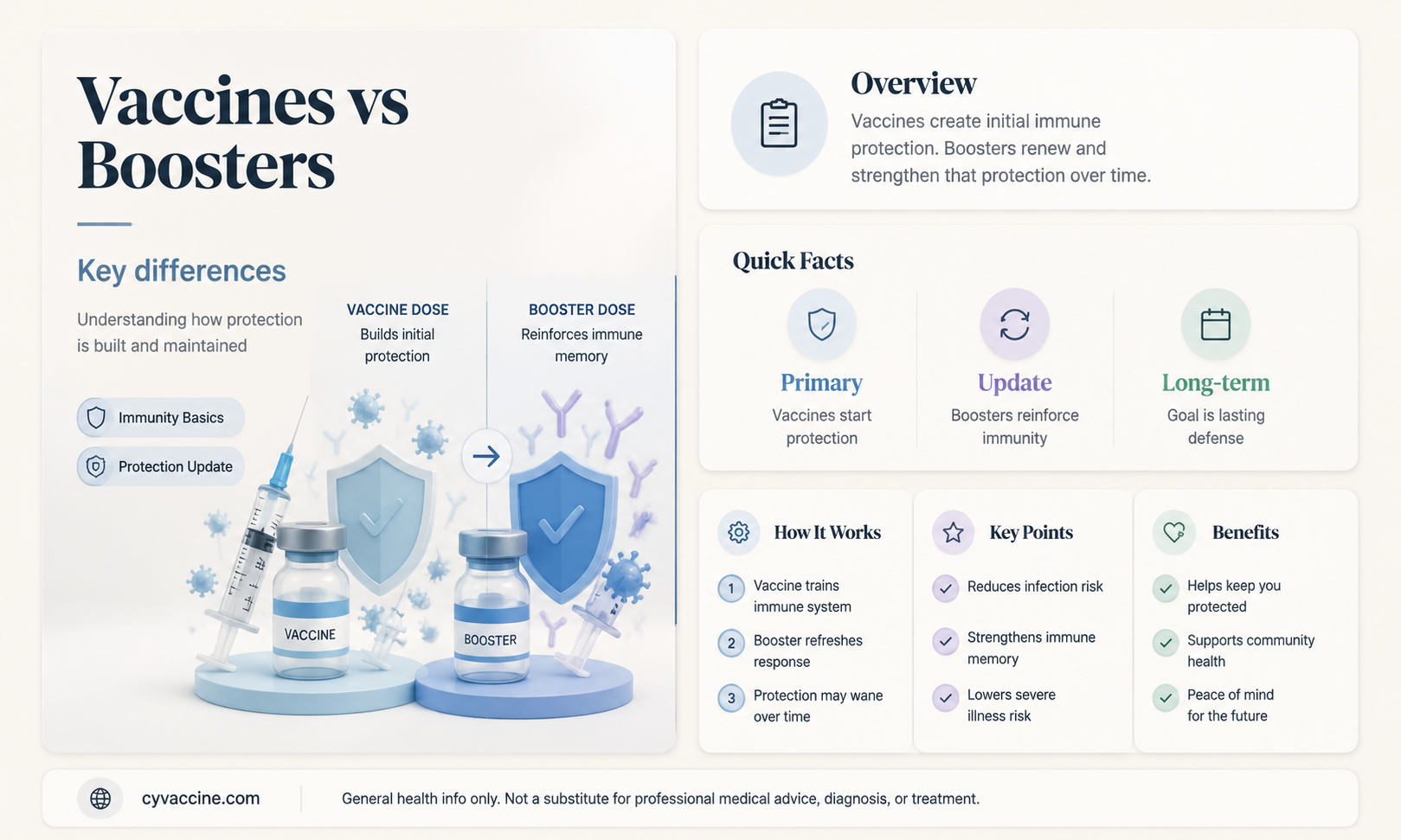
Vaccines and boosters are related but distinct components of immunization strategies. Vaccines are initial doses administered to stimulate the immune system to recognize and combat specific pathogens, such as viruses or bacteria. They typically contain weakened or inactivated forms of the pathogen or its components, triggering the production of antibodies and memory cells for future protection. Boosters, on the other hand, are additional doses given after the initial vaccine series to reinforce immunity. Over time, immune responses may wane, making boosters necessary to maintain protection against diseases. While both vaccines and boosters aim to enhance immunity, they serve different purposes: vaccines establish the foundation of immunity, while boosters strengthen and prolong it. Understanding this distinction is crucial for effective vaccination programs and public health initiatives.
Explore related products





What You'll Learn
- Vaccine Basics: Initial doses to build immunity against diseases, primary prevention method
- Booster Purpose: Additional doses to enhance or restore waning immunity over time
- Composition Differences: Boosters may have same or updated formulas targeting variants
- Timing and Frequency: Vaccines are initial, boosters given months or years later
- Immune Response: Vaccines create foundation, boosters strengthen and prolong protection
![]()
Vaccine Basics: Initial doses to build immunity against diseases, primary prevention method
Vaccines are the cornerstone of disease prevention, designed to train the immune system to recognize and combat pathogens before they cause illness. The initial doses of a vaccine, often referred to as the primary series, are critical in building this foundational immunity. For example, the measles, mumps, and rubella (MMR) vaccine requires two doses, typically administered at 12–15 months and 4–6 years of age, to ensure robust protection. These doses introduce a harmless form of the virus or its components, prompting the body to produce antibodies and memory cells that stand ready for future encounters with the actual pathogen.
The primary series is not a one-size-fits-all regimen; it varies by vaccine and age group. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) require two doses spaced 3–4 weeks apart for individuals aged 12 and older, while those aged 5–11 receive a lower dosage in two shots spaced 21–28 days apart. In contrast, the Johnson & Johnson vaccine is a single-dose regimen for adults. Adhering to the recommended schedule is crucial, as incomplete or improperly spaced doses may result in suboptimal immunity, leaving individuals vulnerable to infection.
Building immunity through initial doses is a proactive measure, serving as the first line of defense against infectious diseases. Unlike treatments that address existing illnesses, vaccines prevent diseases from taking hold in the first place. This primary prevention method reduces the risk of severe illness, hospitalization, and death, while also curbing the spread of pathogens within communities. For example, the influenza vaccine, administered annually, not only protects individuals but also helps prevent outbreaks in schools, workplaces, and healthcare settings.
Practical tips for ensuring successful vaccination include scheduling appointments well in advance, especially for multi-dose vaccines, and keeping a record of immunization dates. Parents should consult their child’s pediatrician to stay on track with the recommended vaccine schedule, which includes vaccines like DTaP (diphtheria, tetanus, pertussis), polio, and hepatitis B. Adults should also review their vaccination status, as some vaccines, such as Tdap (tetanus, diphtheria, pertussis) and shingles (Shingrix), require boosters later in life. By prioritizing initial doses, individuals contribute to both personal and public health, creating a shield against preventable diseases.
Vaccination Dangers: Separating Verifiable Risks from Misinformation and Myths
You may want to see also
Explore related products






![]()
Booster Purpose: Additional doses to enhance or restore waning immunity over time
Vaccines and boosters serve distinct roles in maintaining immunity, though they are often conflated. While a vaccine introduces the immune system to a pathogen, a booster’s purpose is to re-expose it to the same antigen, reinforcing memory cells that may have diminished over time. This is critical because immunity, whether from infection or vaccination, wanes naturally—sometimes within 6 to 12 months, depending on the vaccine. For instance, the COVID-19 mRNA vaccines initially provided robust protection, but studies showed antibody levels dropping significantly after 6 months, prompting the introduction of booster doses to restore efficacy against severe disease.
The timing and dosage of boosters are tailored to the specific vaccine and population. For example, the influenza vaccine requires annual boosters due to the virus’s rapid mutation, while the Tdap vaccine (tetanus, diphtheria, pertussis) is recommended every 10 years. COVID-19 boosters, on the other hand, are often administered 3 to 6 months after the primary series, with dosage adjustments for age groups—older adults and immunocompromised individuals may receive higher or additional doses due to their heightened risk of waning immunity. This precision underscores the booster’s role as a strategic intervention, not a one-size-fits-all solution.
Practical considerations for boosters include monitoring side effects, which are typically mild but can vary by vaccine. For instance, mRNA COVID-19 boosters may cause fatigue or muscle pain in some individuals, while the shingles vaccine booster (Shingrix) is known for more pronounced arm soreness. Scheduling is also key: avoid overlapping boosters with other vaccines when possible, and consult a healthcare provider if you’re unsure about timing. For parents, ensuring children receive boosters like the DTaP (diphtheria, tetanus, pertussis) at ages 4–6 and 11–12 is crucial for sustained protection during developmental years.
The broader takeaway is that boosters are not redundant doses but essential tools to address the biological reality of waning immunity. Without them, even fully vaccinated individuals may become susceptible to infection or severe outcomes over time. This is particularly critical for diseases like measles, where herd immunity thresholds require high and sustained antibody levels. By understanding boosters as targeted reinforcements rather than optional add-ons, individuals can make informed decisions to protect themselves and their communities.
Is Proof of Vaccination Legal? Understanding the Rights and Regulations
You may want to see also
Explore related products






![]()
Composition Differences: Boosters may have same or updated formulas targeting variants
Boosters and vaccines, while often discussed interchangeably, are not always identical in composition. A key distinction lies in their formulation, particularly when addressing evolving pathogens like SARS-CoV-2. Primary vaccines are designed to establish a foundational immune response, typically containing a standardized antigen or genetic material (e.g., mRNA) targeting the original strain of a virus. Boosters, however, may retain the same formula as the initial vaccine or incorporate updates to combat emerging variants. For instance, the COVID-19 mRNA boosters from Pfizer-BioNTech and Moderna introduced in late 2022 included bivalent formulations, targeting both the original strain and the Omicron subvariants BA.4 and BA.5. This strategic adjustment ensures continued efficacy against dominant circulating strains.
Consider the practical implications of these composition differences. If a booster uses the same formula as the primary vaccine, it serves primarily to reinforce the initial immune response, often administered at a reduced dosage. For example, the Pfizer-BioNTech COVID-19 booster for individuals aged 12 and older is 30 micrograms, half the 60-microgram dose of the primary series. Conversely, updated boosters may require a full dose to introduce new antigenic targets effectively. This variation underscores the importance of following age-specific and health-condition-based guidelines, as immunocompromised individuals or those over 65 may require tailored booster regimens.
From a persuasive standpoint, understanding these differences empowers individuals to make informed decisions about their health. Updated boosters are not merely redundant shots but strategic tools to address the dynamic nature of viral evolution. For example, the 2023-2024 flu vaccines include an updated strain of influenza A(H1N1), reflecting global surveillance data. Similarly, COVID-19 boosters with variant-specific formulas offer enhanced protection against severe disease and hospitalization, particularly for vulnerable populations. By staying informed about booster composition, individuals can align their vaccination choices with personal risk factors and public health recommendations.
A comparative analysis highlights the adaptability of boosters versus the foundational role of vaccines. While primary vaccines establish baseline immunity, boosters act as precision instruments, fine-tuning the immune system’s response to current threats. For instance, the Novavax COVID-19 booster, a protein subunit vaccine, provides an alternative for those hesitant about mRNA technology while still incorporating updated antigen designs. This diversity in composition and delivery mechanisms ensures broader accessibility and efficacy across populations. Ultimately, recognizing these differences fosters a more nuanced appreciation of vaccination strategies in combating evolving pathogens.
Global Vaccination Leaders: Top Countries with Highest Immunization Rates
You may want to see also
Explore related products






![]()
Timing and Frequency: Vaccines are initial, boosters given months or years later
Vaccines and boosters are not administered on the same timeline. Initial vaccine doses are given to introduce the immune system to a pathogen, often in a series of 1–3 shots spaced weeks apart. For example, the COVID-19 mRNA vaccines require two doses, 3–4 weeks apart for Pfizer or 4–8 weeks for Moderna. Boosters, however, are timed months or years later to reinforce immunity that may have waned. The COVID-19 booster, for instance, is recommended 5 months after the second dose for Pfizer and Moderna, or 2 months after the single-dose Johnson & Johnson vaccine. This staggered approach ensures the immune system remains primed without overwhelming it.
The timing of boosters is not arbitrary. Studies show antibody levels can drop significantly 6–12 months after initial vaccination, depending on the vaccine and individual factors like age or underlying health conditions. For example, older adults or immunocompromised individuals may require boosters sooner due to faster immune decline. The flu vaccine, on the other hand, is administered annually because the virus mutates rapidly, requiring a new formulation each year. Understanding these intervals is crucial for maximizing protection and minimizing vulnerability gaps.
Practical considerations also dictate booster timing. For children, vaccine schedules are age-specific, with boosters for vaccines like DTaP (diphtheria, tetanus, pertussis) given at 4–6 years old, and Tdap (tetanus, diphtheria, pertussis) again at 11–12 years. Adults may need boosters for tetanus every 10 years, or shingles (Shingrix) after age 50, with the second dose 2–6 months after the first. Travel vaccines, like hepatitis A, require a booster 6–12 months after the initial dose for long-term immunity. Keeping track of these timelines with a vaccination record or digital health app ensures compliance and continuity.
The frequency of boosters varies by vaccine and individual risk factors. While some, like the MMR (measles, mumps, rubella), typically require only one or two doses for lifelong immunity, others demand periodic reinforcement. For instance, the HPV vaccine (Gardasil 9) is given in two or three doses over 6–12 months for adolescents, but immunocompromised individuals may need three doses regardless of age. Boosters are not a one-size-fits-all solution; they are tailored to the vaccine’s efficacy, the pathogen’s behavior, and the recipient’s immune response. Consulting healthcare providers for personalized schedules is essential for optimal protection.
The 1918 Pandemic's End: How It Vanished Without a Vaccine
You may want to see also
Explore related products






![]()
Immune Response: Vaccines create foundation, boosters strengthen and prolong protection
Vaccines and boosters are not interchangeable, though they work in tandem to fortify the immune system. Vaccines act as the cornerstone, introducing the immune system to a pathogen—whether through a weakened or inactivated virus, a fragment of the virus, or genetic material—to trigger an initial immune response. This response includes the production of antibodies and the creation of memory cells, which "remember" the pathogen for future encounters. For instance, the COVID-19 mRNA vaccines provide a blueprint for cells to produce a harmless piece of the virus’s spike protein, teaching the immune system to recognize and combat it. Boosters, on the other hand, are designed to reinvigorate this memory, enhancing the immune response by reminding the body of the threat. Without the foundational work of the vaccine, boosters would lack the context to effectively strengthen immunity.
Consider the immune system as a security team: the vaccine trains the team to identify and neutralize a specific intruder, while the booster conducts a refresher course to ensure the team remains alert and responsive over time. This analogy highlights the distinct roles of vaccines and boosters. For example, the initial COVID-19 vaccine series primes the immune system, while a booster dose, often administered 6 months later, significantly increases antibody levels, providing better protection against variants and severe disease. Studies show that a booster can raise antibody titers by up to 20-fold, demonstrating its role in amplifying the immune response rather than initiating it.
From a practical standpoint, understanding this difference is crucial for scheduling vaccinations and boosters effectively. For children aged 5–11, the Pfizer COVID-19 vaccine is administered in two doses 21 days apart, with a booster recommended at least 5 months later. Adults, particularly those over 50 or immunocompromised, may require additional boosters due to waning immunity. For instance, the CDC recommends a second COVID-19 booster for individuals over 65, administered 4 months after the first booster. This tiered approach ensures that the immune system remains robust, adapting to the vaccine’s foundation and the booster’s reinforcement.
A common misconception is that boosters are optional if the initial vaccine series was completed. However, data from the Omicron variant surge underscores the necessity of boosters. During this period, individuals with only the primary vaccine series experienced a 10-fold higher risk of infection compared to those who received a booster. This disparity illustrates how boosters not only prolong protection but also adapt immunity to evolving pathogens. For maximum efficacy, follow the recommended dosing intervals and stay informed about updated guidelines, as these may change based on emerging variants or new research.
In summary, vaccines and boosters are distinct yet interdependent tools in immune defense. Vaccines lay the groundwork by teaching the immune system to recognize a pathogen, while boosters sharpen and sustain this response. By adhering to recommended schedules and understanding their unique roles, individuals can maximize their protection against infectious diseases. Think of it as building a house: the vaccine constructs the frame, and the booster ensures the structure remains sturdy over time. Both are essential for long-term resilience.
Understanding Routine Vaccine Schedules: A Comprehensive Definition and Guide
You may want to see also
Frequently asked questions
No, vaccines and boosters are not the same. A vaccine is the initial dose(s) given to build immunity against a disease, while a booster is an additional dose administered later to enhance or restore immunity that may have waned over time.
Boosters are designed to strengthen the immune response established by the initial vaccine. While they provide similar protection, their primary purpose is to reinforce immunity, especially against new variants or as immunity decreases.
No, boosters are only effective when administered after the initial vaccine series. They rely on the foundation of immunity built by the primary doses and are not standalone vaccines.
Side effects from boosters are generally similar to those of the initial vaccine but may be milder. Common side effects include soreness at the injection site, fatigue, headache, or fever, though they vary by individual and vaccine type.