Polio, once a widespread and devastating disease, has been largely eradicated globally thanks to widespread vaccination efforts. However, the question of whether children still receive the polio vaccine remains relevant, as the virus persists in a few countries and poses a risk of resurgence if immunization rates decline. In most parts of the world, including the United States and Europe, the polio vaccine is still administered as part of routine childhood immunizations, typically through the inactivated polio vaccine (IPV). This ensures continued protection and prevents the reintroduction of the virus. In polio-endemic countries, such as Afghanistan and Pakistan, both IPV and the oral polio vaccine (OPV) are used to combat the disease. While significant progress has been made, maintaining high vaccination coverage is crucial to achieving complete eradication and ensuring that future generations remain polio-free.
| Characteristics | Values |
|---|---|
| Current Polio Vaccine Status | Yes, children still receive polio vaccines in many countries. |
| Vaccine Types | Inactivated Polio Vaccine (IPV) is the primary vaccine used globally. |
| Global Vaccination Coverage | Approximately 86% of infants received 3 doses of polio vaccine (2022). |
| Eradication Efforts | Polio is nearly eradicated, with only 2 countries (Afghanistan, Pakistan) reporting cases in 2023. |
| Routine Immunization | Included in routine childhood immunization schedules in most countries. |
| Booster Doses | Booster doses are recommended in some regions to maintain immunity. |
| Side Effects | Generally safe; mild side effects include soreness at the injection site, fever, or irritability. |
| Global Initiatives | Supported by the Global Polio Eradication Initiative (GPEI). |
| Age of Vaccination | Typically administered at 2, 4, and 6-18 months, followed by boosters. |
| Country-Specific Policies | Varies; some countries have additional doses or travel requirements. |
Explore related products



$20.46 $21.95



What You'll Learn
- Current Polio Vaccination Schedules: Global recommendations and country-specific polio vaccine administration timelines for children
- Vaccine Types: Differences between inactivated (IPV) and oral (OPV) polio vaccines used today
- Herd Immunity Impact: How widespread vaccination protects unvaccinated children from polio outbreaks
- Polio Eradication Efforts: Progress and challenges in eliminating polio globally since the 1980s
- Vaccine Hesitancy Concerns: Addressing misconceptions and resistance to polio vaccination in some communities
![]()
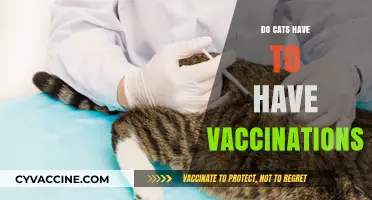
Current Polio Vaccination Schedules: Global recommendations and country-specific polio vaccine administration timelines for children
Polio vaccination remains a cornerstone of global health efforts, but the schedules and strategies vary widely across countries. The World Health Organization (WHO) recommends a primary series of at least three doses of the polio vaccine, typically administered during infancy. This foundation is critical for building immunity against the poliovirus, which can cause irreversible paralysis. In most countries, the first dose is given at 6 weeks of age, followed by two more doses at 4-week intervals. This initial series is often part of a combined vaccine, such as the pentavalent vaccine, which protects against multiple diseases simultaneously. Booster doses are then administered between 12 and 23 months to ensure long-term immunity, aligning with global eradication goals.
Country-specific schedules reflect local disease prevalence, healthcare infrastructure, and public health priorities. For instance, in high-risk regions like Afghanistan and Pakistan, where wild poliovirus transmission persists, children receive additional doses through supplementary immunization activities (SIAs). These campaigns often involve oral polio vaccine (OPV) and aim to reach every child under 5 years old, regardless of prior vaccination history. In contrast, countries declared polio-free, such as the United States and most of Europe, rely on the inactivated polio vaccine (IPV) and administer it as part of routine immunizations. Here, the schedule typically includes a dose at 2 months, 4 months, 6–18 months, and a booster at 4–6 years, ensuring sustained protection without overburdening the healthcare system.
The choice between OPV and IPV also influences vaccination timelines. OPV, which uses a weakened live virus, is cheaper and easier to administer, making it ideal for mass campaigns in low-resource settings. However, it carries a rare risk of vaccine-derived poliovirus (VDPV), prompting some countries to transition to IPV. IPV, while safer, requires injection and is more expensive, limiting its use in regions with limited healthcare access. This dichotomy highlights the balance between cost-effectiveness and safety in global polio eradication strategies.
Practical considerations for parents and caregivers include adhering to local vaccination schedules and keeping immunization records up to date. In countries with fragmented healthcare systems, mobile clinics and community health workers play a vital role in ensuring children receive all required doses. Additionally, travelers from polio-endemic areas may need proof of vaccination to enter certain countries, emphasizing the global interconnectedness of polio prevention efforts. Understanding these nuances empowers families to protect their children effectively while contributing to the broader goal of polio eradication.
Despite progress, challenges remain in achieving universal polio vaccination. Vaccine hesitancy, logistical hurdles, and political instability in some regions threaten to undo decades of work. However, the success of countries like India, which eradicated polio in 2014 through rigorous vaccination campaigns, demonstrates the power of sustained effort. By following WHO guidelines and adapting them to local contexts, countries can ensure that children continue to receive polio vaccines, moving the world closer to a polio-free future.
AstraZeneca and J&J Vaccines: Similarities and Differences
You may want to see also
Explore related products






![]()
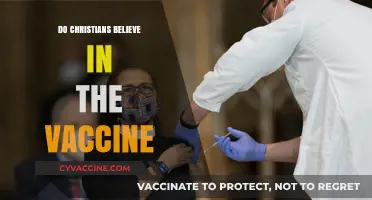
Vaccine Types: Differences between inactivated (IPV) and oral (OPV) polio vaccines used today
Polio vaccination remains a cornerstone of global health efforts, but the choice between inactivated polio vaccine (IPV) and oral polio vaccine (OPV) varies by region and health strategy. Both vaccines target the poliovirus, yet their mechanisms, administration, and outcomes differ significantly. Understanding these differences is crucial for parents, healthcare providers, and policymakers navigating polio prevention in children.
Mechanism and Composition:
IPV is an injectable vaccine containing inactivated (killed) poliovirus strains (types 1, 2, and 3). It triggers the body to produce antibodies in the bloodstream, offering protection against paralytic polio. OPV, on the other hand, is an oral vaccine containing live, attenuated (weakened) poliovirus strains. It mimics natural infection, inducing immunity in the gut (intestinal mucosa) and bloodstream. This gut immunity prevents viral shedding and transmission, a key advantage of OPV in controlling outbreaks.
Administration and Dosage:
IPV is administered intramuscularly or subcutaneously, typically as part of routine immunization schedules. In the U.S., children receive 4 doses: at 2 months, 4 months, 6–18 months, and 4–6 years. OPV is delivered orally, often in drops or syrup, making it easier to administer, especially in mass vaccination campaigns. The WHO recommends 3–4 doses in infancy, with additional campaigns in endemic regions. However, OPV’s live virus can, in rare cases, revert to a virulent form, causing vaccine-associated paralytic polio (VAPP), a risk absent with IPV.
Immunity and Herd Protection:
OPV’s ability to induce mucosal immunity makes it superior in interrupting poliovirus transmission, a critical factor in eradication efforts. However, IPV provides robust individual protection against paralysis but does not prevent viral shedding. This distinction explains why many high-income countries use IPV exclusively, while low-income regions with active transmission rely on OPV. The Global Polio Eradication Initiative often employs a combination strategy, using OPV for outbreak control and IPV for routine immunization.
Practical Considerations:
For parents, the choice between IPV and OPV often depends on geographic location and public health recommendations. In polio-free countries, IPV is the standard, ensuring safety without compromising individual protection. In endemic areas, OPV remains the tool of choice for its logistical simplicity and herd immunity benefits. Travelers to polio-affected regions may require additional OPV doses, even if previously vaccinated with IPV. Always consult healthcare providers for age-appropriate dosing and schedules, as these can vary by country and risk profile.
Global Trends and Future Directions:
As wild poliovirus nears eradication, the focus shifts to minimizing vaccine-derived polio cases. The phased removal of type 2 OPV in 2016, replaced by IPV in routine schedules, exemplifies this transition. However, OPV’s role in outbreak response remains indispensable. Innovations like novel OPV2, designed to reduce reversion risks, highlight ongoing efforts to balance safety and efficacy. For children today, the polio vaccine they receive reflects a global strategy tailored to local needs, ensuring protection while advancing eradication goals.
Should You Vaccinate Your Cat Against FIV? Pros and Cons
You may want to see also
Explore related products






![]()
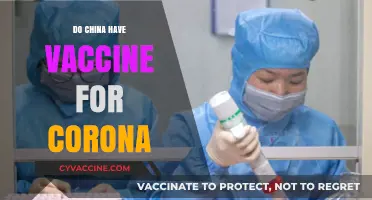
Herd Immunity Impact: How widespread vaccination protects unvaccinated children from polio outbreaks
Polio, once a global menace, has been nearly eradicated thanks to widespread vaccination efforts. However, the question of whether children still receive the polio vaccine remains relevant, especially in regions where the disease persists. The concept of herd immunity plays a critical role in protecting unvaccinated children from polio outbreaks. When a high percentage of the population is immunized, the virus struggles to find susceptible hosts, effectively shielding those who cannot be vaccinated due to medical reasons or age. This collective defense mechanism is a cornerstone of public health, ensuring that even the most vulnerable remain safe.
To understand herd immunity’s impact, consider the polio vaccine’s administration schedule. In most countries, children receive the inactivated poliovirus vaccine (IPV) or oral poliovirus vaccine (OPV) in a series of doses starting at 2 months of age, with boosters at 4 months, 6-18 months, and 4-6 years. This regimen ensures robust individual immunity. However, not all children can follow this schedule due to allergies, immunodeficiencies, or other health conditions. For these children, herd immunity is their only safeguard. When vaccination rates exceed 80-85%, the virus’s transmission chain is disrupted, significantly reducing the likelihood of outbreaks. This threshold is crucial, as it minimizes the risk of exposure for unvaccinated individuals.
A real-world example of herd immunity’s success is India, which was declared polio-free in 2014 after decades of vaccination campaigns. Despite challenges like population density and accessibility, high vaccination rates created a protective barrier, even for those who couldn’t be immunized. Conversely, regions with low vaccination coverage, such as parts of Afghanistan and Pakistan, continue to report polio cases, highlighting the fragility of herd immunity when it’s compromised. These disparities underscore the importance of maintaining global vaccination efforts to protect not just individuals but entire communities.
Practical steps to strengthen herd immunity include ensuring timely vaccination for all eligible children, addressing vaccine hesitancy through education, and improving healthcare access in underserved areas. Parents can contribute by adhering to recommended vaccine schedules and advocating for community-wide immunization. Policymakers must prioritize funding for vaccination programs and surveillance systems to detect and respond to potential outbreaks swiftly. By working together, societies can sustain the progress made against polio and protect future generations from this devastating disease. The lesson is clear: widespread vaccination doesn’t just save lives—it creates a shield that guards everyone, including those who cannot be vaccinated.
Vaccinating Children: Harmful or Helpful?
You may want to see also
Explore related products






![]()
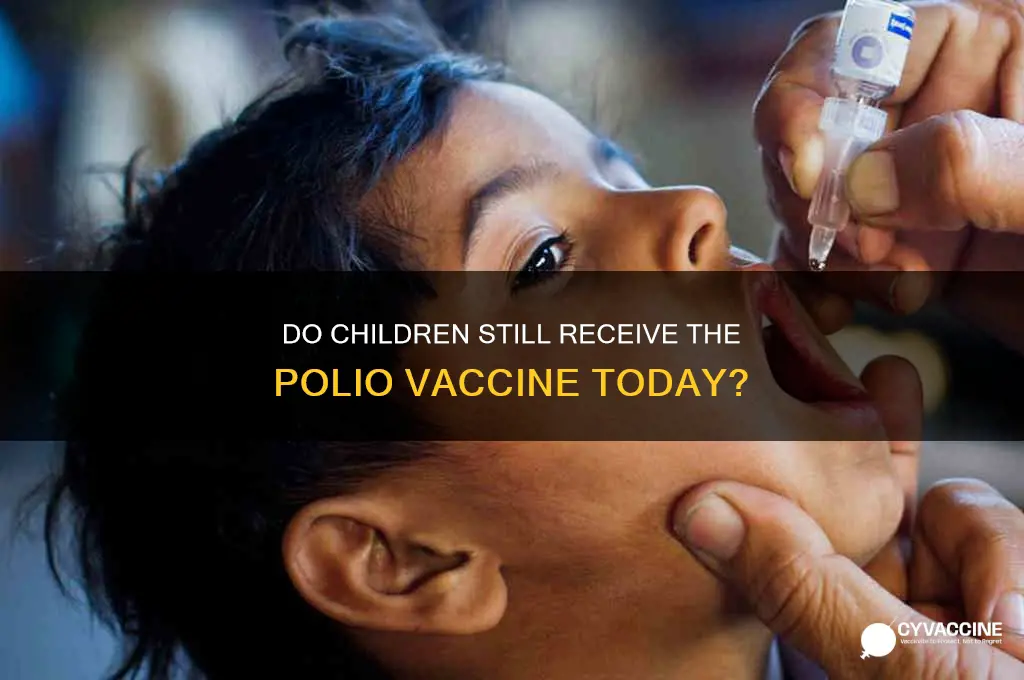
Polio Eradication Efforts: Progress and challenges in eliminating polio globally since the 1980s
Since the 1980s, global polio eradication efforts have achieved remarkable milestones, reducing cases by over 99% and confining the virus to just two countries: Afghanistan and Pakistan. This success is largely due to the widespread administration of the polio vaccine, primarily the oral polio vaccine (OPV) and, in some regions, the inactivated polio vaccine (IPV). Children worldwide still receive the polio vaccine as part of routine immunization schedules, typically starting at 6 weeks of age with a series of doses administered up to 18 months. In high-risk areas, supplementary immunization campaigns ensure additional protection, often delivering OPV drops to children under 5 years old. Despite these advancements, the final push to eradicate polio faces significant challenges, including vaccine hesitancy, political instability, and the emergence of vaccine-derived polioviruses (VDPVs), which occur in under-immunized communities.
One of the most instructive aspects of polio eradication is the strategic use of vaccines tailored to different contexts. OPV, a live-attenuated vaccine, is highly effective in inducing intestinal immunity and halting person-to-person transmission, making it the cornerstone of eradication efforts. However, its rare ability to revert to a virulent form has led to VDPV outbreaks, prompting the introduction of IPV in routine immunization programs. IPV, while safer and effective in preventing paralytic polio, does not confer intestinal immunity, necessitating continued OPV use in outbreak-prone areas. This dual approach highlights the complexity of balancing eradication goals with risk management, particularly in regions with fragile healthcare systems.
Persuasively, the economic and humanitarian case for polio eradication remains compelling. Eradicating polio would save an estimated $40–50 billion globally over the next 20 years, primarily by eliminating the need for ongoing vaccination and treatment of polio-related disabilities. For every $1 invested in eradication, societies reap $27 in health and economic benefits. Yet, securing sustained funding and political commitment remains a challenge, especially as polio cases dwindle and other health priorities emerge. Advocates must emphasize that eradication is not just a health goal but a testament to global solidarity and the power of collective action.
Comparatively, polio eradication efforts offer lessons for tackling other vaccine-preventable diseases. The success of polio campaigns in reaching remote populations through innovative strategies, such as mobile vaccination teams and community engagement, provides a blueprint for improving overall immunization coverage. However, polio’s unique characteristics—its visible symptoms, short infectious period, and lack of animal reservoirs—have made it a more tractable target than diseases like measles or malaria. Translating polio’s successes to other diseases requires adapting strategies to address their distinct epidemiological and social challenges, such as combating misinformation and strengthening healthcare infrastructure.
Descriptively, the human impact of polio eradication is profound. In the 1980s, polio paralyzed over 350,000 children annually, leaving many with lifelong disabilities. Today, fewer than 10 wild poliovirus cases are reported yearly, and entire generations have grown up without witnessing its devastating effects. Yet, the persistence of polio in Afghanistan and Pakistan, coupled with VDPV outbreaks in countries like Nigeria and the Democratic Republic of Congo, underscores the fragility of progress. Each unvaccinated child remains a potential conduit for the virus’s resurgence, making the final mile of eradication the most critical—and the most challenging. Practical steps for parents include ensuring their children complete the full vaccine series, participating in supplementary campaigns, and advocating for community-wide immunization to achieve herd immunity. The end of polio is within reach, but only if global efforts remain unwavering.
Puppy Vaccination Schedule: Shots Needed for Full Immunity
You may want to see also
Explore related products





![]()
Vaccine Hesitancy Concerns: Addressing misconceptions and resistance to polio vaccination in some communities
Polio, once a global scourge, has been nearly eradicated thanks to widespread vaccination efforts. Yet, in some communities, vaccine hesitancy persists, threatening to undo decades of progress. Misconceptions about the polio vaccine’s safety, efficacy, or necessity fuel resistance, particularly in regions where the disease is no longer endemic. Addressing these concerns requires a nuanced understanding of the fears driving hesitancy and tailored strategies to rebuild trust.
One common misconception is the belief that the polio vaccine causes the disease it aims to prevent. This myth often stems from misinformation about the oral polio vaccine (OPV), which contains a weakened live virus. In extremely rare cases (about 1 in 2.7 million doses), the attenuated virus can mutate and cause vaccine-derived poliovirus (VDPV). However, the inactivated polio vaccine (IPV), which is injected and contains no live virus, eliminates this risk entirely. Educating communities about the differences between OPV and IPV, along with their respective benefits and risks, is crucial. For instance, IPV is recommended for children under 18 months in many countries, followed by booster doses at 4 and 6–18 months, depending on local guidelines.
Another barrier to polio vaccination is the perception that the disease is no longer a threat. In regions where polio has been eradicated, parents may question the need for continued vaccination. This complacency overlooks the fact that polio remains endemic in a few countries, and global travel can reintroduce the virus to unvaccinated populations. Historical examples, such as the 2013 outbreak in Syria after a 14-year absence, underscore the importance of maintaining high vaccination rates. Public health campaigns should emphasize the concept of herd immunity and the role each vaccinated child plays in protecting the broader community.
Cultural and religious beliefs also contribute to vaccine resistance in some communities. Rumors that vaccines contain harmful substances or violate religious principles can spread rapidly, particularly in areas with limited access to reliable information. Engaging local leaders, religious figures, and trusted community members to dispel these myths can be highly effective. For example, in Nigeria, involving Islamic scholars in polio eradication efforts helped overcome resistance by affirming the vaccine’s compatibility with religious teachings. Similarly, providing transparent information about vaccine ingredients and manufacturing processes can address specific concerns.
Finally, systemic issues, such as inadequate healthcare infrastructure and inconsistent vaccine availability, exacerbate hesitancy. When parents face logistical challenges in accessing vaccines or experience stockouts, their trust in the system erodes. Strengthening healthcare delivery systems, ensuring consistent vaccine supply, and offering flexible vaccination schedules can mitigate these issues. Mobile clinics, for instance, have proven effective in reaching underserved populations, while reminder systems via SMS or community health workers can improve adherence to vaccination schedules.
In conclusion, addressing vaccine hesitancy in polio vaccination requires a multi-faceted approach that tackles misinformation, cultural barriers, and systemic challenges. By providing accurate, culturally sensitive information and improving access to vaccines, communities can be empowered to protect their children from this preventable disease. The fight against polio is not over—sustained vaccination efforts are essential to ensure a polio-free future for all.
Are US Vaccines Imported from China? Uncovering the Supply Chain
You may want to see also
Frequently asked questions
Yes, children still receive the polio vaccine as part of routine immunization schedules in many countries to prevent the disease and maintain global eradication efforts.
In many countries, the polio vaccine is mandatory for children as part of their standard immunization schedule, though requirements may vary by region.
Children still need the polio vaccine because the virus is not completely eradicated globally, and stopping vaccination could lead to a resurgence of the disease.
Children today typically receive the inactivated poliovirus vaccine (IPV), which is administered through injection, as it is safer and more widely used than the oral polio vaccine (OPV).