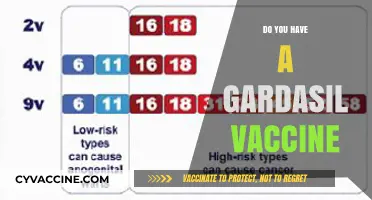
The question of whether we truly need more vaccines is a complex and multifaceted issue that sparks debate among scientists, healthcare professionals, and the public. While vaccines have historically been one of the most effective tools in preventing infectious diseases and saving millions of lives, the development of new vaccines must be carefully evaluated based on factors such as disease prevalence, severity, and existing immunity. Critics argue that over-vaccination or unnecessary vaccines could lead to resource wastage, potential side effects, or public mistrust, while proponents emphasize the importance of preparedness for emerging pathogens and the prevention of outbreaks. Striking a balance between innovation and necessity is crucial to ensuring that vaccine efforts align with global health priorities and public trust.
Explore related products






What You'll Learn
- Historical Success of Vaccines: Eradication of diseases like smallpox, polio reduction through global vaccination efforts
- Herd Immunity Importance: Protecting vulnerable populations by achieving high community vaccination rates
- Vaccine Safety Myths: Debunking misinformation about vaccine side effects and long-term health risks
- Economic Impact Analysis: Cost savings from prevented illnesses vs. vaccine development and distribution expenses
- Ethical Considerations: Balancing individual choice with public health responsibility in vaccine mandates
![]()
Historical Success of Vaccines: Eradication of diseases like smallpox, polio reduction through global vaccination efforts
The eradication of smallpox stands as one of the most monumental achievements in medical history, a testament to the power of global vaccination efforts. By 1980, the World Health Organization (WHO) declared smallpox eradicated, marking the first and only time a human disease has been completely eliminated. This success was achieved through a coordinated campaign that included mass vaccination with the Dryvax vaccine, ring vaccination (targeting contacts of infected individuals), and rigorous surveillance. The vaccine, administered via a bifurcated needle, required a single dose to confer immunity, though a booster was recommended every 10 years for sustained protection. This example underscores the potential of vaccines to not only control but entirely eliminate a disease when deployed strategically and universally.
Contrast smallpox with polio, a disease that, while not eradicated, has been reduced by over 99% since 1988 due to global vaccination initiatives. The Global Polio Eradication Initiative (GPEI) has been instrumental in this effort, utilizing both the oral polio vaccine (OPV) and the inactivated polio vaccine (IPV). OPV, administered as drops, is particularly effective in inducing intestinal immunity and stopping person-to-person spread, making it ideal for mass campaigns in endemic regions. IPV, given as an injection, provides individual protection without the rare risk of vaccine-derived polio associated with OPV. Children typically receive a series of 3–4 doses starting at 2 months of age, with boosters recommended in high-risk areas. The near-elimination of polio highlights how sustained vaccination efforts can bring a disease to the brink of eradication, even in the face of logistical and societal challenges.
Analyzing these successes reveals a common thread: the importance of global cooperation and infrastructure. Smallpox eradication required not just a vaccine but a worldwide commitment to surveillance, containment, and accessibility. Similarly, polio reduction has relied on partnerships between governments, NGOs, and local communities to reach even the most remote populations. For instance, in Nigeria, one of the last polio-endemic countries, door-to-door vaccination campaigns and community engagement were critical to overcoming skepticism and logistical hurdles. These examples demonstrate that vaccines are not just medical tools but catalysts for collective action, requiring robust systems to ensure equitable distribution and uptake.
A cautionary note emerges when comparing these successes to current vaccination challenges. While smallpox and polio efforts benefited from clear, measurable goals and global consensus, modern vaccine campaigns often face misinformation, political resistance, and resource disparities. For instance, the COVID-19 vaccine rollout highlighted how vaccine hesitancy and inequitable distribution can hinder progress. To replicate historical successes, we must address these barriers through transparent communication, community involvement, and strengthened healthcare systems. Practical steps include investing in cold chain infrastructure for vaccine storage, training healthcare workers, and leveraging technology for real-time monitoring of vaccination rates.
In conclusion, the historical success of vaccines in eradicating smallpox and nearly eliminating polio provides a blueprint for tackling other infectious diseases. These achievements were not merely scientific triumphs but the result of coordinated global efforts, strategic planning, and unwavering commitment. As we confront new and evolving health threats, the lessons from smallpox and polio remind us that vaccines are indispensable tools—but their potential can only be fully realized through collaboration, innovation, and equitable access. By studying these successes, we can chart a path forward to protect future generations from preventable diseases.
The Lasting Mark: Why the Old Polio Vaccine Left a Scar
You may want to see also
Explore related products






![]()
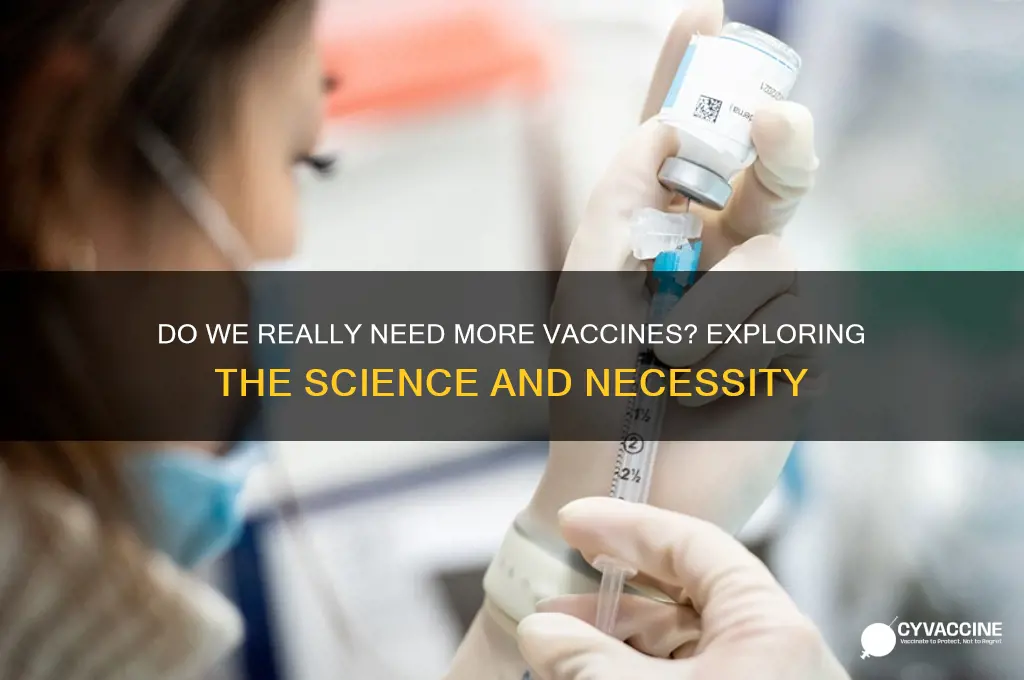
Herd Immunity Importance: Protecting vulnerable populations by achieving high community vaccination rates
Vaccination rates above 80-90% create herd immunity, a protective shield that safeguards those who cannot receive vaccines due to medical reasons. This includes individuals with compromised immune systems, severe allergies to vaccine components, or certain chronic conditions. For example, a fully vaccinated community significantly reduces the circulation of measles, a highly contagious virus. With a basic reproduction number (R0) of 12-18, meaning one infected person can spread it to 12-18 others, achieving a vaccination rate of 93-95% is crucial to prevent outbreaks and protect vulnerable populations.
Consider the impact on infants too young for certain vaccines. The MMR vaccine, which protects against measles, mumps, and rubella, is administered in two doses, the first at 12-15 months. Until then, babies rely on herd immunity. Similarly, individuals undergoing chemotherapy or organ transplants have weakened immune systems, making them susceptible to vaccine-preventable diseases. High community vaccination rates act as a buffer, reducing their exposure to pathogens.
Achieving herd immunity requires a collective effort. Vaccines like the flu shot, which has a variable efficacy rate (40-60% in most seasons), still play a vital role in protecting vulnerable populations. Even if vaccinated individuals contract the flu, their symptoms are typically milder, reducing the risk of severe complications in those around them. This concept of "cocooning" through herd immunity is particularly important for the elderly, who may have diminished immune responses to vaccines.
To contribute to herd immunity, follow these practical steps: ensure your vaccinations are up-to-date, including boosters for diseases like tetanus (every 10 years) and pertussis (Tdap recommended during each pregnancy). Encourage friends and family to vaccinate, especially those in close contact with vulnerable individuals. Stay informed about local vaccination rates and advocate for policies that promote vaccine accessibility. Remember, herd immunity is not just a personal choice but a community responsibility, protecting those who cannot protect themselves.
Recombinant Rabies Vaccine 3-Year Brand for Cats Explained
You may want to see also
Explore related products






![]()
Vaccine Safety Myths: Debunking misinformation about vaccine side effects and long-term health risks
Misinformation about vaccine side effects often exaggerates their severity, creating unwarranted fear. For instance, claims that the measles, mumps, and rubella (MMR) vaccine causes autism have been thoroughly debunked by numerous studies involving millions of children. The original 1998 paper linking the two was retracted due to ethical violations and fraudulent data. Side effects from vaccines are typically mild—fever, soreness, or fatigue—and resolve within days. Severe reactions, such as anaphylaxis, occur in fewer than 1 in a million doses. Understanding these facts helps distinguish between rare, manageable risks and baseless myths.
Consider the flu vaccine, often criticized for its alleged ineffectiveness or harmfulness. While it’s true the vaccine’s efficacy varies annually (40–60% on average), it significantly reduces hospitalization and death, especially in high-risk groups like the elderly and immunocompromised. Claims that it causes the flu are false—the vaccine contains inactivated or weakened viruses incapable of causing illness. For those hesitant about additives like thimerosal, it’s worth noting that this preservative has been removed from most childhood vaccines since 2001, with no change in autism rates. This demonstrates how misinformation persists long after evidence disproves it.
Long-term health risks are another common myth, with some fearing vaccines cause chronic conditions like autoimmune disorders or infertility. Studies show no link between vaccines and these outcomes. For example, the HPV vaccine, which prevents cervical cancer, has been administered to over 130 million people worldwide with no evidence of long-term harm. Similarly, the COVID-19 vaccines underwent rigorous testing and continue to be monitored through systems like VAERS (Vaccine Adverse Event Reporting System). Rare side effects, such as myocarditis (inflammation of the heart muscle), occur in approximately 1 in 100,000 young males but are far less risky than the complications of COVID-19 itself.
To combat misinformation, focus on credible sources like the CDC, WHO, or peer-reviewed journals. When evaluating claims, ask: Is the source biased? Are studies cited, and are they large-scale or anecdotal? For parents, discuss concerns with pediatricians, who can provide tailored advice. Practical tips include scheduling vaccines when children are well-rested and using pain relievers like acetaminophen for post-vaccine discomfort. By grounding decisions in evidence, individuals can protect themselves and their communities from both diseases and misinformation.
Discovering the Brand Name of the RSV Vaccine: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Economic Impact Analysis: Cost savings from prevented illnesses vs. vaccine development and distribution expenses
Vaccine development and distribution are significant investments, often costing billions of dollars from research to rollout. For instance, the COVID-19 vaccine development alone required over $10 billion in initial funding, with additional expenses for manufacturing, logistics, and administration. These upfront costs are substantial, but they pale in comparison to the potential economic burden of unchecked illnesses. Consider the 2009 H1N1 pandemic, which cost the global economy an estimated $55 billion due to lost productivity, healthcare expenses, and preventive measures. The question isn’t whether vaccines are expensive—it’s whether we can afford *not* to invest in them.
To evaluate the economic impact, compare the cost of vaccine programs to the savings from prevented illnesses. A single dose of the measles vaccine costs approximately $1–2, yet measles outbreaks can lead to hospitalization costs exceeding $10,000 per patient. In 2019, the U.S. experienced 1,282 measles cases, resulting in an estimated $20–30 million in direct medical expenses. If 95% vaccination coverage had been maintained, these costs—along with indirect losses from school closures and productivity declines—could have been avoided. This example illustrates how modest vaccine investments yield disproportionate returns by preventing costly outbreaks.
A step-by-step analysis reveals the long-term economic benefits of vaccination. First, calculate the total cost of vaccine development, production, and distribution per dose. For the HPV vaccine, this averages $130 per course. Next, quantify the prevented illness costs, including medical treatment, lost wages, and disability. HPV-related cancers cost the U.S. healthcare system $5 billion annually, but vaccination reduces cervical cancer cases by 90%. Finally, compare the two figures: the $130 vaccine expense versus the $5 billion in avoided costs. The conclusion is clear—vaccines are not just a health intervention but a cost-saving economic strategy.
Critics argue that vaccine distribution in low-income regions is inefficient, but evidence suggests otherwise. Gavi, the Vaccine Alliance, has immunized over 980 million children in developing countries since 2000, preventing 16.4 million deaths. The economic return on this $20 billion investment? An estimated $150 billion in healthcare savings and productivity gains. Practical tips for maximizing impact include prioritizing high-risk age groups (e.g., children under 5 and adults over 65) and leveraging existing healthcare infrastructure to reduce distribution costs. When executed strategically, vaccination programs deliver unparalleled economic value.
Ultimately, the debate over vaccine necessity hinges on a cost-benefit analysis. While development and distribution expenses are tangible, the savings from prevented illnesses—both direct and indirect—far outweigh the initial outlay. For every dollar spent on childhood immunizations, societies yield $44 in economic benefits. This isn’t merely a health imperative; it’s a financial one. By framing vaccines as an investment rather than an expense, policymakers and stakeholders can make informed decisions that protect both public health and economic stability.
Can You Still Catch COVID-19 After Getting Vaccinated?
You may want to see also
Explore related products






![]()
Ethical Considerations: Balancing individual choice with public health responsibility in vaccine mandates
Vaccine mandates ignite a fiery debate between individual autonomy and collective well-being. At the heart of this ethical dilemma lies a fundamental question: where do we draw the line between personal choice and societal responsibility? This tension is particularly acute in the context of infectious diseases like measles, mumps, and rubella (MMR), where vaccination not only protects the individual but also contributes to herd immunity, shielding vulnerable populations who cannot be vaccinated due to medical reasons.
Consider the MMR vaccine, typically administered in two doses, the first at 12-15 months and the second at 4-6 years. This vaccine boasts a remarkable efficacy rate of 97% after two doses, drastically reducing the transmission of these highly contagious diseases. Yet, despite its proven benefits, vaccine hesitancy persists, fueled by misinformation, historical mistrust, and concerns about potential side effects, which are overwhelmingly mild and short-lived, such as fever or soreness at the injection site.
Proponents of mandates argue that they are a necessary public health tool, particularly in the face of outbreaks. They point to historical successes, like the eradication of smallpox, achieved through widespread vaccination campaigns. Opponents, however, view mandates as an infringement on personal liberty, arguing that individuals should have the right to make informed decisions about their own bodies. This clash of principles demands a nuanced approach, one that acknowledges the validity of both concerns.
A potential solution lies in striking a balance through a multi-pronged strategy. Firstly, robust public education campaigns are crucial, addressing misinformation and fostering trust in scientific evidence. Secondly, offering easily accessible vaccination services, including mobile clinics and school-based programs, can remove logistical barriers. Finally, implementing targeted mandates for high-risk groups, such as healthcare workers or students in crowded settings, can be justified on the grounds of protecting vulnerable populations without imposing blanket restrictions on the entire population.
Ultimately, the ethical dilemma surrounding vaccine mandates requires a delicate dance between individual rights and collective responsibility. By prioritizing transparency, accessibility, and targeted interventions, we can navigate this complex landscape, ensuring both personal freedoms and the health of our communities.
FDA-Approved COVID-19 Vaccine Release Date: What You Need to Know
You may want to see also
Frequently asked questions
Yes, the MMR vaccine is still essential because these diseases can spread quickly in unvaccinated populations, and outbreaks can occur even in countries where they are rare.
The MMR vaccine is safe and highly effective. Serious side effects are extremely rare, and the benefits of protection against measles, mumps, and rubella far outweigh any risks.
No, extensive scientific research has conclusively shown that there is no link between the MMR vaccine and autism. This myth has been thoroughly debunked by the medical community.
Yes, adults who are unsure of their vaccination status or were not fully vaccinated as children should get the MMR vaccine, especially if they are at risk of exposure to these diseases.