The claim that Donald Trump froze childhood MMR (measles, mumps, rubella) vaccinations is not supported by factual evidence. Throughout his presidency, Trump did not implement any policies or executive actions to halt or freeze the administration of childhood vaccines, including the MMR vaccine. In fact, during his tenure, the Centers for Disease Control and Prevention (CDC) and other health agencies continued to recommend and support routine childhood immunizations. Trump’s public statements on vaccines have been mixed, with some comments raising concerns about vaccine safety, particularly in relation to autism, a claim that has been widely debunked by scientific research. However, these remarks did not translate into policy changes affecting the MMR vaccine or other childhood immunizations. The MMR vaccine remains a critical component of public health efforts to prevent infectious diseases, and its administration has continued uninterrupted under federal guidelines.
| Characteristics | Values |
|---|---|
| Claim | Trump froze childhood MMR vaccination |
| Fact-Check | False |
| Evidence | No official policy or executive order from the Trump administration freezing childhood MMR vaccinations. |
| CDC Guidance | The CDC continued to recommend MMR vaccinations for children throughout Trump's presidency. |
| Vaccination Rates | Childhood vaccination rates, including MMR, remained stable during Trump's presidency (2017-2021). |
| Source of Misinformation | Likely stemmed from misinformation campaigns or misinterpretation of vaccine-related policies. |
| Relevant Policies | Trump administration focused on COVID-19 vaccine development and distribution, not on restricting existing childhood vaccines. |
| Current Status | MMR vaccination remains a standard part of childhood immunization schedules in the U.S. |
Explore related products


$11.93 $21.99




What You'll Learn
![]()
Trump's Stance on Vaccines
Former President Donald Trump's stance on vaccines, particularly the MMR (measles, mumps, rubella) vaccine, has been marked by inconsistency and controversy. During his presidency, Trump made several public statements that both supported and questioned vaccine safety, often amplifying misinformation that fueled hesitancy among some groups. For instance, in a 2014 tweet, Trump falsely linked childhood vaccines to autism, a claim debunked by extensive scientific research. However, during the COVID-19 pandemic, he shifted gears, championing the rapid development of vaccines under Operation Warp Speed, even receiving the vaccine himself in private. This duality in his messaging has left a lasting impact on public perception of vaccines, including routine childhood immunizations like the MMR.
Analyzing Trump's actions during his presidency reveals a lack of direct interference with childhood vaccination programs, including the MMR vaccine. Despite his occasional skepticism, there is no evidence that his administration froze or halted the distribution or administration of childhood vaccines. The Centers for Disease Control and Prevention (CDC) and state health departments continued to recommend and administer the MMR vaccine according to the standard schedule: the first dose at 12–15 months and the second dose at 4–6 years. Trump's rhetoric, however, contributed to a broader climate of mistrust in vaccines, which may have indirectly influenced vaccination rates in certain communities.
From a practical standpoint, parents seeking clarity on the MMR vaccine should focus on evidence-based guidance rather than political statements. The MMR vaccine is highly effective, with two doses providing 97% protection against measles, 88% against mumps, and 97% against rubella. Side effects are typically mild, such as fever or rash, and occur in less than 10% of recipients. To ensure timely protection, adhere to the CDC’s recommended schedule and consult a pediatrician if you have concerns. Delaying or skipping doses increases the risk of outbreaks, as seen in recent measles resurgences linked to vaccine hesitancy.
Comparatively, Trump's approach to vaccines stands in contrast to the consistent messaging of public health experts and previous administrations. While he did not implement policies to freeze childhood vaccinations, his mixed signals created confusion and eroded trust in institutions like the CDC. For example, his 2019 meeting with anti-vaccine activists at the White House raised alarms among health professionals, even though no policy changes resulted. This highlights the power of presidential rhetoric in shaping public health behaviors, even without direct legislative action.
In conclusion, while Trump did not freeze childhood MMR vaccinations, his inconsistent and often misleading statements on vaccine safety have had tangible consequences. Parents and caregivers must prioritize reliable information from trusted sources like the CDC and WHO when making decisions about immunizations. The MMR vaccine remains a critical tool in preventing serious diseases, and maintaining high vaccination rates is essential for community immunity. Trump's legacy on this issue serves as a reminder of the importance of clear, science-based communication in public health.
Affordable Vaccine: Dementia Prevention or Pipe Dream?
You may want to see also
Explore related products






![]()
MMR Vaccine Safety Concerns
The MMR vaccine, a cornerstone of childhood immunization, has faced persistent safety concerns despite overwhelming scientific evidence supporting its efficacy and safety. One of the most notorious claims linking the MMR vaccine to autism, stemming from a fraudulent 1998 study by Andrew Wakefield, has been thoroughly debunked. Yet, this misinformation continues to circulate, fueled by anti-vaccine movements and, at times, amplified by public figures. For instance, former President Trump’s comments during the 2016 presidential debates and on social media raised questions about vaccine schedules, though he later clarified support for vaccination. Such statements, even when not directly advocating against vaccines, can sow doubt among parents already hesitant about the MMR vaccine’s safety.
Analyzing the safety profile of the MMR vaccine reveals a rigorous testing and monitoring process. The vaccine contains weakened forms of measles, mumps, and rubella viruses, administered typically in two doses: the first at 12–15 months and the second at 4–6 years. Common side effects are mild, including fever, rash, or soreness at the injection site, occurring in less than 10% of recipients. Serious adverse events, such as severe allergic reactions, are exceedingly rare, estimated at 1 in a million doses. Compare this to the risks of the diseases themselves: measles can lead to pneumonia, encephalitis, and death in 1–3 per 1,000 cases. The vaccine’s benefits far outweigh its minimal risks, a fact underscored by global health organizations like the CDC and WHO.
For parents navigating MMR vaccine safety concerns, practical steps can alleviate anxiety. First, consult a pediatrician to discuss your child’s medical history, as certain conditions (e.g., severe immune system disorders) may warrant delaying or avoiding vaccination. Second, verify information sources; rely on peer-reviewed studies and official health guidelines rather than anecdotal claims or social media posts. Third, monitor your child post-vaccination for any unusual symptoms, though serious reactions are rare. Finally, consider the community impact: vaccinating your child contributes to herd immunity, protecting vulnerable populations like infants too young to be vaccinated and immunocompromised individuals.
A comparative look at countries with high MMR vaccination rates versus those with low rates highlights the vaccine’s importance. In the U.S., where MMR coverage is around 90%, measles outbreaks remain sporadic. Conversely, countries with lower vaccination rates, such as Ukraine or the Philippines, have seen devastating measles epidemics in recent years, with thousands of cases and hundreds of deaths. This contrast underscores the vaccine’s role in disease prevention and the dangers of misinformation-driven hesitancy. While no medical intervention is entirely risk-free, the MMR vaccine’s safety record is robust, supported by decades of data and billions of doses administered worldwide.
In conclusion, MMR vaccine safety concerns, though persistent, are largely unfounded. The vaccine’s minimal risks pale in comparison to the severe consequences of measles, mumps, and rubella. Parents should approach these concerns with a critical eye, prioritizing evidence-based information and expert guidance. By doing so, they not only protect their children but also contribute to public health at large, ensuring these preventable diseases remain a relic of the past.
Vaccine Pain and Immunity: Is There a Link?
You may want to see also
Explore related products






![]()
Childhood Vaccination Policies
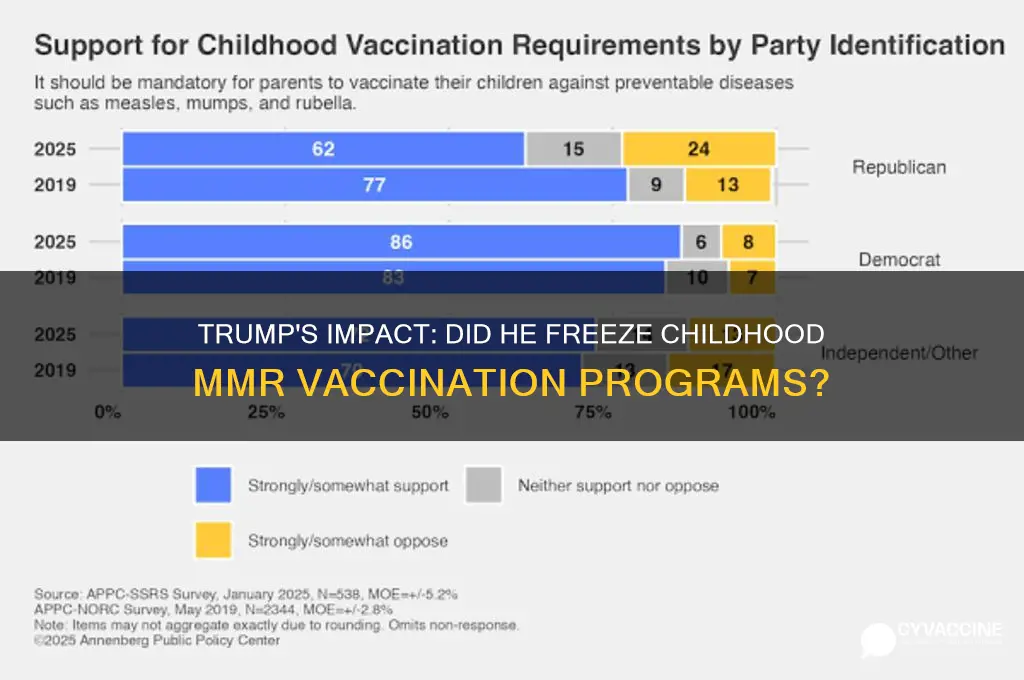
Analyzing the impact of political rhetoric on vaccination policies reveals a critical lesson: consistency in messaging is vital. Trump’s suggestion in 2017 that vaccines might be linked to autism, despite overwhelming evidence to the contrary, underscored the need for leaders to rely on scientific consensus. Childhood vaccination policies are not merely administrative directives but lifelines for communities. A single MMR dose is 93% effective against measles, while two doses raise protection to 97%. When policies are questioned without basis, it erodes confidence, particularly among parents navigating conflicting information. Policymakers must prioritize transparency, such as publishing vaccination schedules with clear age-specific guidelines and addressing concerns through trusted public health channels.
Implementing effective childhood vaccination policies requires a multi-pronged approach. First, ensure accessibility by integrating vaccines into routine pediatric care and offering catch-up schedules for missed doses. Second, combat misinformation through education campaigns that emphasize the safety and efficacy of vaccines like MMR. For example, schools can mandate vaccination records while providing exemptions only for medical reasons, not personal beliefs. Third, leverage technology, such as reminder systems for parents, to improve adherence. A study in *Pediatrics* found that text message reminders increased vaccination rates by 4.5%. These steps, combined with consistent leadership, can fortify policies against political interference.
Comparing childhood vaccination policies globally offers insights into best practices. Countries like Japan, which historically faced vaccine hesitancy after a 1993 MMR controversy, have since reinstated robust programs with public education campaigns. In contrast, the U.S.’s decentralized approach leaves vaccination rates vulnerable to regional disparities. A federal policy mandating uniform schedules, while respecting state autonomy, could bridge this gap. Additionally, incentivizing vaccination through initiatives like vaccine-preventable disease tracking can demonstrate the tangible benefits of adherence. For parents, practical tips include scheduling vaccinations during well-child visits and keeping immunization records updated for school enrollment.
Ultimately, childhood vaccination policies must be shielded from political whims to remain effective. While Trump did not freeze MMR vaccination programs, his rhetoric underscored the fragility of public trust in science-driven policies. Policymakers should focus on evidence, accessibility, and education to sustain high vaccination rates. Parents can support this by following the CDC’s recommended MMR schedule and advocating for science-based policies in their communities. In an era of misinformation, the strength of vaccination programs lies not just in their design but in the collective commitment to their success.
Does CVS Accept Medicaid for Vaccines? A Comprehensive Guide
You may want to see also
Explore related products





![]()
Public Health Impact Analysis
A critical examination of the alleged freeze on childhood MMR vaccinations under the Trump administration reveals no evidence of such a policy. The MMR vaccine, administered in two doses—the first at 12–15 months and the second at 4–6 years—remains a cornerstone of pediatric immunization schedules. Public health data from the CDC shows consistent vaccination rates during this period, with no abrupt disruptions attributable to federal intervention. This stability underscores the importance of evidence-based policy analysis, as misinformation can erode trust in life-saving vaccines.
Analyzing the hypothetical impact of a freeze on MMR vaccinations highlights the fragility of herd immunity. A 5% drop in MMR coverage could increase measles cases by 50%, according to modeling studies. Measles, with a basic reproduction number (R0) of 12–18, spreads rapidly in unvaccinated populations. For context, a single case in a school with 90% vaccination coverage could still infect 1–2 susceptible children. Public health systems must therefore prioritize accurate communication to prevent unfounded fears from reducing vaccination uptake.
Instructively, maintaining vaccination programs requires robust supply chain management and clear public messaging. The MMR vaccine’s storage at 2°C–8°C and its administration via subcutaneous injection are technical details often overlooked but critical for efficacy. Healthcare providers should emphasize that delaying or skipping doses leaves children vulnerable to complications like pneumonia, encephalitis, and lifelong disabilities. Parents should be encouraged to adhere to the CDC’s recommended schedule, using tools like vaccine reminder apps or clinic follow-ups.
Comparatively, countries with disrupted vaccination programs offer cautionary tales. During the 2018–2020 measles outbreak in Europe, nations with vaccination rates below 95% saw over 100,000 cases. In contrast, the U.S. maintained a 91% MMR coverage rate during the same period, avoiding similar outbreaks. This disparity illustrates the direct correlation between policy stability and public health outcomes. Policymakers must learn from these examples to safeguard immunization programs against political or logistical interference.
Persuasively, the absence of a Trump-era MMR freeze should not distract from ongoing challenges. Vaccine hesitancy, exacerbated by misinformation, remains a threat. Public health campaigns must counter myths with accessible, science-backed information. For instance, explaining that the MMR vaccine contains less than 0.0015 mg of neomycin—far below allergenic thresholds—can reassure concerned parents. By focusing on transparency and education, stakeholders can protect the gains made in childhood immunization and prevent future setbacks.
Japan's Vaccine Rollout: Unraveling the Delays and Challenges
You may want to see also
Explore related products






![]()
Misinformation and Vaccine Hesitancy
Misinformation about vaccines, particularly the MMR (measles, mumps, rubella) vaccine, has been a persistent issue, often fueled by unverified claims and political rhetoric. One such claim—that former President Trump froze childhood MMR vaccinations—has circulated, despite lacking factual basis. This rumor exemplifies how misinformation can exploit public uncertainty, especially during times of political polarization or health crises. The MMR vaccine, typically administered in two doses (the first at 12-15 months and the second at 4-6 years), remains a cornerstone of childhood immunization, preventing diseases that once caused widespread harm. Yet, false narratives like this can erode trust, leading to vaccine hesitancy and potentially dangerous delays in vaccination schedules.
Analyzing the impact of such misinformation reveals a troubling pattern: it often preys on parental concerns about vaccine safety. For instance, debunked studies linking the MMR vaccine to autism have lingered in public memory, making fertile ground for new falsehoods. When political figures or social media influencers amplify these claims, they gain an air of legitimacy, even if unsupported by scientific evidence. This dynamic underscores the need for clear, accessible communication from health authorities. Parents should be encouraged to consult trusted sources like the CDC or WHO, which provide detailed guidelines on vaccine safety and efficacy, rather than relying on unverified online claims.
To combat vaccine hesitancy, it’s essential to address the root causes of mistrust. One practical step is to educate parents about the rigorous testing vaccines undergo before approval. For example, the MMR vaccine has been in use since the 1970s, with extensive data confirming its safety and effectiveness. Healthcare providers can play a critical role by engaging in open, non-judgmental conversations with hesitant parents, addressing their concerns with empathy and evidence. Additionally, public health campaigns should highlight success stories, such as the near-eradication of measles in the U.S. before recent outbreaks linked to declining vaccination rates.
Comparing the spread of misinformation about the MMR vaccine to other health-related falsehoods reveals a common thread: the exploitation of fear and uncertainty. Just as myths about COVID-19 vaccines led to hesitancy, claims about the MMR vaccine freezing under Trump tap into broader anxieties about government overreach or hidden agendas. To counter this, fact-checking organizations and media outlets must prioritize accuracy and transparency. Parents should be taught to critically evaluate sources, looking for credentials, peer-reviewed studies, and consensus among experts. By fostering media literacy, we can empower individuals to discern truth from fiction.
Ultimately, the fight against misinformation requires a multi-faceted approach. Health professionals, educators, and policymakers must collaborate to build a culture of trust and informed decision-making. For parents, staying informed means following vaccination schedules, understanding the mild side effects (e.g., fever or rash in 5-15% of cases), and recognizing the far greater risks of forgoing immunization. Misinformation may persist, but with vigilance and education, its impact on vaccine hesitancy can be minimized, ensuring the continued protection of children through proven vaccines like the MMR.
Vaccine-Induced Immunity: How Vaccines Build Long-Term Protection Against Diseases
You may want to see also
Frequently asked questions
No, there is no evidence that Donald Trump froze or halted childhood MMR (measles, mumps, rubella) vaccinations during his presidency.
No, Trump did not issue any executive orders to freeze or restrict childhood MMR vaccinations.
There were no federal policy changes under Trump specifically targeting or freezing MMR vaccinations. However, his administration did promote vaccine hesitancy through certain statements and actions.
While Trump’s comments on vaccines may have contributed to vaccine hesitancy among some groups, there is no direct evidence of a freeze on MMR vaccinations. Vaccination rates were primarily managed at the state and local levels.
No, there were no widespread reports of MMR vaccine shortages or freezes during Trump’s presidency. Vaccines remained available through standard healthcare channels.