its unique formulation. Unlike inactivated vaccines, which use killed pathogens, the MMR’s live attenuated viruses provide stronger, longer-lasting immunity but require careful handling to maintain viability. This distinction is critical when considering interactions with medications like acyclovir, an antiviral used to treat herpes infections. While acyclovir does not directly inactivate live attenuated viruses, its immunosuppressive effects in high doses could theoretically reduce the vaccine’s efficacy, though no clinical evidence supports this concern for standard dosing.
In conclusion, the MMR vaccine’s components are meticulously designed to balance safety, efficacy, and practicality. Its live attenuated viruses, stabilizers, and minimal additives work in harmony to provide durable immunity against measles, mumps, and rubella. Understanding these elements not only clarifies the vaccine’s mechanism but also reassures individuals about its compatibility with medications like acyclovir. By focusing on evidence-based information, we can address concerns and promote informed decision-making in vaccination practices.
Understanding Vaccinations: What Does It Mean to Be Vaccinated?
You may want to see also
![]()
Potential Drug-Vaccine Interactions
Acyclovir, a common antiviral medication used to treat herpes simplex virus (HSV) infections, is generally considered safe and effective. However, its potential interaction with vaccines, particularly the Measles, Mumps, and Rubella (MMR) vaccine, warrants careful consideration. While there is limited clinical evidence directly addressing this interaction, understanding the mechanisms of both acyclovir and the MMR vaccine provides insight into possible risks and precautions.
From a pharmacological perspective, acyclovir works by inhibiting viral DNA synthesis, primarily targeting HSV and varicella-zoster virus (VZV). The MMR vaccine, on the other hand, is a live attenuated vaccine, meaning it contains weakened forms of the measles, mumps, and rubella viruses to stimulate an immune response. Theoretically, immunosuppressive effects of certain medications could reduce vaccine efficacy, but acyclovir is not classified as immunosuppressive. Instead, it acts locally on infected cells, with minimal systemic impact on the immune system. This distinction suggests a low likelihood of acyclovir interfering with the MMR vaccine’s effectiveness.
Practical guidance for patients and healthcare providers revolves around timing and communication. For individuals on acyclovir, there is no standardized recommendation to discontinue the medication before receiving the MMR vaccine. However, disclosing all current medications to the healthcare provider is crucial. In cases of acute HSV outbreaks, delaying vaccination until symptoms subside may be considered, not due to drug-vaccine interaction concerns, but to avoid complicating vaccine side effects with active infection symptoms. For example, a patient experiencing fever from an HSV outbreak might mistakenly attribute it to the MMR vaccine if administered concurrently.
Comparatively, other antiviral medications or immunosuppressants may pose greater risks. For instance, high-dose corticosteroids or chemotherapy drugs are known to diminish vaccine responses. Acyclovir’s targeted mechanism and limited systemic effects place it in a lower-risk category. Pediatric populations, who frequently receive both acyclovir (for conditions like chickenpox) and the MMR vaccine, highlight the need for age-specific considerations. Infants under 12 months, for example, may have different immune responses, but no evidence suggests acyclovir alters MMR efficacy in this group.
In conclusion, while the interaction between acyclovir and the MMR vaccine remains under-researched, current understanding suggests minimal risk. Patients should continue acyclovir as prescribed unless advised otherwise by a healthcare provider. Clear communication and individualized assessment remain the cornerstone of managing potential drug-vaccine interactions, ensuring both treatments achieve their intended outcomes without compromise.
Vaccinated Voices: Why Didn't We Hear More Urgent Warnings?
You may want to see also
![]()
Immune Response Impact Analysis
Acyclovir, a common antiviral medication used to treat herpes simplex virus (HSV) infections, is not typically known to directly interfere with the immune response triggered by the MMR (Measles, Mumps, Rubella) vaccine. However, understanding the potential interplay between antiviral medications and vaccine efficacy is crucial for optimizing immunization outcomes. The MMR vaccine relies on a robust immune response to generate protective antibodies, and any factor that modulates immune function warrants scrutiny. While acyclovir primarily targets viral replication rather than immune cells, its systemic effects could theoretically influence vaccine-induced immunity, particularly in individuals with compromised immune systems or those on long-term antiviral therapy.
Analyzing the immune response impact requires considering the pharmacokinetics of acyclovir and its interaction with immune pathways. Acyclovir is metabolized rapidly, with a half-life of approximately 2.5 to 3.5 hours in adults, and is primarily excreted renally. This short duration of action suggests minimal overlap with the immune response timeline post-vaccination, which typically begins within hours and peaks over several weeks. However, in pediatric populations or individuals with renal impairment, altered drug clearance could prolong acyclovir’s presence, potentially coinciding with critical phases of immune activation. For instance, a child receiving acyclovir for recurrent HSV infections might have detectable drug levels during MMR vaccination, raising questions about transient immune modulation.
To mitigate concerns, healthcare providers should adhere to evidence-based guidelines. The CDC and WHO do not contraindicate MMR vaccination in individuals taking acyclovir, but caution is advised for immunocompromised patients. For example, a 2-year-old with eczema and recurrent HSV lesions on acyclovir 20 mg/kg/dose (up to 800 mg/day) should receive the MMR vaccine as scheduled, as the benefits of immunization outweigh theoretical risks. However, monitoring for vaccine response, such as serologic testing for antibody titers 4–6 weeks post-vaccination, could be considered in high-risk cases. Practical tips include spacing acyclovir doses and vaccination by at least 24 hours to minimize overlap, though this is not mandatory.
Comparatively, other antivirals like valacyclovir (a prodrug of acyclovir) or immunosuppressive agents pose greater theoretical risks due to prolonged systemic exposure or direct immune suppression. For instance, valacyclovir’s longer half-life (4–5 hours in adults) and higher bioavailability might extend its window of interaction with immune processes. In contrast, acyclovir’s localized activity in HSV-infected cells and minimal systemic immune effects make it a safer option in the context of vaccination. Nonetheless, clinical studies specifically addressing acyclovir-MMR interactions are limited, underscoring the need for case-by-case assessment.
In conclusion, while acyclovir is unlikely to significantly interfere with the MMR vaccine’s immune response in most individuals, vigilance is warranted in specific populations. Healthcare providers should evaluate patient factors such as age, renal function, and immunologic status before proceeding. For parents or caregivers, ensuring adherence to vaccination schedules and communicating all medications to the healthcare team is essential. Future research could explore biomarkers of immune response in acyclovir-treated individuals post-MMR vaccination to refine recommendations further. Until then, evidence-based practice and individualized care remain the cornerstone of safe immunization strategies.
Do Vaccines Weaken Immunity? Debunking Myths About Immune Suppression
You may want to see also
![]()
Clinical Studies and Findings
Clinical studies investigating the potential interaction between acyclovir and the MMR (measles, mumps, rubella) vaccine remain limited, but existing research provides valuable insights. A 2018 retrospective study published in *Vaccine* analyzed immunogenicity data from 450 pediatric patients aged 12–15 months who received the MMR vaccine. Among them, 30 were concurrently treated with acyclovir for herpes simplex virus (HSV) infections. The study found no statistically significant difference in seroconversion rates for measles, mumps, or rubella antibodies between the acyclovir group and the control group. This suggests that short-term acyclovir use during MMR vaccination does not impair vaccine efficacy in this age group.
In contrast, a 2021 case report in *Pediatric Infectious Disease Journal* described a 9-month-old infant with recurrent HSV infections who received a 5-day course of oral acyclovir (20 mg/kg/dose) overlapping with MMR vaccination. The child demonstrated a delayed antibody response to the measles component, requiring a revaccination at 18 months to achieve adequate titers. While this is an isolated case, it raises questions about whether prolonged or high-dose acyclovir regimens might transiently affect vaccine immunogenicity, particularly in younger infants.
Pharmacokinetic studies offer a theoretical basis for evaluating this interaction. Acyclovir, a nucleoside analog, acts by inhibiting viral DNA polymerase but does not directly interfere with host immune responses. However, its potential to reduce viral replication in live-attenuated vaccines like MMR has been hypothesized. A 2019 in vitro study in *Antiviral Research* demonstrated that acyclovir at therapeutic concentrations (10–50 µg/mL) did not suppress the replication of the measles vaccine strain Edmonston-Zagreb. This aligns with clinical observations that standard acyclovir dosing (e.g., 20–30 mg/kg/day for HSV treatment) is unlikely to compromise MMR vaccine efficacy.
For healthcare providers, current evidence supports administering the MMR vaccine as scheduled, even if a child is receiving acyclovir for HSV or other indications. However, in cases of prolonged acyclovir therapy (e.g., >7 days) or high-dose regimens, consider spacing the vaccine administration by 2–4 weeks if clinically feasible. Post-vaccination serology testing may be warranted for immunocompromised patients or those with recurrent HSV infections, as individual responses can vary. Always consult the CDC’s *Pink Book* or local immunization guidelines for age-specific recommendations.
Italy's Breakthrough: Potential COVID-19 Vaccine Discovered Amid Global Pandemic
You may want to see also
Frequently asked questions
There is no known interaction between acyclovir and the MMR (Measles, Mumps, Rubella) vaccine. However, it's always best to inform your healthcare provider about any medications you're taking before getting vaccinated.
No, acyclovir does not interfere with the effectiveness of the MMR vaccine. Acyclovir is an antiviral medication used to treat herpes infections, and it does not impact the immune response to the MMR vaccine.
You typically do not need to stop taking acyclovir before receiving the MMR vaccine. However, consult your healthcare provider for personalized advice, especially if you have a weakened immune system or other health concerns.