Vaccines have played a pivotal role in reducing the incidence of diphtheria, a once-common and often fatal bacterial infection that primarily affects the throat and nose. Before the introduction of the diphtheria vaccine in the 1920s, the disease was a leading cause of childhood mortality worldwide, claiming hundreds of thousands of lives annually. The widespread adoption of vaccination programs has led to a dramatic decline in diphtheria cases, with many countries reporting fewer than a handful of cases per year. For instance, in the United States, cases have dropped from over 200,000 annually in the 1920s to virtually zero in recent decades. This success underscores the effectiveness of vaccines in controlling and nearly eradicating diphtheria, highlighting their critical role in public health. However, the disease remains a threat in regions with low vaccination rates, emphasizing the ongoing need for global immunization efforts.
| Characteristics | Values |
|---|---|
| Disease Prevalence Before Vaccines | Diphtheria was a major cause of childhood illness and death globally. |
| Vaccine Introduction | Diphtheria vaccines (e.g., DTaP, Tdap) introduced in the 1920s-1940s. |
| Global Reduction in Cases | Over 90% reduction in diphtheria cases worldwide post-vaccination. |
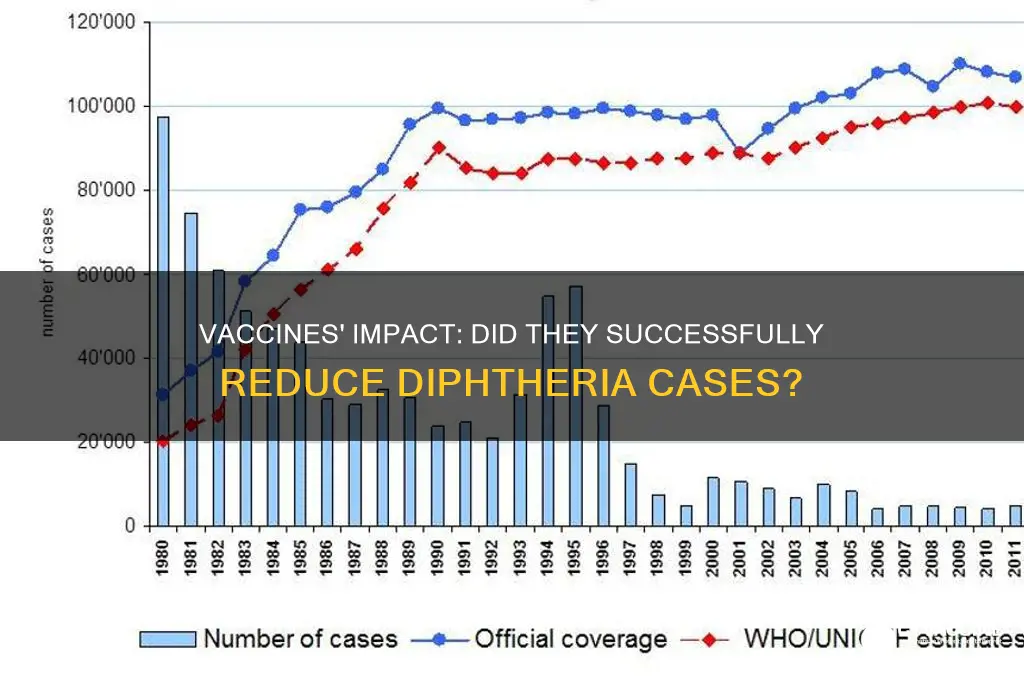
| WHO Data (Latest) | Reported cases dropped from ~100,000 annually in the 1980s to <10,000 now. |
| Mortality Rate Decline | Diphtheria-related deaths decreased by >99% in vaccinated populations. |
| Herd Immunity Impact | Vaccination programs significantly reduced disease transmission. |
| Resurgence Risk | Outbreaks occur in areas with low vaccination coverage (e.g., Ukraine 2015). |
| Vaccine Efficacy | Diphtheria vaccines are ~90-95% effective in preventing severe disease. |
| Long-Term Immunity | Booster doses required every 10 years to maintain immunity. |
| Global Eradication Status | Not eradicated but controlled in most regions due to vaccination. |
Explore related products






What You'll Learn
![]()
Historical diphtheria cases before vaccines
Before the advent of vaccines, diphtheria was a pervasive and often deadly disease, particularly among children. Historical records from the late 19th and early 20th centuries reveal staggering statistics: in the United States alone, annual cases peaked at over 200,000 in 1921, with approximately 15,000 deaths, mostly in children under 15. Globally, the situation was equally dire, with outbreaks decimating communities and leaving survivors with long-term complications such as heart damage and paralysis. These numbers underscore the pre-vaccine era as a time of constant fear and vulnerability, especially for parents.
Consider the mechanics of diphtheria’s spread to understand its historical impact. Caused by *Corynebacterium diphtheriae*, the disease thrives in crowded, unsanitary conditions, making it a scourge of urban areas. Before vaccines, containment relied on isolation, antitoxin treatments, and improved hygiene—measures that were often ineffective or inaccessible. For instance, the antitoxin, derived from horses, required careful dosage adjustments (typically 20,000–100,000 units for severe cases) and carried risks of allergic reactions. This treatment, while lifesaving for some, was no substitute for prevention, leaving populations at the mercy of the bacterium’s relentless spread.
A comparative analysis of pre-vaccine diphtheria outbreaks highlights the disease’s unpredictability and severity. The 1925 Nome, Alaska, outbreak, for example, illustrates the challenges of managing diphtheria in remote areas. With no road access and a looming blizzard, a relay of dogsled teams delivered antitoxin serum in a race against time, saving the town’s children. This event, known as the "Great Race of Mercy," exemplifies the desperation of pre-vaccine interventions. In contrast, urban centers faced recurring epidemics, such as the 1900s outbreaks in New York City, where mortality rates among children under 5 reached 80% in some neighborhoods. These disparities reveal how geography and resources shaped survival outcomes.
Persuasively, the historical data on diphtheria cases before vaccines serves as a stark reminder of the disease’s pre-vaccination toll. In the absence of immunization, societies relied on reactive measures that were costly, inconsistent, and often futile. For instance, schools and public spaces frequently closed during outbreaks, disrupting daily life and economies. Families lived in perpetual anxiety, knowing a single cough or sore throat could signal a life-threatening infection. This era of uncertainty ended only with the introduction of the diphtheria toxoid vaccine in the 1920s and its subsequent integration into routine childhood immunizations by the mid-20th century.
Practically, understanding pre-vaccine diphtheria cases offers lessons for modern public health. It underscores the importance of proactive prevention over reactive treatment, particularly in resource-limited settings. For parents today, the historical context provides a compelling reason to adhere to vaccination schedules: the diphtheria vaccine, often administered as DTaP (diphtheria, tetanus, and pertussis) for children under 7 and Tdap for older age groups, has reduced global incidence by over 90%. Skipping doses or delaying vaccination risks not only individual health but also community immunity, potentially reviving a disease that once thrived in the absence of such safeguards.
Unvaccinated Risks: Resurgent Childhood Diseases Threatening Public Health Again
You may want to see also
Explore related products



$32.64 $32.99



![]()
Diphtheria incidence rates post-vaccination
The introduction of diphtheria vaccines in the early 20th century marked a turning point in the battle against this once-common and often fatal disease. Historical data reveals a dramatic decline in incidence rates post-vaccination, particularly in regions with high immunization coverage. For instance, in the United States, diphtheria cases plummeted from over 200,000 annually in the 1920s to fewer than 5 cases per year by the 2000s. This trend is not isolated; countries like Canada, the UK, and Australia report similarly striking reductions, underscoring the vaccine’s efficacy in controlling the disease.
Analyzing the data, the correlation between vaccination rates and diphtheria incidence is unmistakable. In populations where vaccination coverage exceeds 80%, the disease becomes rare, often confined to sporadic outbreaks in undervaccinated communities. For example, a 2010 study in the *Journal of Infectious Diseases* highlighted that regions with vaccination rates below 70% experienced diphtheria outbreaks, while areas maintaining higher coverage remained largely unaffected. This evidence reinforces the principle that herd immunity, achieved through widespread vaccination, is critical in suppressing diphtheria transmission.
Practical implementation of diphtheria vaccination involves a series of doses, typically administered as part of the DTaP (Diphtheria, Tetanus, and Pertussis) vaccine for children under 7, followed by Tdap boosters for adolescents and adults. The Centers for Disease Control and Prevention (CDC) recommends a 5-dose series for children, starting at 2 months of age, with boosters every 10 years thereafter. Adherence to this schedule ensures sustained immunity and minimizes the risk of infection. Notably, even in cases where vaccinated individuals contract diphtheria, the severity of symptoms is significantly reduced, further demonstrating the vaccine’s protective benefits.
Comparatively, regions with inconsistent vaccination programs serve as cautionary examples. In the 1990s, the former Soviet Union experienced a resurgence of diphtheria, with over 150,000 cases and 5,000 deaths, largely due to declining vaccination rates post-dissolution. This outbreak starkly contrasts with the near-elimination of the disease in countries with robust immunization systems. Such disparities highlight the fragility of progress and the need for continuous vigilance in maintaining high vaccination coverage.
In conclusion, the post-vaccination decline in diphtheria incidence rates is a testament to the power of immunization in disease prevention. However, this success is not irreversible. Ongoing efforts to educate communities, address vaccine hesitancy, and ensure equitable access to vaccines are essential to sustain these gains. As global health systems navigate emerging challenges, the lessons from diphtheria’s decline offer a blueprint for combating other vaccine-preventable diseases.
Government Mandates vs. Personal Choice: The Vaccination Debate Explored
You may want to see also
Explore related products



$12.79 $19.95



![]()
Vaccine effectiveness in preventing diphtheria
Diphtheria, once a leading cause of childhood mortality, has seen a dramatic decline in incidence since the introduction of vaccination programs. Historical data reveals that in the early 20th century, the United States alone reported over 200,000 cases annually, with fatality rates exceeding 10%. By 2020, fewer than five cases were reported per year, a reduction of over 99.9%. This near-eradication is directly attributable to the widespread administration of the diphtheria toxoid vaccine, typically given as part of the DTaP (Diphtheria, Tetanus, and Pertussis) or Tdap vaccines. The vaccine’s effectiveness lies in its ability to stimulate the production of antitoxins, neutralizing the potent exotoxin produced by *Corynebacterium diphtheriae*, the bacterium responsible for the disease.
To understand vaccine effectiveness, consider the immunological response it triggers. A standard DTaP series consists of five doses administered at 2, 4, 6, 15-18 months, and 4-6 years of age. Each dose contains 20-30 international units (IU) of diphtheria toxoid, sufficient to induce protective antitoxin levels in over 95% of recipients. Booster doses, such as Tdap (10 IU diphtheria toxoid), are recommended at age 11-12 and every 10 years thereafter to maintain immunity. Studies show that after completing the primary series, individuals have a 97% reduced risk of contracting diphtheria compared to unvaccinated populations. However, waning immunity over time underscores the importance of adhering to booster schedules, particularly for adults and travelers to regions with lower vaccination coverage.
A comparative analysis of vaccinated and unvaccinated populations further highlights the vaccine’s impact. In countries with high vaccination rates, such as the U.S. and Western Europe, diphtheria is virtually nonexistent. Conversely, outbreaks persist in regions with disrupted healthcare systems or vaccine hesitancy. For instance, the 1990s epidemic in the former Soviet Union, where vaccination rates plummeted, resulted in over 150,000 cases and 5,000 deaths. This stark contrast demonstrates that the vaccine not only prevents individual cases but also disrupts community transmission, a phenomenon known as herd immunity. Achieving and maintaining herd immunity requires vaccination rates of at least 80-85%, emphasizing the collective responsibility in disease eradication efforts.
Practical considerations for maximizing vaccine effectiveness include proper storage and administration. The DTaP vaccine must be stored between 2°C and 8°C to preserve its potency, and healthcare providers should follow strict protocols to ensure accurate dosing. Parents and caregivers should monitor children for mild side effects, such as soreness at the injection site or low-grade fever, which typically resolve within 48 hours. For individuals with egg allergies or previous adverse reactions, consultation with an allergist or immunologist is advised before vaccination. Additionally, travelers to endemic areas should verify their immunization status and receive a booster if necessary, as diphtheria remains a threat in parts of Asia, Africa, and South America.
In conclusion, the effectiveness of diphtheria vaccines is irrefutable, as evidenced by the disease’s near disappearance in regions with robust vaccination programs. By adhering to recommended schedules, maintaining herd immunity, and addressing logistical challenges, societies can sustain this success. The diphtheria vaccine stands as a testament to the power of immunization in transforming public health, offering a blueprint for combating other vaccine-preventable diseases.
Unveiling the Design: A Randomized Double-Blind Vaccine Study Explained
You may want to see also
Explore related products






![]()
Global diphtheria outbreaks and vaccination
Diphtheria, a once-feared bacterial infection causing severe respiratory symptoms and potential heart and nerve damage, has seen a dramatic decline in global cases since the introduction of vaccination programs. Historical data reveals a stark contrast: in the prevaccine era, diphtheria claimed hundreds of thousands of lives annually, particularly among children. The World Health Organization (WHO) estimates that before widespread vaccination, diphtheria caused over 1 million cases and 100,000 deaths globally each year. This section delves into the role of vaccination in curbing diphtheria outbreaks, examining its impact, challenges, and ongoing efforts to maintain control.
The Vaccine’s Mechanism and Efficacy
The diphtheria vaccine, typically administered as part of the DTaP (diphtheria, tetanus, pertussis) or Tdap combination, works by stimulating the production of antitoxins that neutralize the harmful effects of the *Corynebacterium diphtheriae* toxin. A primary series of three doses, given at 2, 4, and 6 months of age, provides robust immunity, with booster doses recommended at 15–18 months, 4–6 years, and every 10 years thereafter for adolescents and adults. Studies show that vaccination reduces the risk of diphtheria by over 90%, with herd immunity playing a critical role in protecting unvaccinated individuals. For instance, in countries with high vaccination coverage, such as the United States and the United Kingdom, diphtheria cases have plummeted to near zero, demonstrating the vaccine’s efficacy.
Global Outbreaks: A Tale of Inequity
Despite the vaccine’s success, diphtheria outbreaks persist in regions with low vaccination coverage, fragile healthcare systems, and displacement crises. Recent outbreaks in countries like Yemen, Bangladesh, and Indonesia highlight the vulnerability of populations lacking access to routine immunization. In 2018, a diphtheria outbreak in Rohingya refugee camps in Bangladesh resulted in over 6,000 suspected cases and 45 deaths, underscoring the disease’s ability to exploit gaps in immunity. These outbreaks serve as a stark reminder that global eradication requires equitable vaccine distribution and strengthened healthcare infrastructure, particularly in conflict-affected and low-resource settings.
Challenges to Vaccination Efforts
Several factors hinder diphtheria control, including vaccine hesitancy, supply chain disruptions, and competing health priorities. Misinformation about vaccine safety, often spread through social media, has led to declining vaccination rates in some regions, leaving communities susceptible to outbreaks. Additionally, the diphtheria vaccine’s requirement for cold chain storage poses logistical challenges in areas with limited refrigeration capacity. Addressing these barriers demands targeted public health campaigns, investment in vaccine delivery systems, and international collaboration to ensure consistent supply and access.
Practical Steps for Prevention and Response
To mitigate the risk of diphtheria outbreaks, individuals and communities should prioritize timely vaccination, especially for children and travelers to endemic areas. Healthcare providers must remain vigilant for symptoms—such as a thick gray throat membrane, fever, and swollen lymph nodes—and promptly administer antitoxin and antibiotics when cases arise. Public health officials should implement outbreak response plans that include mass vaccination campaigns, contact tracing, and antimicrobial prophylaxis for close contacts. By combining preventive measures with rapid response strategies, the global community can sustain progress against diphtheria and prevent its resurgence.
In conclusion, while vaccines have undeniably transformed diphtheria from a global scourge to a rare disease in many parts of the world, ongoing outbreaks underscore the need for sustained vigilance and equitable access to immunization. The fight against diphtheria is a testament to the power of vaccination—but it is also a call to action to address the gaps that allow this preventable disease to persist.
Debunking Gardasil Myths: Why the Vaccine Faces Unfair Criticism
You may want to see also
Explore related products






![]()
Diphtheria mortality decline with vaccines
The introduction of diphtheria vaccines in the early 20th century marked a turning point in the battle against this once-feared disease. Historical data reveals a dramatic decline in mortality rates following widespread immunization campaigns. For instance, in the United States, annual diphtheria-related deaths plummeted from over 15,000 in the 1920s to fewer than 10 by the 1970s. This trend is not isolated; similar patterns emerged globally, demonstrating the vaccine’s efficacy in saving lives. The diphtheria toxoid vaccine, typically administered as part of the DTaP (Diphtheria, Tetanus, and Pertussis) or Tdap series, has been instrumental in this decline. For children, the CDC recommends a series of five doses starting at 2 months of age, with boosters every 10 years to maintain immunity.
Analyzing the mechanism of the vaccine provides insight into its success. Diphtheria vaccines work by neutralizing the toxin produced by *Corynebacterium diphtheriae*, the bacterium responsible for the disease. This toxin causes severe complications, including respiratory obstruction and heart failure, which are primary drivers of mortality. By inducing the production of antitoxins, the vaccine prevents the toxin from causing harm, even if infection occurs. Studies show that vaccinated individuals are 95% less likely to develop severe diphtheria compared to the unvaccinated. This protective effect is particularly critical for children under 5 and adults over 60, who are at higher risk of complications.
A comparative analysis of regions with varying vaccination rates underscores the vaccine’s impact. In countries with high immunization coverage, such as the United States and Western Europe, diphtheria has become a rarity. Conversely, outbreaks persist in areas with low vaccination rates, such as parts of Southeast Asia and Africa. For example, a 2017 outbreak in Indonesia resulted in over 100 deaths, primarily among unvaccinated individuals. This contrast highlights the direct correlation between vaccine accessibility and mortality reduction. Public health initiatives must prioritize equitable vaccine distribution to sustain global progress.
Practical steps to maximize the vaccine’s effectiveness include adhering to recommended dosing schedules and ensuring proper storage of vaccine supplies. Health workers should educate communities about the importance of completing the full vaccine series and receiving boosters. In resource-limited settings, cold chain logistics are critical to maintaining vaccine potency. Additionally, surveillance systems must be strengthened to detect and respond to outbreaks promptly. By combining vaccination with improved sanitation and access to antibiotics, societies can further reduce the burden of diphtheria.
The decline in diphtheria mortality is a testament to the power of vaccination as a public health tool. However, complacency poses a risk, as waning immunity and vaccine hesitancy can lead to resurgence. The 1990s outbreak in the former Soviet Union, which resulted in over 5,000 deaths, serves as a cautionary tale. To sustain progress, ongoing investment in vaccine infrastructure and public awareness campaigns is essential. The story of diphtheria’s decline is not just a historical success but a blueprint for combating other vaccine-preventable diseases.
Vaccine Formulas: One Vaccine, Many Recipes
You may want to see also
Frequently asked questions
Yes, vaccines have been highly effective in reducing diphtheria cases globally. Before the introduction of the diphtheria vaccine in the 1920s, the disease was a major cause of childhood illness and death. Widespread vaccination campaigns have led to a 90% decrease in reported cases worldwide, making it a rare disease in many countries.
While rare, diphtheria can still occur in vaccinated populations, especially in areas with low vaccination rates or among individuals who have not received booster shots. Vaccination provides strong protection, but no vaccine is 100% effective, and immunity can wane over time without proper boosters.
Diphtheria remains a concern in some countries due to inadequate vaccination coverage, lack of access to healthcare, and the persistence of the bacterium in the environment. Outbreaks can occur in regions with low immunization rates, emphasizing the importance of maintaining high vaccination levels globally.