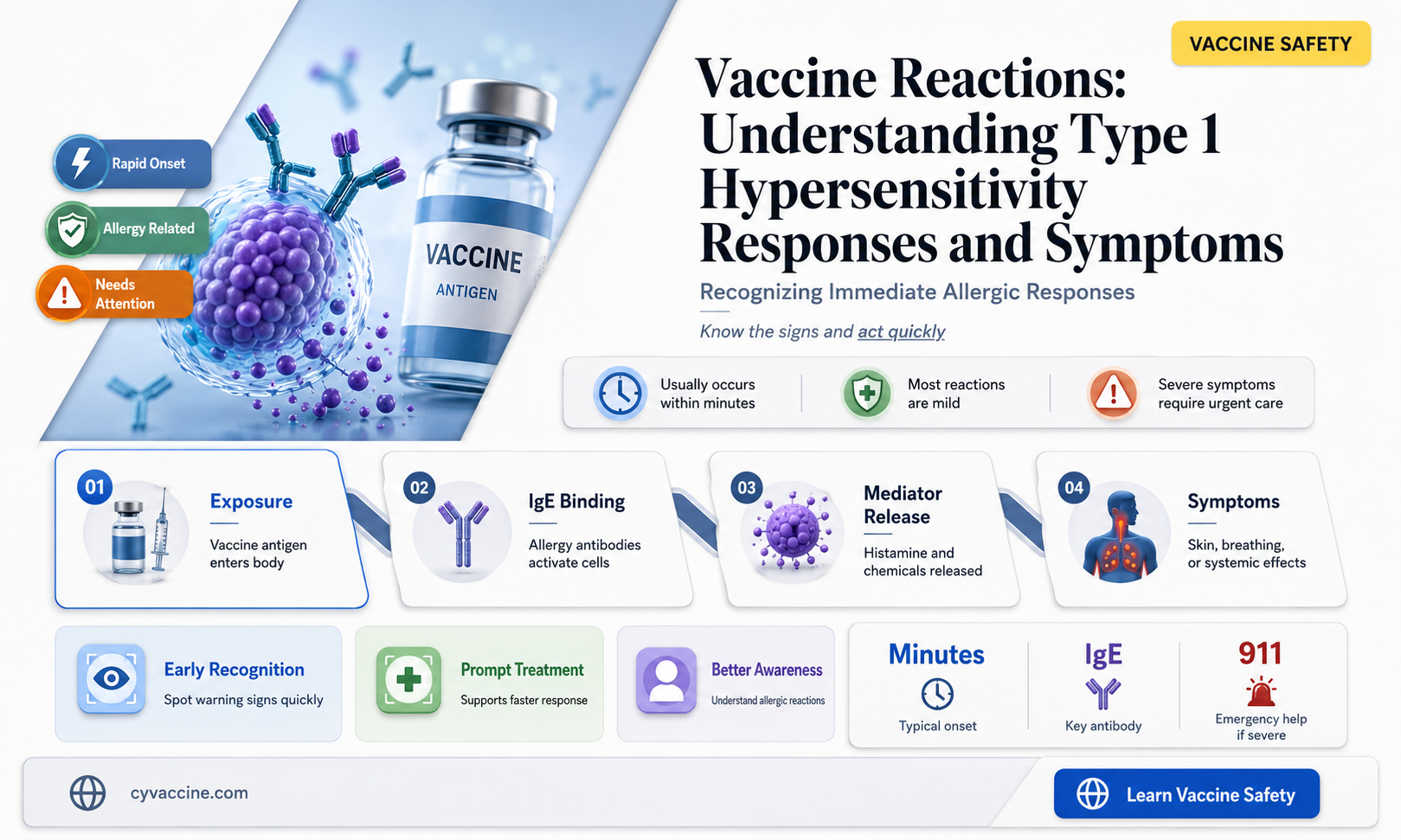
Vaccine reactions, though generally rare, have raised questions about their underlying mechanisms, particularly whether they involve Type 1 hypersensitivity, also known as immediate hypersensitivity. Type 1 hypersensitivity is an allergic reaction mediated by immunoglobulin E (IgE) antibodies, leading to the release of histamine and other inflammatory mediators, typically causing symptoms like hives, swelling, or anaphylaxis. While some vaccine reactions, such as localized redness or mild fever, are common and not allergic in nature, rare cases of severe allergic responses have been reported. These instances prompt investigation into whether they align with the Type 1 hypersensitivity pathway, especially given the involvement of IgE-mediated mechanisms in anaphylaxis. Understanding the immunological basis of vaccine reactions is crucial for improving vaccine safety, identifying at-risk populations, and developing strategies to mitigate adverse events.
| Characteristics | Values |
|---|---|
| Type of Hypersensitivity | Vaccine reactions are not typically classified as Type 1 hypersensitivity (immediate IgE-mediated reactions). |
| Mechanism | Most vaccine reactions are due to non-allergic mechanisms, such as: |
- Local reactions: Inflammation at the injection site (e.g., pain, redness, swelling) caused by vaccine components or immune activation.
- Systemic reactions: Fever, fatigue, headache, or muscle pain due to cytokine release or innate immune responses.
- Rare allergic reactions: Anaphylaxis can occur in rare cases, which is IgE-mediated (Type 1 hypersensitivity), but this is uncommon and typically linked to specific vaccine components (e.g., gelatin, egg protein, or latex). | | IgE Involvement | Type 1 hypersensitivity involves IgE antibodies and mast cell/basophil activation. Most vaccine reactions do not involve IgE, except in rare anaphylactic cases. | | Onset Time | Type 1 hypersensitivity reactions occur within minutes to hours. Most vaccine reactions (e.g., local or systemic) appear within 1-2 days post-vaccination. | | Prevalence | Type 1 hypersensitivity (anaphylaxis) post-vaccination is extremely rare (<1 case per million doses for most vaccines). | | Examples of Vaccines with Rare Type 1 Reactions | MMR (egg protein), influenza (egg-based), COVID-19 (rare cases linked to PEG or other components). | | Management | Anaphylaxis requires immediate epinephrine. Non-allergic reactions are managed symptomatically (e.g., acetaminophen for fever). | | Prevention | Screening for known allergies to vaccine components (e.g., egg, latex) before administration. |
Explore related products






What You'll Learn
- IgE-Mediated Response: Vaccines rarely trigger IgE antibodies, leading to immediate allergic reactions like anaphylaxis
- Symptoms Overview: Hives, swelling, difficulty breathing, and hypotension are common type 1 hypersensitivity signs
- Risk Factors: Pre-existing allergies or prior vaccine reactions increase susceptibility to type 1 responses
- Vaccine Components: Certain additives (e.g., gelatin, egg proteins) can act as allergens in sensitive individuals
- Management Strategies: Epinephrine, antihistamines, and monitoring are key to treating type 1 reactions post-vaccination
![]()
IgE-Mediated Response: Vaccines rarely trigger IgE antibodies, leading to immediate allergic reactions like anaphylaxis
Vaccine-induced anaphylaxis, though rare, is a critical concern in immunology, primarily linked to IgE-mediated responses. This type of reaction occurs when the immune system mistakenly identifies a vaccine component as a threat, triggering the release of IgE antibodies. These antibodies bind to mast cells and basophils, leading to the rapid release of histamine and other inflammatory mediators. The result is an immediate allergic reaction, which can manifest as hives, swelling, difficulty breathing, or, in severe cases, anaphylactic shock. Understanding this mechanism is essential for healthcare providers to recognize and manage such reactions promptly.
The incidence of IgE-mediated reactions to vaccines is exceptionally low, estimated at approximately 1.31 cases per million doses administered. For example, the influenza vaccine, which contains trace amounts of egg protein, has been associated with anaphylaxis in individuals with severe egg allergies. However, even in this population, the risk remains minimal. The MMR (Measles, Mumps, Rubella) and COVID-19 vaccines have also been rarely implicated, with reactions typically occurring within minutes to hours post-vaccination. This rarity underscores the safety profile of vaccines but highlights the need for vigilance during and immediately after administration.
To mitigate risks, pre-vaccination screening is crucial. Individuals with a history of severe allergies, particularly to vaccine components like gelatin or antibiotics, should be identified. For instance, the MMR vaccine contains gelatin, a known allergen for some. In such cases, healthcare providers may opt for skin testing or administer the vaccine in a controlled setting with immediate access to emergency treatments like epinephrine. Additionally, observing patients for 15–30 minutes post-vaccination is standard practice to ensure timely intervention if symptoms arise.
From a comparative perspective, IgE-mediated reactions differ significantly from other vaccine side effects, such as delayed-type hypersensitivity or local inflammation. While the latter are typically mild and self-limiting, IgE-mediated responses demand immediate attention. For example, a sore arm or mild fever after a vaccine is common and resolves within days, whereas anaphylaxis requires urgent epinephrine administration. This distinction emphasizes the importance of educating both healthcare providers and the public about the signs of severe allergic reactions.
In conclusion, while vaccines rarely trigger IgE-mediated responses, the potential for immediate allergic reactions like anaphylaxis necessitates preparedness. Healthcare systems must ensure that vaccination sites are equipped with emergency protocols and medications. For individuals, understanding personal allergy risks and communicating them to healthcare providers can significantly reduce the likelihood of adverse events. By balancing awareness with the proven safety of vaccines, we can continue to protect public health effectively.
Minors' Vaccination Rights: Empowering Youth or Parental Overreach?
You may want to see also
Explore related products






![]()
Symptoms Overview: Hives, swelling, difficulty breathing, and hypotension are common type 1 hypersensitivity signs
Vaccine reactions, though rare, can sometimes manifest as type 1 hypersensitivity responses, characterized by immediate and potentially severe symptoms. Among these, hives (urticaria), swelling (angioedema), difficulty breathing, and hypotension (low blood pressure) are hallmark signs. These symptoms typically occur within minutes to hours after vaccination, triggered by the immune system’s rapid release of histamine and other mediators in response to an allergen, such as a vaccine component. Recognizing these symptoms promptly is critical, as they can escalate quickly and require immediate medical intervention.
Hives and swelling are often the first visible indicators of a type 1 hypersensitivity reaction. Hives appear as raised, itchy welts on the skin, while swelling, particularly around the face, lips, or throat, can be both alarming and dangerous. These symptoms are caused by the dilation of blood vessels and increased permeability of tissues, leading to fluid accumulation. For instance, swelling in the throat can obstruct airways, making breathing difficult. If hives or swelling occur after vaccination, especially if accompanied by respiratory distress, seek medical attention immediately. Antihistamines may provide temporary relief, but professional evaluation is essential to prevent progression.
Difficulty breathing is a red flag that demands urgent action. This symptom can arise from bronchoconstriction (narrowing of the airways) or laryngeal edema (swelling of the voice box), both of which are mediated by histamine release. In severe cases, this can lead to anaphylaxis, a life-threatening condition. Hypotension often accompanies breathing difficulties, as the body’s circulatory system struggles to maintain stability. Symptoms like dizziness, rapid heartbeat, or loss of consciousness may indicate a drop in blood pressure. For individuals with a history of allergies or previous vaccine reactions, carrying an epinephrine auto-injector (e.g., EpiPen) is a practical precaution, as it can buy critical time before emergency care arrives.
While these symptoms are rare, their onset can be rapid and unpredictable. Vaccination sites are equipped to handle such reactions, but preparedness is key. Inform healthcare providers of any known allergies or previous adverse reactions before receiving a vaccine. For children, who may not articulate symptoms clearly, caregivers should watch for signs like restlessness, pallor, or unusual crying. Adults should monitor themselves for tightness in the chest, wheezing, or a sudden drop in blood pressure. In both cases, staying at the vaccination site for 15–30 minutes post-injection is standard practice, allowing for immediate response if symptoms emerge.
In summary, hives, swelling, difficulty breathing, and hypotension are telltale signs of a type 1 hypersensitivity reaction to vaccines. These symptoms require swift recognition and action to prevent severe outcomes. Practical steps include disclosing medical history, observing post-vaccination waiting periods, and having emergency measures like epinephrine readily available. While such reactions are uncommon, understanding and preparedness can make a critical difference in managing them effectively.
DNA Genomes and Vaccines: Unraveling Increased Vulnerability to Immunization
You may want to see also
Explore related products






![]()
Risk Factors: Pre-existing allergies or prior vaccine reactions increase susceptibility to type 1 responses
Vaccine reactions, though rare, can be influenced by individual immune profiles, particularly in those with pre-existing allergies or a history of vaccine responses. Type 1 hypersensitivity, an immediate immune reaction triggered by allergens, shares similarities with certain vaccine responses, raising questions about their connection. For instance, individuals with a history of anaphylaxis to specific allergens, such as eggs or gelatin, may be at higher risk of a type 1-like reaction to vaccines containing these components. The MMR vaccine, for example, is cultivated in gelatin, and the influenza vaccine may contain trace amounts of egg protein, posing potential risks to sensitive individuals.
Identifying High-Risk Groups: People with pre-existing allergies, especially to common vaccine components, should be vigilant. This includes those allergic to eggs, gelatin, latex, or specific antibiotics like neomycin, which are used in vaccine production. A thorough medical history review is crucial before vaccination. For children, parents should inform healthcare providers about any known allergies or previous adverse reactions to vaccines. Adults, particularly those with a history of anaphylaxis, must also disclose their allergy profiles. This proactive approach enables healthcare professionals to select suitable vaccines or administer them under controlled conditions.
The mechanism behind this increased susceptibility lies in the immune system's memory. In type 1 hypersensitivity, the body produces IgE antibodies against specific allergens, leading to rapid release of histamine and other mediators upon re-exposure. Similarly, prior exposure to vaccine components can prime the immune system, potentially resulting in a swift and exaggerated response. This is not a typical reaction but a heightened sensitivity in predisposed individuals. For instance, a person with a severe egg allergy might experience anaphylaxis after receiving an egg-based flu vaccine, a reaction mediated by IgE antibodies.
Mitigating Risks: Healthcare providers can employ strategies to minimize risks. One approach is component avoidance, offering alternative vaccines without the allergen. For egg-allergic individuals, cell-based or recombinant flu vaccines are safer options. Another strategy is graded administration, a process of giving small, incremental doses of the vaccine, monitoring for reactions, and proceeding with the full dose if tolerated. This method has proven effective in allergen immunotherapy and can be adapted for vaccine administration in high-risk cases. Additionally, ensuring immediate access to emergency treatment, such as epinephrine, during vaccination is essential for rapid response to any adverse events.
Understanding these risk factors is crucial for personalized vaccine strategies. While vaccines are generally safe, recognizing and addressing individual susceptibilities can further enhance their safety profile. This tailored approach ensures that the benefits of vaccination are accessible to all, including those with unique immune challenges. By identifying high-risk groups, understanding the immunological mechanisms, and implementing targeted mitigation strategies, healthcare providers can effectively manage and reduce the occurrence of type 1 hypersensitivity-like reactions to vaccines.
Vaccines Against Syphilis: What's Available Now?
You may want to see also
Explore related products






![]()
Vaccine Components: Certain additives (e.g., gelatin, egg proteins) can act as allergens in sensitive individuals
Vaccine formulations often include additives like gelatin, egg proteins, and preservatives to stabilize the active components or enhance immune response. While these substances are generally safe, they can trigger allergic reactions in sensitive individuals. Gelatin, for instance, is a common stabilizer in vaccines such as the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine. For those with gelatin allergy, exposure can lead to symptoms ranging from mild hives to severe anaphylaxis. Similarly, egg proteins, present in influenza and yellow fever vaccines, pose a risk to individuals with egg allergies, though the risk is low and often manageable with precautions.
Understanding the risk factors is crucial for healthcare providers and patients alike. Children, particularly those with a history of allergies, are more susceptible to vaccine-related allergic reactions. For example, the MMR vaccine contains trace amounts of gelatin, and while reactions are rare, they are more likely in children with known gelatin sensitivity. In such cases, healthcare providers may recommend skin testing or administer the vaccine in a controlled setting with immediate access to emergency treatment. Adults with egg allergies can often receive egg-containing vaccines safely, but precautions such as skin testing or graded dosing may be advised for those with severe reactions.
Practical steps can mitigate the risk of allergic reactions to vaccine additives. For egg-allergic individuals, the CDC recommends that the influenza vaccine be administered in a medical setting, such as a hospital, clinic, or health department, where immediate treatment is available. Similarly, for gelatin-allergic patients, healthcare providers should review the vaccine’s excipient list and consider alternatives if available. In cases where no alternative exists, the benefits of vaccination often outweigh the risks, and proceeding with caution is advised. Parents and caregivers should inform healthcare providers of any known allergies before vaccination to ensure appropriate precautions are taken.
Comparing the risks and benefits highlights the importance of individualized care. While additives like gelatin and egg proteins can act as allergens, the incidence of severe reactions is extremely low. For example, studies show that anaphylaxis occurs in approximately 1.3 cases per million doses of the MMR vaccine. In contrast, the diseases prevented by these vaccines—such as measles, which has a fatality rate of 1-3 per 1,000 cases—pose far greater risks. This balance underscores the need for tailored approaches, where potential allergens are identified and managed without compromising the protective benefits of vaccination.
In conclusion, awareness and proactive management are key to addressing vaccine reactions linked to additives. Healthcare providers should remain vigilant, especially when vaccinating individuals with known allergies, and follow guidelines for safe administration. Patients and caregivers must communicate allergy histories clearly and seek medical advice when uncertain. By doing so, the rare risks associated with vaccine components can be minimized, ensuring that the lifesaving benefits of vaccination are accessible to all, even those with sensitivities to specific additives.
Vaccinated and Tested Positive: What Happens After a COVID-19 Breakthrough Infection?
You may want to see also
Explore related products




![]()
Management Strategies: Epinephrine, antihistamines, and monitoring are key to treating type 1 reactions post-vaccination
Vaccine reactions, though rare, can manifest as type 1 hypersensitivity responses, characterized by the rapid release of mediators like histamine and leukotrienes. These reactions, often immediate and potentially life-threatening, demand swift and precise management. The cornerstone of treatment lies in three critical interventions: epinephrine administration, antihistamine use, and vigilant monitoring. Each plays a distinct yet interconnected role in mitigating the severity of the reaction and ensuring patient safety.
Epinephrine stands as the first-line therapy for severe type 1 hypersensitivity reactions, including anaphylaxis post-vaccination. Its mechanism of action involves reversing bronchoconstriction, vasodilation, and hypotension by stimulating alpha- and beta-adrenergic receptors. For adults and children, the recommended dose is 0.3–0.5 mg of 1:1000 epinephrine administered intramuscularly into the lateral thigh. In pediatric patients, the dose is weight-based: 0.01 mg/kg, with a maximum of 0.3 mg. Repeat doses may be necessary every 5–15 minutes if symptoms persist. It’s crucial to position the patient supine to prevent hypotension, and immediate activation of emergency medical services is mandatory, even after epinephrine administration.
Antihistamines, such as diphenhydramine or cetirizine, complement epinephrine by blocking H1 receptors and reducing symptoms like urticaria, angioedema, and pruritus. While not a substitute for epinephrine in severe cases, they provide symptomatic relief and can be administered orally or intravenously. Diphenhydramine dosing is 25–50 mg for adults and 1 mg/kg for children, up to a maximum of 50 mg. However, antihistamines should never delay epinephrine administration in anaphylaxis. Their role is secondary, addressing residual symptoms once the life-threatening aspects are controlled.
Monitoring is the linchpin of effective management, ensuring early detection of symptom progression or recurrence. Vital signs, including blood pressure, heart rate, respiratory rate, and oxygen saturation, must be continuously assessed. Patients should be observed for at least 4–6 hours post-reaction, as biphasic anaphylaxis—a recurrence of symptoms after initial improvement—can occur. In severe cases, hospitalization for extended monitoring may be warranted. Practical tips include keeping the patient in a calm environment, avoiding triggers, and educating caregivers on recognizing early signs of deterioration.
In summary, managing type 1 hypersensitivity reactions post-vaccination requires a structured, evidence-based approach. Epinephrine remains the gold standard for severe reactions, antihistamines provide adjunctive relief, and meticulous monitoring ensures patient stability. By adhering to these strategies, healthcare providers can effectively mitigate risks and improve outcomes in this critical scenario.
Comparing Vaccine Efficacy: Are Some Vaccines Superior to Others?
You may want to see also
Frequently asked questions
Some vaccine reactions, such as immediate allergic responses (e.g., anaphylaxis), can be classified as Type 1 hypersensitivity. These reactions involve IgE antibodies and mast cell activation, leading to rapid symptoms like hives, swelling, or difficulty breathing.
Type 1 hypersensitivity reactions to vaccines are typically caused by an immune response to specific vaccine components, such as proteins, stabilizers, or preservatives. The body produces IgE antibodies against these substances, triggering mast cell release of histamine and other mediators.
Type 1 hypersensitivity reactions to vaccines are rare, occurring in approximately 1 in 1 million doses. Most vaccine-related adverse events are mild and not classified as hypersensitivity reactions. Severe allergic reactions are closely monitored and managed with appropriate medical intervention.