Tuberculosis (TB) remains a significant global health concern, prompting questions about the current status of TB vaccination programs. The Bacille Calmette-Guérin (BCG) vaccine, developed in the early 20th century, is the primary tool for preventing severe forms of TB, particularly in children. While it is widely administered in countries with high TB prevalence, its use varies globally. In low-incidence regions like the United States, BCG vaccination is not routinely given to the general population due to its limited effectiveness against pulmonary TB in adults and the low risk of exposure. However, it is still recommended for specific high-risk groups, such as healthcare workers or individuals traveling to endemic areas. Thus, while TB vaccination practices differ by region, the BCG vaccine remains a critical component of TB prevention strategies in many parts of the world.
| Characteristics | Values |
|---|---|
| Current Use of BCG Vaccine | Yes, but not universally. Primarily used in countries with high TB prevalence. |
| Countries with Universal BCG Vaccination | Most low- and middle-income countries with high TB burden (e.g., India, South Africa, Brazil). |
| Countries without Universal BCG Vaccination | Most high-income countries with low TB incidence (e.g., USA, Canada, Western Europe). |
| Target Population | Newborns and infants in high-risk areas. Occasionally used for high-risk adults (e.g., healthcare workers). |
| Effectiveness | ~50% protection against severe TB forms (e.g., meningitis, miliary TB); variable protection against pulmonary TB. |
| Duration of Protection | 10–15 years, with waning immunity over time. |
| Side Effects | Generally safe; rare side effects include local abscess, ulceration, or disseminated BCG infection (in immunocompromised individuals). |
| Alternative Strategies | In low-incidence countries, targeted testing and treatment of latent TB infection (LTBI) are preferred over vaccination. |
| Research and Development | New TB vaccines (e.g., M72/AS01E) are under development to improve efficacy and replace or complement BCG. |
| WHO Recommendation | BCG vaccination at birth in countries with high TB prevalence; not recommended for low-incidence countries unless specific risk factors exist. |
| Global TB Burden | ~10 million new TB cases annually (2022); BCG remains a key tool in high-burden settings despite limitations. |
Explore related products






What You'll Learn
- BCG Vaccine Availability: Current global distribution and accessibility of the TB vaccine
- High-Risk Groups: Who still receives TB vaccination in targeted populations
- Vaccine Effectiveness: Efficacy of the BCG vaccine in preventing TB infections
- Alternative Treatments: Emerging TB prevention methods beyond traditional vaccination
- Country-Specific Policies: Variations in TB vaccination practices worldwide
![]()
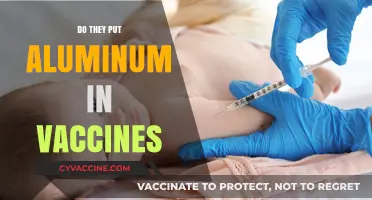
BCG Vaccine Availability: Current global distribution and accessibility of the TB vaccine
The Bacille Calmette- Guérin (BCG) vaccine, developed in the 1920s, remains the only licensed vaccine against tuberculosis (TB). Despite its age, its global distribution and accessibility vary widely, influenced by factors such as disease prevalence, healthcare infrastructure, and policy decisions. In high-burden TB countries like India and South Africa, universal childhood vaccination is standard, often administered within the first few days of life. However, in low-incidence regions, such as the United States and most of Western Europe, BCG vaccination is typically reserved for high-risk groups, including healthcare workers and infants with TB-positive family members. This disparity highlights the vaccine’s role as both a preventive measure and a subject of strategic allocation.
Analyzing the current distribution reveals a patchwork of accessibility. The World Health Organization (WHO) estimates that over 100 countries include BCG vaccination in their national immunization programs, primarily targeting newborns. The vaccine is administered as a single intradermal dose of 0.05 mL, containing 0.05–0.82 mg of lyophilized vaccine. Despite its widespread use, supply chain challenges persist, particularly in low-resource settings. For instance, cold chain requirements and limited production capacity can disrupt availability, leaving vulnerable populations at risk. Additionally, the vaccine’s variable efficacy—ranging from 0% to 80% depending on geographic location—complicates its universal adoption, prompting some countries to reconsider its inclusion in routine immunization schedules.
From a practical standpoint, individuals seeking BCG vaccination outside national programs face significant hurdles. In non-endemic countries, obtaining the vaccine often requires a prescription and may involve out-of-pocket costs, as it is not routinely stocked in pharmacies. Travelers to high-risk regions are advised to consult healthcare providers at least 6–8 weeks before departure to assess their need for vaccination. It’s crucial to note that BCG is not recommended for individuals with compromised immune systems, pregnant women, or those with severe skin conditions, as these factors increase the risk of adverse reactions. For parents in endemic regions, ensuring timely vaccination of newborns is essential, as delays can reduce the vaccine’s protective effects.
Comparatively, the BCG vaccine’s accessibility contrasts sharply with that of vaccines for diseases like measles or polio, which benefit from global eradication campaigns and robust funding. TB’s persistent prevalence, coupled with the vaccine’s limitations, has relegated it to a lower priority in global health initiatives. However, ongoing research into new TB vaccines, such as M72/AS01E, offers hope for improved protection and broader accessibility in the future. Until then, maximizing the BCG vaccine’s reach within existing frameworks remains critical. This includes strengthening healthcare systems in high-burden countries, addressing supply chain inefficiencies, and raising awareness about the vaccine’s role in TB prevention.
In conclusion, the BCG vaccine’s availability is a reflection of global health inequities and strategic priorities. While it remains a cornerstone of TB prevention in many regions, its accessibility is far from universal. Practical steps, such as improving distribution networks and educating at-risk populations, can enhance its impact. For individuals and policymakers alike, understanding the vaccine’s limitations and potential is key to navigating its role in the fight against TB. As the world awaits next-generation vaccines, the BCG vaccine continues to serve as a vital, if imperfect, tool in this ongoing battle.
Did I Have the Hepatitis A Vaccine? How to Check
You may want to see also
Explore related products






![]()
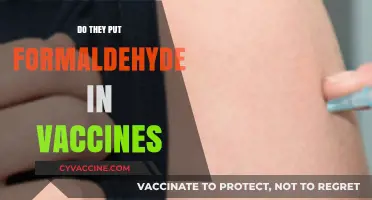
High-Risk Groups: Who still receives TB vaccination in targeted populations
The Bacille Calmette-Guérin (BCG) vaccine, developed in the 1920s, remains the only available vaccine for tuberculosis (TB). Despite its age, it is not universally administered due to variable efficacy and shifting global health priorities. However, targeted populations at high risk of TB exposure or severe outcomes still receive the BCG vaccine as part of strategic public health efforts. These groups are identified based on geographic location, occupational hazards, and specific health conditions that increase susceptibility to TB infection.
Identifying High-Risk Groups:
In countries with high TB incidence, such as India, South Africa, and parts of Southeast Asia, infants are routinely vaccinated at birth. This practice aims to protect them during early childhood, when the risk of severe TB, including meningitis and disseminated disease, is highest. For example, the World Health Organization (WHO) recommends BCG vaccination for all newborns in regions with a TB incidence rate exceeding 40 per 100,000 population. In contrast, countries with low TB prevalence, like the United States, reserve BCG vaccination for specific high-risk groups, such as healthcare workers exposed to multidrug-resistant TB (MDR-TB) or individuals with documented exposure to untreated TB cases.
Occupational and Environmental Risks:
Healthcare workers, laboratory personnel, and individuals working in congregate settings (e.g., prisons, homeless shelters) face elevated TB exposure risks. In these cases, BCG vaccination may be offered as part of a comprehensive TB prevention strategy, though it is often supplemented with regular TB screening and preventive therapy. For instance, a healthcare worker in a high-burden setting might receive a single 0.1 mL intradermal dose of BCG, followed by annual tuberculin skin tests to monitor for infection. However, the vaccine’s efficacy in adults is limited, typically ranging from 0% to 80%, so it is not a standalone solution.
Immunocompromised Individuals and Special Considerations:
While BCG is generally contraindicated in people with weakened immune systems due to the risk of disseminated BCG infection, certain immunocompromised groups may still receive the vaccine under strict medical supervision. For example, HIV-positive infants in high-burden settings are vaccinated at birth, as the risk of severe TB outweighs the potential vaccine risks. However, this decision is made on a case-by-case basis, considering factors like viral load, CD4 count, and local TB prevalence. Pregnant women and individuals with severe skin conditions are typically excluded from BCG vaccination due to safety concerns.
Practical Implementation and Challenges:
Administering BCG to targeted populations requires careful planning and resource allocation. The vaccine must be stored between 2°C and 8°C, and its distinctive administration method—intradermal injection using a bifurcated needle—demands trained personnel. Scar formation at the injection site is a hallmark of successful vaccination, but it can also cause confusion in TB screening, as it may lead to false-positive tuberculin skin test results. Public health programs must balance these logistical challenges with the vaccine’s potential to prevent severe TB in vulnerable groups.
In summary, BCG vaccination remains a critical tool for protecting high-risk populations from TB, particularly in regions with high disease burden. By targeting infants, healthcare workers, and select immunocompromised individuals, public health efforts aim to maximize the vaccine’s impact while minimizing risks. As global TB control strategies evolve, the role of BCG vaccination will continue to be refined to address the needs of those most at risk.
Choosing the Right Vaccine: A Comprehensive Guide to Your Best Option
You may want to see also
Explore related products





![]()
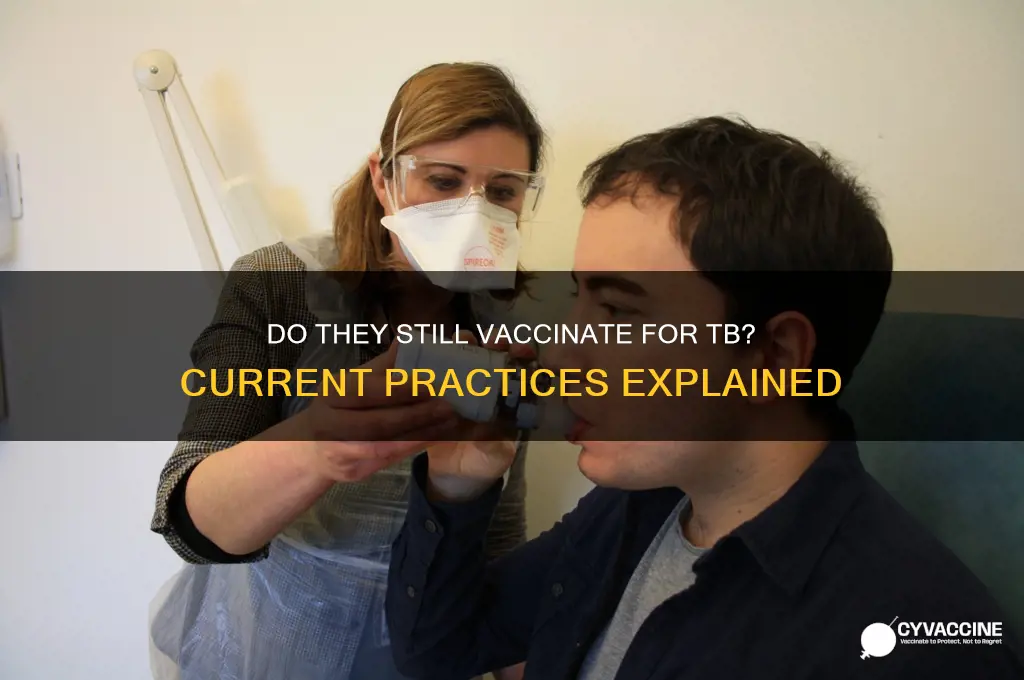
Vaccine Effectiveness: Efficacy of the BCG vaccine in preventing TB infections
The Bacille Calmette-Guérin (BCG) vaccine, developed in the early 20th century, remains the only widely available vaccine for tuberculosis (TB). Its effectiveness, however, is a subject of ongoing debate and varies significantly depending on geographic location, age, and the specific strain of *Mycobacterium tuberculosis* circulating in a population. In countries with high TB prevalence, such as India and parts of Africa, the BCG vaccine is routinely administered to infants within the first few days of life. This early vaccination is critical because the vaccine’s protective efficacy against severe forms of TB, like meningitis in children, can reach up to 80%. However, its effectiveness against pulmonary TB in adults is far less consistent, typically ranging from 0% to 80% in different studies. This variability underscores the need for a nuanced understanding of the BCG vaccine’s role in TB prevention.
One of the key challenges in assessing BCG’s efficacy is its waning immunity over time. Studies show that the vaccine’s protective effects diminish after 10–15 years, leaving adolescents and adults vulnerable to TB infection. This has led to the exploration of booster doses or alternative vaccination strategies, such as revaccination in high-risk populations. For instance, in some countries, healthcare workers or individuals with known TB exposure may receive a second BCG dose, though evidence supporting this practice remains limited. Additionally, the vaccine’s effectiveness can be influenced by prior exposure to environmental mycobacteria, which may interfere with the immune response to BCG. This phenomenon, known as “masking,” further complicates efforts to standardize its use globally.
Despite these limitations, the BCG vaccine remains a cornerstone of TB prevention in many parts of the world. Its ability to reduce childhood mortality from TB is well-documented, making it a vital tool in regions with high disease burden. However, its inconsistent protection against pulmonary TB—the most common and contagious form of the disease—highlights the urgent need for a more effective vaccine. Researchers are currently investigating novel candidates, such as the M72/AS01E vaccine, which has shown promising results in phase IIb trials, with 50% efficacy in preventing TB in adults with latent infection. Until such alternatives become available, optimizing BCG’s use through targeted administration and improved delivery methods remains a priority.
Practical considerations for BCG vaccination include ensuring proper administration via intradermal injection, typically using a dose of 0.05–0.1 mL of the vaccine. The characteristic BCG scar that forms at the injection site is a sign of successful immunization, though its absence does not necessarily indicate vaccine failure. Adverse effects are generally mild, such as local pain or swelling, but severe reactions like abscess formation or disseminated BCG infection are rare, occurring primarily in immunocompromised individuals. For this reason, BCG is contraindicated in individuals with HIV or other conditions affecting the immune system. Understanding these specifics is crucial for healthcare providers to maximize the vaccine’s benefits while minimizing risks.
In conclusion, while the BCG vaccine is not a perfect solution for TB prevention, its role in reducing severe disease in children and its potential as a stopgap measure in high-burden settings cannot be overlooked. Efforts to improve its efficacy, such as through booster doses or combination with new vaccines, are essential to address its limitations. As the global health community continues to combat TB, the BCG vaccine remains a critical tool—one that, when used strategically, can save lives and pave the way for more advanced interventions in the future.
Massachusetts Vaccine Booking Guide: Steps to Secure Your Appointment
You may want to see also
Explore related products



![]()
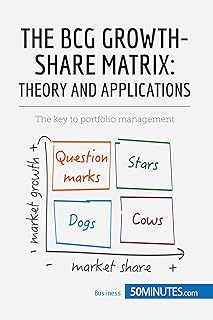
Alternative Treatments: Emerging TB prevention methods beyond traditional vaccination
The Bacille Calmette-Guerin (BCG) vaccine, the traditional TB vaccine, offers limited protection against pulmonary TB in adults, the most common form of transmission. This reality fuels the search for alternative prevention methods, particularly for high-risk populations.
One promising avenue is host-directed therapies (HDTs), which aim to boost the body's innate immune response to TB. These therapies target specific cellular pathways involved in fighting Mycobacterium tuberculosis, the bacterium causing TB. For instance, research suggests that vitamin D supplementation, particularly in deficient individuals, may enhance macrophage function, the immune cells that engulf and destroy invading pathogens. Studies indicate a potential 50% reduction in TB risk with adequate vitamin D levels, though optimal dosage and duration require further investigation.
Dosing recommendations vary, but generally, adults may benefit from 1000-2000 IU of vitamin D3 daily, with higher doses potentially needed for those with severe deficiencies.
Another emerging strategy involves trained immunity, a form of long-term immune memory in innate immune cells. Certain vaccines, like the BCG itself or the measles vaccine, have been shown to induce trained immunity, potentially offering broader protection against various infections, including TB. This approach leverages the body's existing immune system, potentially providing a more sustainable and cost-effective solution compared to traditional vaccines.
While still in its early stages, trained immunity research holds immense promise for TB prevention, particularly in resource-limited settings.
Beyond pharmacological interventions, lifestyle modifications play a crucial role in TB prevention. Adequate nutrition, particularly a diet rich in fruits, vegetables, and whole grains, strengthens the immune system. Regular exercise promotes overall health and may enhance immune function. Additionally, reducing exposure to air pollution and improving ventilation in crowded living conditions can significantly lower the risk of TB transmission.
These alternative approaches, while not replacements for traditional vaccination, offer a multifaceted strategy for TB prevention. By combining host-directed therapies, leveraging trained immunity, and promoting healthy lifestyles, we can move towards a future where TB is no longer a global health threat.
Post-Shingrix Vaccine Diet: Best Foods for Recovery and Comfort
You may want to see also
![]()
Country-Specific Policies: Variations in TB vaccination practices worldwide
The Bacille Calmette-Guerin (BCG) vaccine, developed in the early 20th century, remains the only widely available tool for preventing tuberculosis (TB). However, its use varies dramatically across countries, influenced by factors like TB incidence rates, healthcare infrastructure, and cost-effectiveness analyses. This patchwork of policies creates a global landscape where a child born in one nation might receive the vaccine at birth, while another in a neighboring country never encounters it.
Understanding these variations is crucial for travelers, healthcare professionals, and anyone interested in global health disparities.
Consider the contrasting approaches of the United States and India. In the U.S., where TB cases are relatively rare, the BCG vaccine is not routinely administered. The Centers for Disease Control and Prevention (CDC) recommends it only for specific high-risk groups, such as healthcare workers exposed to multidrug-resistant TB or infants traveling to countries with high TB prevalence. This targeted approach reflects the low disease burden and the vaccine's limited efficacy against pulmonary TB, the most contagious form. Conversely, India, a country with a high TB burden, implements universal BCG vaccination at birth. This strategy aims to provide a baseline level of protection to the entire population, despite the vaccine's limitations.
The Indian government's Revised National Tuberculosis Control Program (RNTCP) emphasizes early vaccination as a cornerstone of its TB control efforts, often administering the vaccine within 24 hours of birth.
The BCG vaccine's dosage and administration methods also exhibit regional differences. While the standard dose is 0.05 mL for newborns, some countries, like Brazil, use a 0.1 mL dose for older children and adults. This variation highlights the need for careful consideration of age-specific immune responses and potential side effects. Additionally, the vaccine's route of administration varies. The traditional intradermal injection, where the vaccine is delivered just beneath the skin's surface, is the most common method. However, some countries, like Japan, have experimented with scarification, a technique involving multiple pricks on the skin's surface, to improve immune response.
These country-specific policies are not without controversy. Critics argue that universal BCG vaccination in low-incidence countries may lead to false positive results in TB skin tests, complicating diagnosis. Conversely, in high-burden settings, the vaccine's moderate efficacy against pulmonary TB raises questions about its overall impact on disease transmission. Despite these debates, the BCG vaccine remains a vital tool in the global fight against TB, with its use continually evolving based on local epidemiological data and public health priorities.
Catching Up: Steps to Get Your Child’s Vaccinations Back on Track
You may want to see also
Frequently asked questions
The Bacille Calmette-Guérin (BCG) vaccine for TB is not routinely given in the United States. It is only recommended for specific high-risk groups, such as healthcare workers exposed to multidrug-resistant TB or infants living in households with active TB cases.
Yes, the BCG vaccine is still widely used in many countries, particularly those with high TB prevalence. It is often given at birth or during childhood as part of national immunization programs to reduce the risk of severe TB in infants and young children.
The BCG vaccine is not universally administered because its effectiveness varies, and it primarily protects against severe forms of TB in children, not adult pulmonary TB. In low-incidence countries like the U.S., other strategies, such as testing and treatment, are prioritized to control TB.















![Latest Updates: Is a Vaccine Available for [Disease/Condition] Yet?](/images/resources/do-they-have-a-vaccine-yet_20251212033410.webp)