The question of whether vaccines still contain Adjuvant 65 is a topic of interest, particularly as adjuvants play a crucial role in enhancing the immune response to vaccines. Adjuvant 65, also known as aluminum hydroxide, has been historically used in various vaccines to improve their efficacy. However, its presence in modern vaccines varies depending on the specific vaccine and its formulation. While some vaccines continue to utilize aluminum-based adjuvants, including derivatives of Adjuvant 65, others have transitioned to alternative adjuvants or adjuvant-free formulations. This shift is driven by advancements in vaccine technology, safety considerations, and the development of more targeted immune-enhancing components. As a result, the inclusion of Adjuvant 65 is no longer universal, and its use is carefully evaluated on a case-by-case basis to ensure optimal safety and efficacy in vaccine development.
| Characteristics | Values |
|---|---|
| Adjuvant 65 Usage | Adjuvant 65, also known as aluminum hydroxide, is still used in some vaccines as an adjuvant to enhance the immune response. |
| Current Vaccines with Adjuvant 65 | Examples include certain formulations of DTaP (diphtheria, tetanus, pertussis), hepatitis A, hepatitis B, and pneumococcal vaccines. |
| Purpose of Adjuvant 65 | To increase the body's immune response to the vaccine antigen, improving vaccine efficacy and duration of protection. |
| Safety Profile | Widely considered safe, with extensive research supporting its use in vaccines for decades. |
| Side Effects | Mild and transient, such as soreness, redness, or swelling at the injection site. |
| Regulatory Approval | Approved by major regulatory bodies like the FDA, EMA, and WHO for use in vaccines. |
| Alternatives | Other adjuvants like AS04 (aluminum hydroxide and MPL) and MF59 (squalene-based) are also used in some vaccines. |
| Research and Development | Ongoing research to optimize adjuvant use, but Adjuvant 65 remains a standard due to its proven safety and efficacy. |
| Public Perception | Generally accepted, though misinformation about adjuvants persists, necessitating public education. |
| Future Trends | Continued use expected, with potential for new adjuvants to complement or replace Adjuvant 65 in specific vaccines. |
Explore related products






What You'll Learn
- Aluminum Adjuvants in Vaccines: Most vaccines use aluminum salts as adjuvants to enhance immune response
- Adjuvant 65 vs. Modern Adjuvants: Adjuvant 65 is outdated; newer, safer adjuvants are now used
- Safety of Aluminum Adjuvants: Extensive research confirms aluminum adjuvants are safe and effective in vaccines
- Adjuvant-Free Vaccines: Some vaccines, like mRNA COVID-19 vaccines, do not contain adjuvants
- Historical Use of Adjuvant 65: Adjuvant 65 was once used but has been replaced by advanced alternatives
![]()
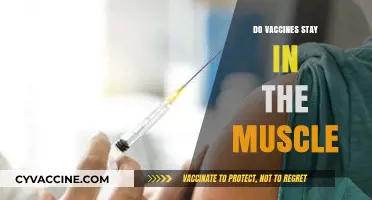
Aluminum Adjuvants in Vaccines: Most vaccines use aluminum salts as adjuvants to enhance immune response
Aluminum adjuvants, typically in the form of aluminum salts like aluminum hydroxide, aluminum phosphate, or potassium aluminum sulfate, are a cornerstone of modern vaccine formulation. These compounds have been used for nearly a century to enhance the immune response to vaccines, ensuring that the body produces sufficient antibodies to protect against disease. Unlike the live or weakened pathogens in some vaccines, aluminum adjuvants act as immunological accelerants, priming the immune system to recognize and respond to the antigen more effectively. This mechanism is particularly crucial for vaccines containing inactivated or subunit antigens, which alone might not elicit a robust immune reaction.
The safety and efficacy of aluminum adjuvants are well-documented, with extensive research supporting their use in vaccines. For instance, the amount of aluminum in vaccines is meticulously regulated, typically ranging from 0.125 to 0.85 milligrams per dose, depending on the vaccine. To put this in perspective, infants receive less aluminum from vaccines in their first year of life than they do from breast milk or infant formula over the same period. Regulatory bodies like the FDA and WHO continually monitor aluminum adjuvants to ensure they remain within safe limits, particularly for vulnerable populations such as infants and the elderly.
One common misconception is that aluminum adjuvants are linked to long-term health risks, such as neurological disorders or chronic illnesses. However, decades of scientific inquiry have found no credible evidence to support these claims. Studies have consistently shown that the aluminum in vaccines is rapidly cleared from the body, primarily through the kidneys, and does not accumulate in tissues. Moreover, the immune response triggered by aluminum adjuvants is localized, minimizing systemic exposure and potential side effects. This safety profile, combined with their proven efficacy, makes aluminum adjuvants an indispensable tool in vaccine development.
Practical considerations for healthcare providers and parents include understanding the role of aluminum adjuvants in vaccine schedules. For example, the DTaP (diphtheria, tetanus, and pertussis) vaccine for infants contains aluminum hydroxide, while the hepatitis B vaccine uses aluminum phosphate. Parents should be reassured that these adjuvants are not only safe but essential for ensuring the vaccine’s effectiveness. Additionally, spacing out vaccines to avoid aluminum accumulation is unnecessary, as the body efficiently processes the small amounts present in each dose. Clear communication about the benefits and safety of aluminum adjuvants can help build trust and reduce vaccine hesitancy.
In conclusion, aluminum adjuvants remain a vital component of vaccines, enhancing immune responses without compromising safety. Their long history of use, coupled with rigorous regulatory oversight, underscores their reliability in preventing infectious diseases. As vaccine technology evolves, aluminum salts continue to play a critical role, ensuring that vaccines remain effective across diverse populations and age groups. Understanding their function and safety can empower individuals to make informed decisions about vaccination, contributing to broader public health goals.
Vaccine Mix-Up: Consequences of Vaccinating Mia Instead of Zoie
You may want to see also
Explore related products






![]()
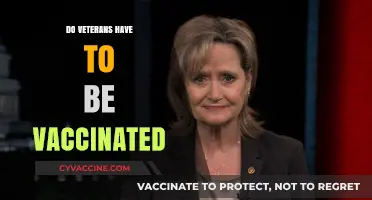
Adjuvant 65 vs. Modern Adjuvants: Adjuvant 65 is outdated; newer, safer adjuvants are now used
Adjuvant 65, once a cornerstone in vaccine formulations, has largely been phased out in favor of newer, more advanced alternatives. This shift is driven by the evolution of vaccine technology and a deeper understanding of immunology. Modern adjuvants, such as AS03 (used in pandemic influenza vaccines) and CpG 1018 (found in the hepatitis B vaccine), are designed to enhance immune responses more efficiently while minimizing side effects. Unlike Adjuvant 65, which was associated with localized reactions like redness and swelling, these newer adjuvants are engineered to target specific immune pathways, ensuring a more controlled and robust response.
Consider the practical implications for vaccine recipients. Adjuvant 65, typically composed of aluminum salts, was often used in doses ranging from 0.1 to 1.0 mg per injection. While effective, it sometimes caused discomfort, particularly in pediatric populations. Modern adjuvants, however, are used in significantly lower quantities—for instance, AS03 contains 10.69 mg of DL-α-tocopherol and 11.86 mg of squalene per dose—yet they achieve superior immunogenicity. This precision reduces the likelihood of adverse reactions, making vaccines more tolerable for individuals of all age groups, from infants to the elderly.
From a comparative standpoint, the transition from Adjuvant 65 to modern adjuvants reflects a broader trend in vaccine development: the prioritization of safety and efficacy. Adjuvant 65, while groundbreaking in its time, lacked the specificity of contemporary alternatives. For example, the TLR4 agonist GLA-AF, used in experimental vaccines, activates innate immune cells with minimal off-target effects. This targeted approach not only enhances vaccine effectiveness but also aligns with current regulatory standards, which demand rigorous safety profiles for all vaccine components.
For healthcare providers and policymakers, the takeaway is clear: Adjuvant 65 is a relic of past vaccine formulations, and its use has been largely discontinued in favor of safer, more effective options. When reviewing vaccine ingredients or advising patients, it’s crucial to emphasize that modern adjuvants are the result of decades of research and innovation. Practical tips include staying informed about vaccine formulations through resources like the CDC’s Vaccine Excipient & Media Summary and educating patients about the benefits of updated adjuvant technologies. By doing so, trust in vaccination programs can be strengthened, ensuring broader public health protection.
Unvaccinated Children: Risk to Vaccinated Peers or Misunderstood Threat?
You may want to see also
Explore related products






![]()
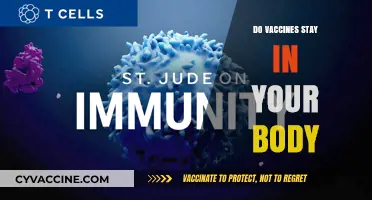
Safety of Aluminum Adjuvants: Extensive research confirms aluminum adjuvants are safe and effective in vaccines
Aluminum adjuvants have been a cornerstone of vaccine technology for nearly a century, enhancing the immune response to antigens and ensuring the efficacy of many life-saving vaccines. Despite their long history of use, concerns about their safety persist, particularly regarding their potential to cause adverse effects. However, extensive research, including numerous clinical trials and post-market surveillance studies, has consistently demonstrated that aluminum adjuvants are both safe and effective. For instance, the amount of aluminum in vaccines is meticulously regulated, typically ranging from 0.125 to 0.85 milligrams per dose, which is significantly lower than the daily aluminum intake from food, water, and other sources. This regulated dosage ensures that vaccines remain within safe limits while effectively boosting immunity.
One of the most compelling pieces of evidence supporting the safety of aluminum adjuvants comes from their widespread use in vaccines administered to billions of people globally. Vaccines like DTaP (diphtheria, tetanus, and pertussis), hepatitis B, and HPV vaccines all contain aluminum adjuvants and have been rigorously tested across diverse populations, including infants, children, and adults. Studies have shown that the incidence of serious adverse events linked to aluminum adjuvants is extremely rare. For example, a 2011 review by the Institute of Medicine found no evidence of long-term health issues associated with aluminum-containing vaccines. This robust safety profile is further reinforced by ongoing monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States, which continuously evaluates vaccine safety in real-world settings.
Critics often raise concerns about the potential for aluminum to accumulate in the body and cause harm, particularly in infants and young children. However, research has shown that the body efficiently eliminates aluminum from vaccines, with studies indicating that more than 95% of the aluminum from a vaccine dose is excreted within two days. Additionally, the aluminum in vaccines is in the form of aluminum salts, which are less bioavailable than other forms of aluminum, further minimizing any potential risk. Pediatricians and health organizations, including the World Health Organization (WHO), emphasize that the benefits of vaccination far outweigh any hypothetical risks associated with aluminum adjuvants, especially considering the severe diseases they prevent.
Practical considerations for parents and healthcare providers include understanding that aluminum adjuvants are not present in all vaccines. For example, live attenuated vaccines like MMR (measles, mumps, rubella) do not contain aluminum. When discussing vaccines with patients, healthcare providers should highlight the rigorous testing and regulation that aluminum adjuvants undergo, as well as the decades of safe use. Parents can also be reassured by the fact that vaccine schedules are designed to minimize aluminum exposure while maximizing protection, with doses spaced out to allow for proper elimination of the adjuvant. For those with specific concerns, consulting a healthcare professional for personalized advice is always recommended.
In conclusion, the safety and efficacy of aluminum adjuvants in vaccines are supported by a vast body of scientific evidence. Their role in enhancing immune responses has been critical in preventing millions of deaths and reducing the global burden of infectious diseases. By understanding the facts and relying on credible research, individuals can make informed decisions about vaccination, confident in the knowledge that aluminum adjuvants are a safe and essential component of modern vaccines.
Vaccines and Pediatric Cancers: Unraveling the Scientific Connection
You may want to see also
Explore related products






![]()
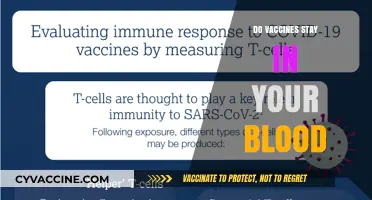
Adjuvant-Free Vaccines: Some vaccines, like mRNA COVID-19 vaccines, do not contain adjuvants
Adjuvants, substances added to vaccines to enhance the immune response, have been a staple in vaccine formulation for decades. However, not all vaccines rely on these additives. A notable example is the mRNA COVID-19 vaccines, such as those developed by Pfizer-BioNTech and Moderna. These vaccines operate on a fundamentally different mechanism, delivering genetic material that instructs cells to produce a harmless piece of the virus’s spike protein, triggering an immune response without the need for adjuvants. This innovation marks a significant shift in vaccine design, prioritizing precision and minimalism in their composition.
From a practical standpoint, adjuvant-free vaccines like the mRNA COVID-19 shots offer distinct advantages. For instance, the Pfizer vaccine is administered in a two-dose series, typically 3–4 weeks apart for individuals aged 12 and older, while a lower dosage is used for children aged 5–11. The absence of adjuvants reduces the likelihood of certain side effects, such as localized swelling or redness, which are more commonly associated with adjuvanted vaccines. This makes them particularly suitable for populations with heightened sensitivity or specific medical conditions, ensuring broader accessibility.
The development of adjuvant-free vaccines also reflects a broader trend in medical science toward personalized and targeted therapies. Unlike traditional vaccines, which often use a one-size-fits-all approach, mRNA technology can be rapidly adapted to address new variants or pathogens. For example, the COVID-19 mRNA vaccines were updated in 2022 and 2023 to include components targeting the Omicron subvariants, demonstrating their flexibility. This adaptability positions adjuvant-free vaccines as a cornerstone of future pandemic responses and routine immunizations.
Despite their advantages, adjuvant-free vaccines are not without challenges. mRNA vaccines, for instance, require ultra-cold storage conditions—the Pfizer vaccine must be stored at -90°C to -60°C—which can complicate distribution, particularly in low-resource settings. Additionally, their novelty means long-term efficacy and safety data are still emerging, though current studies indicate robust protection and minimal severe side effects. As research progresses, these vaccines may become even more refined, further solidifying their role in modern immunology.
In conclusion, adjuvant-free vaccines represent a paradigm shift in vaccine development, exemplified by the mRNA COVID-19 vaccines. Their targeted mechanism, reduced side effects, and adaptability make them a powerful tool in public health. While logistical hurdles remain, ongoing advancements promise to address these challenges, ensuring that adjuvant-free vaccines continue to play a pivotal role in global disease prevention.
Vaccine Eligibility Check: A Step-by-Step Guide to Determine Your Status
You may want to see also
Explore related products






![]()
Historical Use of Adjuvant 65: Adjuvant 65 was once used but has been replaced by advanced alternatives
Adjuvant 65, a mineral oil-based substance, was once a cornerstone of vaccine formulation, particularly in veterinary medicine. Its primary role was to enhance the immune response to antigens, ensuring that vaccines provided robust and lasting protection. Historically, Adjuvant 65 was favored for its ability to prolong antigen release at the injection site, thereby stimulating a stronger immune reaction. However, its use was not without challenges. The adjuvant was associated with adverse reactions, including granulomas and abscesses at the injection site, which raised concerns about its safety and efficacy. These issues prompted researchers to seek safer and more effective alternatives, marking the beginning of Adjuvant 65’s decline in vaccine formulations.
The transition away from Adjuvant 65 began in the late 20th century as advancements in immunology and vaccine technology accelerated. Modern adjuvants, such as aluminum salts (alum), oil-in-water emulsions, and novel immunostimulatory molecules, emerged as superior alternatives. For instance, alum, which is widely used in human vaccines, offers a favorable safety profile and effectively enhances immune responses without the severe local reactions associated with Adjuvant 65. Similarly, oil-in-water emulsions, like MF59 and AS03, have been developed to provide stronger and more durable immunity, particularly in influenza and pandemic vaccines. These advancements rendered Adjuvant 65 obsolete in most applications, as newer adjuvants could achieve better outcomes with fewer risks.
The replacement of Adjuvant 65 also reflects evolving regulatory standards and public expectations for vaccine safety. Regulatory bodies, such as the FDA and EMA, have increasingly prioritized adjuvants with well-characterized safety profiles and minimal side effects. Adjuvant 65’s tendency to cause persistent local reactions made it a poor fit for these stricter criteria. Additionally, public awareness of vaccine ingredients has grown, with consumers demanding transparency and safety in vaccine formulations. The shift to advanced adjuvants aligns with these expectations, ensuring that vaccines remain both effective and well-tolerated.
Practically, the historical use of Adjuvant 65 serves as a cautionary tale for vaccine development. While it played a crucial role in early vaccine formulations, its limitations highlight the importance of continuous innovation in adjuvant technology. For veterinarians and immunologists, understanding this history underscores the need to balance immunogenicity with safety when selecting adjuvants. Today, Adjuvant 65 is rarely, if ever, used in modern vaccines, having been entirely replaced by alternatives that offer superior performance and safety profiles. This evolution demonstrates the dynamic nature of vaccine science and its commitment to improving public and animal health.
Is There a West Nile Vaccine? Exploring Prevention and Protection
You may want to see also
Frequently asked questions
No, Adjuvant 65 (also known as AS02) is not currently used in any routinely administered vaccines. It was primarily used in the past, such as in the Cervarix HPV vaccine, but has been phased out in favor of other adjuvants or formulations.
Adjuvant 65 was used to enhance the immune response to the vaccine, making it more effective with smaller amounts of antigen. It contained components like aluminum hydroxide, monophosphoryl lipid A (MPL), and QS-21, which stimulated the immune system.
Adjuvant 65 was discontinued due to the development of newer adjuvants and vaccine formulations that offered similar or improved efficacy with fewer side effects. Additionally, some vaccines no longer required adjuvants due to advancements in vaccine technology.
Yes, some vaccines still use adjuvants, but they are different from Adjuvant 65. For example, the AS03 adjuvant (used in some pandemic influenza vaccines) and aluminum salts (commonly used in vaccines like DTaP and hepatitis B) are still in use, but they have distinct compositions and mechanisms.