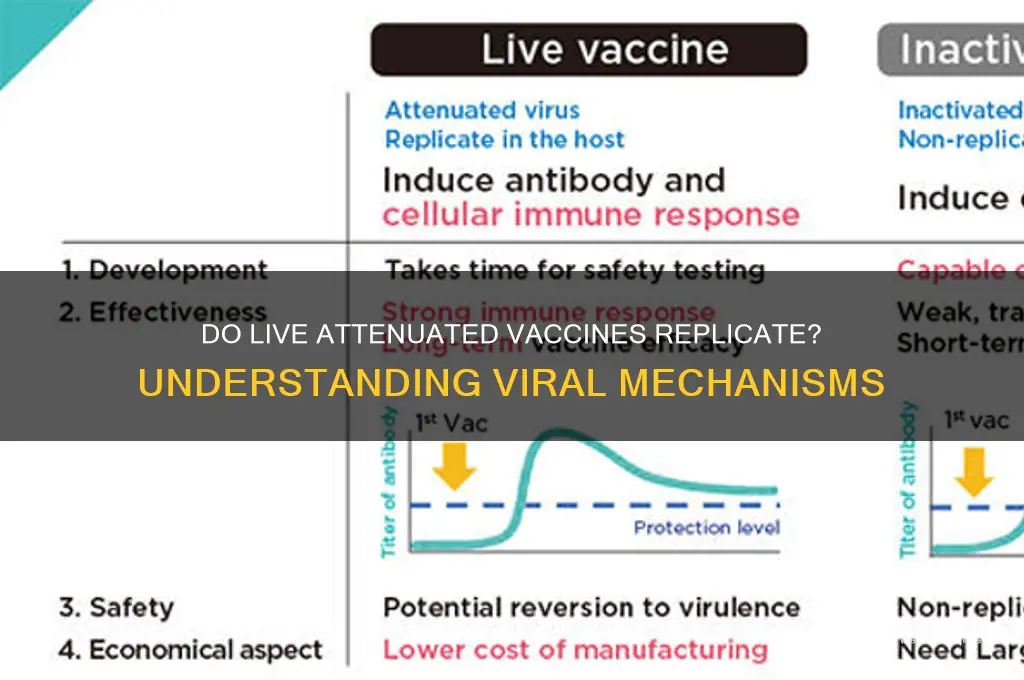
Live attenuated vaccines contain weakened versions of viruses that are still capable of replicating within the body, albeit at a reduced rate compared to their wild-type counterparts. This limited replication is crucial for triggering a robust immune response, as it allows the immune system to recognize and respond to the virus without causing severe disease. The attenuation process ensures that the virus is safe for use in vaccines while retaining its ability to stimulate both humoral and cell-mediated immunity, providing long-lasting protection against the targeted pathogen. Understanding how these viruses replicate in the body is essential for optimizing vaccine efficacy and safety.
| Characteristics | Values |
|---|---|
| Replication Capability | Live attenuated vaccine viruses replicate at a reduced rate in the host. |
| Attenuation Mechanism | Viruses are weakened through serial passage in cell cultures or animals. |
| Immune Response | Stimulates strong humoral and cell-mediated immune responses. |
| Duration of Immunity | Typically provides long-lasting immunity, often lifelong. |
| Shedding Potential | Can be shed in bodily fluids (e.g., nasal secretions, stool) post-vaccination. |
| Contraindications | Not recommended for immunocompromised individuals due to replication risk. |
| Storage Requirements | Often requires refrigeration to maintain virus viability. |
| Examples | Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Yellow Fever vaccines. |
| Reversion to Virulence Risk | Extremely low but theoretically possible under specific conditions. |
| Administration Route | Commonly administered via oral, nasal, or subcutaneous routes. |
| Efficacy | Highly effective due to mimicking natural infection. |
| Safety Profile | Generally safe but may cause mild, vaccine-related symptoms. |
Explore related products






What You'll Learn
- Replication Mechanism: How attenuated viruses replicate at lower levels in the body
- Immune Response: Stimulation of strong, lasting immunity via controlled viral replication
- Safety Measures: Attenuation ensures limited replication, preventing disease while triggering immunity
- Shedding Risks: Potential for vaccine virus shedding and transmission to others
- Cold Chain Dependency: Replication stability and vaccine efficacy reliance on proper storage
![]()
Replication Mechanism: How attenuated viruses replicate at lower levels in the body
Live attenuated vaccines harness a delicate balance: weakened viruses that retain their ability to replicate, but at significantly reduced levels compared to their wild counterparts. This controlled replication is the cornerstone of their effectiveness, stimulating a robust immune response without causing severe disease. The attenuation process, often achieved through serial passage in cell cultures or targeted genetic modifications, introduces mutations that impair the virus's ability to replicate efficiently in the human body.
These mutations can affect various stages of the viral life cycle, from entry into host cells to viral protein synthesis and assembly. For instance, the measles vaccine virus, Schwarz strain, carries mutations in its fusion protein, hindering its ability to fuse with host cell membranes and limiting its spread. Similarly, the yellow fever vaccine, YF-17D, has mutations in its non-structural proteins, reducing its replicative capacity in human cells compared to mosquitoes, its natural host.
The attenuated virus's replication is further constrained by the host's immune system. As the virus replicates at low levels, it triggers the innate immune response, leading to the production of interferons and other antiviral molecules that suppress viral replication. This initial response buys time for the adaptive immune system to mount a targeted attack, producing antibodies and cytotoxic T cells that eliminate infected cells and prevent further viral spread. This two-pronged immune response not only controls the attenuated virus but also establishes long-lasting immunity against the wild-type virus.
Understanding the replication mechanism of attenuated viruses is crucial for vaccine development and safety. By carefully calibrating the level of attenuation, scientists can ensure that the vaccine virus replicates sufficiently to induce a strong immune response, but not so much as to cause harm. This balance is particularly important for vulnerable populations, such as infants and immunocompromised individuals, who may be more susceptible to adverse effects from even low levels of viral replication. For example, the rotavirus vaccine, RotaTeq, is administered orally to infants in a three-dose series (at 2, 4, and 6 months of age) to ensure optimal immune response while minimizing the risk of adverse events.
In practice, the replication of attenuated viruses can be influenced by various factors, including the route of administration, dosage, and host immune status. Intranasal vaccines, such as the live attenuated influenza vaccine (LAIV), replicate primarily in the nasal mucosa, eliciting a localized immune response that can prevent infection at the site of entry. In contrast, oral vaccines, like the Sabin polio vaccine, must survive the acidic environment of the stomach and replicate in the intestinal tract to induce a systemic immune response. To maximize the effectiveness of live attenuated vaccines, it is essential to follow recommended dosage schedules and storage conditions. For instance, LAIV should be stored at 2-8°C and administered only to healthy individuals aged 2-49 years, as per CDC guidelines. By understanding and controlling the replication mechanism of attenuated viruses, we can harness their potential to provide safe, effective, and long-lasting immunity against infectious diseases.
Vaccine Side Effects: Taste and Smell Loss?
You may want to see also
Explore related products






![]()
Immune Response: Stimulation of strong, lasting immunity via controlled viral replication
Live attenuated vaccines harness the power of controlled viral replication to stimulate a robust and enduring immune response. Unlike inactivated or subunit vaccines, these vaccines contain weakened but still viable pathogens that mimic natural infection without causing disease. This replication, though limited, triggers a multifaceted immune reaction, activating both innate and adaptive arms of the immune system. For instance, the measles, mumps, and rubella (MMR) vaccine uses attenuated viruses that replicate locally in the body, prompting the production of neutralizing antibodies, cytotoxic T cells, and memory cells. This orchestrated response not only clears the attenuated virus but also establishes long-term immunity, often lasting a lifetime with just one or two doses.
To understand the mechanism, consider the dosage and administration of live attenuated vaccines. The varicella vaccine, for example, delivers a precise dose of weakened varicella-zoster virus, typically administered subcutaneously to children aged 12–15 months, with a booster at 4–6 years. This controlled replication in the lymphatic system primes the immune system to recognize and combat the virus effectively. Practical tips for parents include ensuring the child is healthy at the time of vaccination, as mild fever or rash may occur post-vaccination, signaling a normal immune response rather than disease.
Comparatively, live attenuated vaccines offer distinct advantages over other vaccine types. While mRNA vaccines like Pfizer-BioNTech’s COVID-19 vaccine rely on genetic material to induce spike protein production, live attenuated vaccines expose the immune system to the entire virus, albeit in a weakened form. This exposure fosters a more comprehensive immune memory, including mucosal immunity, which is particularly critical for respiratory and gastrointestinal pathogens. For example, the oral polio vaccine (OPV) replicates in the gut, providing both systemic and local immunity, reducing viral shedding and transmission in communities.
However, the controlled replication of live attenuated vaccines requires careful consideration of safety and contraindications. Immunocompromised individuals, such as those with HIV or undergoing chemotherapy, may face risks if the attenuated virus replicates unchecked. Pregnant women are also advised to avoid live vaccines due to theoretical risks to the fetus. Healthcare providers must assess patient history and immune status before administering these vaccines, balancing the benefits of strong immunity against potential risks.
In conclusion, the stimulation of strong, lasting immunity via controlled viral replication is a hallmark of live attenuated vaccines. By leveraging the body’s natural immune response, these vaccines provide unparalleled protection against infectious diseases. Practical implementation involves precise dosing, age-appropriate administration, and awareness of contraindications. As a standalone strategy, live attenuated vaccines remain a cornerstone of preventive medicine, offering durable immunity with minimal doses and maximal impact.
Wealth and Vaccine Hesitancy: Unraveling the Surprising Connection
You may want to see also
Explore related products






![]()
Safety Measures: Attenuation ensures limited replication, preventing disease while triggering immunity
Live attenuated vaccines represent a cornerstone of modern immunology, leveraging weakened viruses to stimulate robust immune responses without causing disease. The key to their safety lies in attenuation—a process that reduces the virus’s virulence while preserving its ability to replicate minimally. This controlled replication is critical: it allows the immune system to recognize and respond to the pathogen, generating memory cells for future protection. For instance, the measles vaccine contains an attenuated virus that replicates just enough to trigger immunity but not enough to overwhelm the body’s defenses. This balance ensures that the vaccine is both effective and safe, even for vulnerable populations like infants, who typically receive their first dose at 12 months of age.
Attenuation is achieved through meticulous laboratory techniques, such as serial passage in cell cultures or targeted genetic modifications. These methods introduce mutations that impair the virus’s ability to cause harm while maintaining its immunogenicity. For example, the oral polio vaccine (OPV) uses an attenuated poliovirus that replicates in the gut, inducing mucosal immunity without spreading to the central nervous system. However, safety measures extend beyond attenuation itself. Dosage is carefully calibrated to ensure limited replication; too much could risk adverse effects, while too little might fail to elicit a sufficient immune response. This precision is why live attenuated vaccines often require fewer doses compared to inactivated vaccines, such as the single-dose yellow fever vaccine for travelers to endemic regions.
Despite their safety, live attenuated vaccines are not without precautions. They are generally contraindicated in immunocompromised individuals, as even limited replication could pose risks. For instance, the varicella vaccine for chickenpox is avoided in HIV-positive patients with low CD4 counts. Additionally, these vaccines must be stored and handled properly—typically at 2°C to 8°C—to maintain viral viability without reversion to virulence. Practical tips for healthcare providers include verifying patient immunity status before administration and counseling on potential mild side effects, such as a low-grade fever or rash at the injection site, which are normal signs of immune activation.
Comparatively, live attenuated vaccines offer advantages over other vaccine types, such as mRNA or subunit vaccines, by mimicking natural infection more closely. This results in durable immunity, often lasting decades, as seen with the MMR (measles, mumps, rubella) vaccine. However, their live nature necessitates stricter safety protocols. For example, the rotavirus vaccine is administered orally in a multi-dose regimen, with timing critical to avoid interference from maternal antibodies in infants. This highlights the importance of adhering to age-specific guidelines: rotavirus vaccination begins at 6 weeks of age, with the final dose given no later than 8 months.
In conclusion, attenuation is a sophisticated safety measure that ensures live vaccines replicate just enough to provoke immunity without causing disease. This delicate balance is achieved through precise laboratory techniques, careful dosage calibration, and stringent handling protocols. While precautions are necessary, particularly for at-risk groups, the benefits of live attenuated vaccines—such as long-lasting immunity and fewer required doses—make them indispensable tools in public health. By understanding and implementing these safety measures, healthcare providers can maximize the efficacy of these vaccines while minimizing risks, ensuring protection for individuals and communities alike.
Iceland Entry: Vaccination Requirements and Rules
You may want to see also
Explore related products






![]()
Shedding Risks: Potential for vaccine virus shedding and transmission to others
Live attenuated vaccines, such as those for measles, mumps, rubella (MMR), and varicella (chickenpox), contain weakened viruses that can replicate in the vaccinated individual. While this replication is typically limited and controlled, it raises the question of vaccine virus shedding—whether these viruses can be transmitted to others. Shedding occurs when the vaccine virus is excreted from the body, often through respiratory secretions, stool, or skin lesions, and can potentially expose unvaccinated or immunocompromised individuals. Understanding this risk is crucial for informed decision-making and public health strategies.
Consider the varicella vaccine, which is known to cause mild rash and, in rare cases, vaccine-strain virus shedding. Studies show that approximately 10-30% of vaccinated children shed the vaccine virus, primarily through respiratory secretions or skin lesions. While transmission to close contacts is rare, it has been documented, particularly in household settings. For instance, a 2014 study reported vaccine-strain varicella transmission from a vaccinated child to an immunocompromised adult, highlighting the importance of monitoring shedding risks in vulnerable populations. This underscores the need for precautions, such as avoiding contact with high-risk individuals during the 4-6 weeks post-vaccination when shedding is most likely.
From a practical standpoint, minimizing shedding risks involves timing and isolation strategies. For live attenuated vaccines like MMR or varicella, recipients should avoid close contact with severely immunocompromised individuals for 3-4 weeks post-vaccination. Healthcare workers or caregivers who receive these vaccines should adhere to strict hygiene practices, including handwashing and mask-wearing, to reduce the likelihood of transmission. Additionally, individuals with skin lesions post-varicella vaccination should keep the area covered until fully healed to prevent shedding via direct contact.
Comparatively, the shedding risk of live attenuated vaccines is significantly lower than that of natural infection. For example, wild-type varicella-zoster virus (VZV) shedding is more prolonged and occurs in higher viral loads, increasing transmission risk. The attenuated vaccine virus, while capable of limited replication, is less likely to cause severe disease or widespread transmission. This distinction is critical in weighing the benefits of vaccination against the minimal shedding risks, especially in community settings where herd immunity protects vulnerable populations.
In conclusion, while vaccine virus shedding is a real but rare phenomenon, its implications are manageable with proper precautions. Healthcare providers should educate patients about potential shedding risks, particularly for live attenuated vaccines, and advise on preventive measures. For immunocompromised individuals, alternative vaccination strategies or temporary isolation of recently vaccinated contacts may be necessary. By balancing awareness with practical steps, we can maximize the benefits of live attenuated vaccines while minimizing transmission risks.
Unprotected: The Hepatitis Strain Still Lacking a Vaccine Today
You may want to see also
Explore related products






![]()
Cold Chain Dependency: Replication stability and vaccine efficacy reliance on proper storage
Live attenuated vaccines (LAVs) rely on weakened viruses to stimulate immunity without causing disease. Their efficacy hinges on viral replication within the host, a process that demands precise conditions—both in the body and during storage. This is where the cold chain becomes critical. A single break in temperature control can render these vaccines ineffective, as the attenuated viruses are highly sensitive to heat and freezing. For instance, the measles-mumps-rubella (MMR) vaccine, a LAV, must be stored between 2°C and 8°C (36°F and 46°F). Exposure to temperatures outside this range, even briefly, can degrade the virus’s ability to replicate, reducing immunogenicity. A 2017 study found that MMR vaccine potency dropped by 50% after just 8 hours at 25°C (77°F), underscoring the fragility of these formulations.
Consider the logistical challenges of maintaining such strict storage conditions, especially in resource-limited settings. Vaccines like the oral polio vaccine (OPV) require constant refrigeration until administration, yet they are often distributed in regions with unreliable electricity or extreme climates. A lapse in cold chain integrity at any point—during transport, storage, or handling—can compromise the vaccine’s viability. For example, OPV’s efficacy drops significantly if exposed to temperatures above 8°C for more than 48 hours. This is not merely a theoretical concern; a 2019 WHO report linked vaccine failures in parts of Africa and Asia to cold chain breaches, highlighting the real-world consequences of improper storage.
The implications extend beyond individual protection to herd immunity. LAVs like the yellow fever vaccine, which requires storage at 2°C to 8°C, are critical in outbreak control. A 2020 study in Brazil demonstrated that even minor temperature deviations during distribution reduced the vaccine’s replication stability, leading to suboptimal immune responses in 30% of recipients. This not only jeopardizes personal immunity but also weakens community-level protection, allowing diseases to persist or re-emerge. To mitigate this, healthcare providers must adhere to WHO’s “Five Rights” of vaccine management: right vaccine, right dose, right patient, right route, and right temperature. Digital temperature loggers and solar-powered refrigerators are increasingly used to monitor and maintain cold chain integrity, particularly in remote areas.
Practical steps for ensuring cold chain compliance include regular equipment calibration, staff training on handling protocols, and contingency plans for power outages. For instance, vaccine carriers with ice packs can maintain temperatures for up to 48 hours during transport, while data loggers provide real-time alerts for temperature deviations. Parents and caregivers can also play a role by inquiring about vaccine storage practices at clinics and avoiding exposure of vials to direct sunlight or heat. Ultimately, the efficacy of LAVs is a delicate balance between biological design and logistical precision. Without a robust cold chain, even the most advanced vaccines risk becoming inert, underscoring the inseparable link between storage and immunity.
Optimal Equine Influenza Vaccination Schedule for Horses: Expert Recommendations
You may want to see also
Frequently asked questions
Yes, live attenuated vaccines contain weakened viruses that are designed to replicate in the body, but at a much lower rate and with reduced virulence compared to wild-type viruses.
While rare, the attenuated viruses in these vaccines can sometimes cause mild symptoms similar to the disease they prevent, but they are generally not severe and do not lead to full-blown illness in healthy individuals.
The risk of reversion to a virulent form is extremely low. Live attenuated vaccines are carefully developed and tested to ensure the viruses remain stable and do not regain their disease-causing ability.