Vaccines and antibodies are distinct but interconnected components of the immune system. Vaccines are biological preparations that stimulate the body's immune response to a specific pathogen, such as a virus or bacterium, by introducing a harmless form of the pathogen or its components. This process primes the immune system to recognize and combat the actual pathogen if encountered in the future. Antibodies, on the other hand, are proteins produced by the immune system in response to the presence of foreign substances, known as antigens. They act as a defense mechanism by binding to these antigens, neutralizing them, or marking them for destruction by other immune cells. While vaccines trigger the production of antibodies as part of the immune response, they are not the same; vaccines are the tools that prepare the body, and antibodies are the resulting weapons used to fight off infections.
| Characteristics | Values |
|---|---|
| Definition | Vaccines are biological preparations that provide active, acquired immunity to particular diseases. Antibodies are proteins produced by the immune system to neutralize pathogens like viruses and bacteria. |
| Origin | Vaccines are externally administered (e.g., injections, oral doses). Antibodies are naturally produced by the body's immune system in response to pathogens or vaccines. |
| Function | Vaccines stimulate the immune system to produce antibodies and memory cells. Antibodies directly bind to and neutralize pathogens. |
| Specificity | Vaccines target specific pathogens or components (e.g., spike proteins in COVID-19 vaccines). Antibodies are highly specific to the pathogen or antigen they were produced against. |
| Duration | Vaccines provide long-term immunity through memory cells. Antibodies may decline over time, but memory cells can rapidly produce them upon re-exposure. |
| Passive vs. Active Immunity | Vaccines induce active immunity. Antibodies can be transferred passively (e.g., monoclonal antibodies or maternal antibodies). |
| Production Time | Vaccines take time (weeks) to stimulate antibody production. Antibodies are produced immediately upon pathogen detection or vaccine administration. |
| Role in Immunity | Vaccines are preventive measures. Antibodies are part of the immune response, whether natural or vaccine-induced. |
| Examples | COVID-19 vaccines (Pfizer, Moderna), flu vaccines. IgG, IgM, IgA antibodies. |
| Side Effects | Vaccines may cause mild side effects (e.g., soreness, fever). Antibodies themselves do not cause side effects but are part of the immune response. |
| Storage | Vaccines require specific storage conditions (e.g., refrigeration). Antibodies are stored naturally in the body. |
| Cost | Vaccines have development and administration costs. Antibody production is a natural bodily function. |
Explore related products






What You'll Learn
![]()
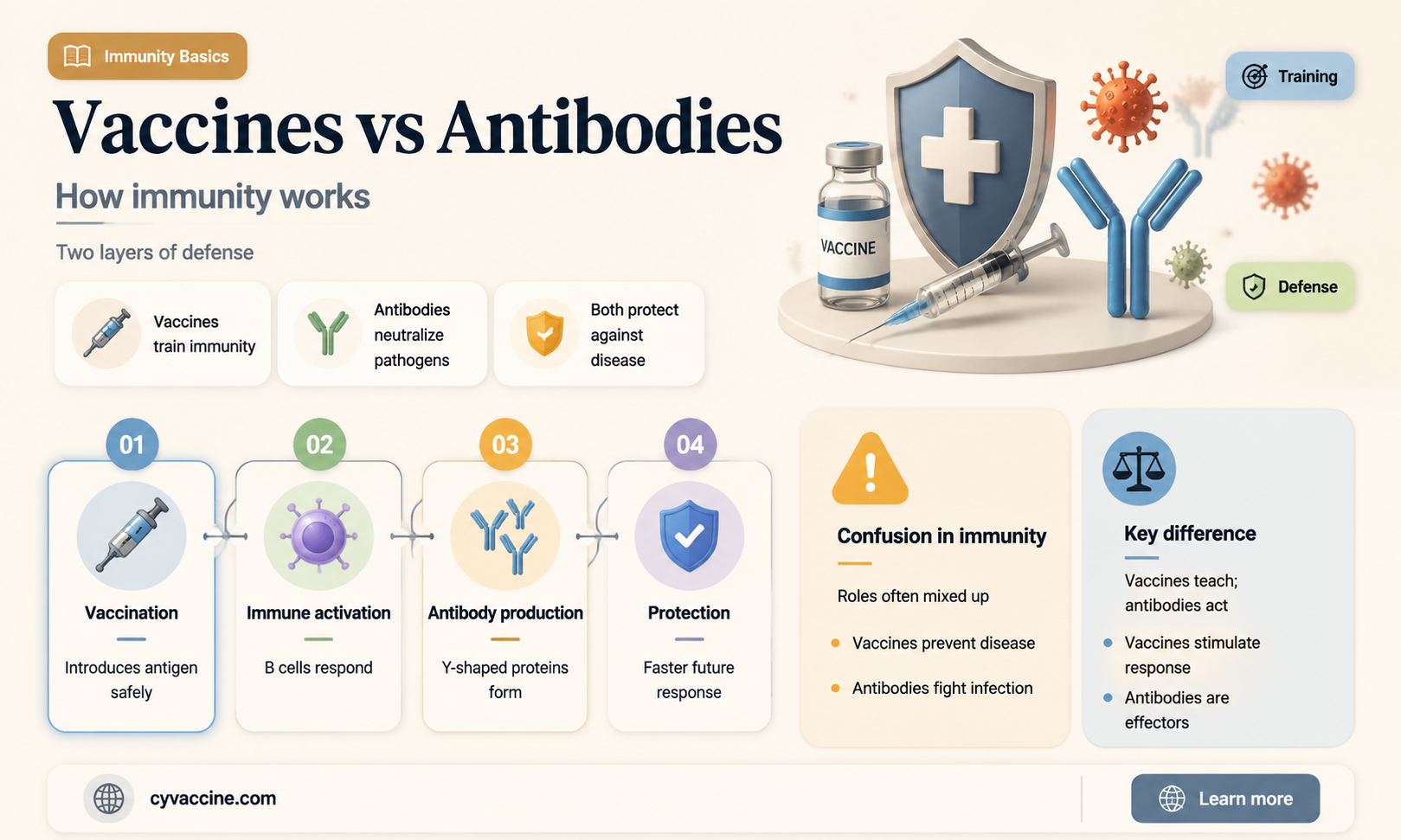
Vaccines vs. Antibodies: Definitions
Vaccines and antibodies are often mentioned in the same breath, yet they serve distinct roles in the immune system. A vaccine is a biological preparation that introduces a weakened or inactivated pathogen, or parts of it, to the body. This exposure trains the immune system to recognize and combat the real threat if encountered later. For instance, the COVID-19 mRNA vaccines deliver genetic material that instructs cells to produce a harmless piece of the virus’s spike protein, triggering an immune response. Antibodies, on the other hand, are proteins produced by the immune system in response to a detected pathogen. They act as targeted weapons, binding to specific antigens on the pathogen to neutralize or mark it for destruction. While vaccines are a preventive measure, antibodies are the body’s active defense once a threat is detected.
Understanding the difference is crucial for informed health decisions. Vaccines are typically administered in doses—for example, the MMR vaccine requires two shots, usually given at 12–15 months and 4–6 years of age. These doses build immunity over time by simulating an infection without causing illness. Antibodies, however, are not administered directly; they are naturally produced by B cells in response to either vaccination or infection. Monoclonal antibody treatments, like those used for severe COVID-19 cases, are an exception, providing lab-created antibodies to supplement the body’s response. This distinction highlights why vaccines are a proactive tool, while antibodies are a reactive mechanism.
From a practical standpoint, vaccines are a cornerstone of public health, preventing diseases like polio, measles, and influenza. They are designed to elicit both immediate and long-term immunity, often requiring boosters to maintain protection. Antibodies, however, have a shorter lifespan and are specific to the pathogen that triggered their production. For example, IgG antibodies, the most common type, can persist for years, while IgM antibodies, produced early in an infection, last only a few weeks. This difference underscores why vaccination schedules are critical—they ensure sustained immunity rather than relying on transient antibody responses.
A persuasive argument for vaccination lies in its ability to reduce the burden on the healthcare system. By preventing infections, vaccines lower the need for treatments that rely on antibodies, whether naturally produced or administered. For instance, widespread flu vaccination reduces hospitalizations, freeing resources for other critical care needs. Conversely, relying solely on natural antibody production through infection risks overwhelming healthcare systems, as seen during the COVID-19 pandemic. This comparison illustrates why vaccines are not just personal health tools but essential components of community well-being.
In summary, vaccines and antibodies are complementary but not interchangeable. Vaccines are a preventive measure that primes the immune system, while antibodies are the immune system’s active response to a threat. Vaccines require careful dosing and scheduling to build lasting immunity, whereas antibodies are produced on demand but are short-lived and specific. By understanding these definitions, individuals can make informed decisions about their health and contribute to broader public health goals.
Can Yeast in Vaccines Be Digested in the Bloodstream?
You may want to see also
Explore related products






![]()
How Vaccines Trigger Antibody Production
Vaccines and antibodies are not the same, but they are intimately connected in the body's defense system. Vaccines are biological preparations that provide active, acquired immunity to particular diseases by training the immune system to recognize and combat pathogens. Antibodies, on the other hand, are proteins produced by the immune system in response to the presence of foreign substances, known as antigens. Understanding how vaccines trigger antibody production is crucial to appreciating their role in disease prevention.
The process begins with the administration of a vaccine, which typically contains a weakened or inactivated form of a pathogen, or specific components of it, such as proteins or sugars. For instance, the influenza vaccine contains inactivated virus particles, while the mRNA COVID-19 vaccines provide genetic instructions to produce a harmless piece of the virus’s spike protein. Upon injection, usually into the muscle (e.g., deltoid muscle for doses of 0.5 mL in adults), these antigens are taken up by antigen-presenting cells (APCs), such as dendritic cells. These cells then migrate to lymph nodes, where they present the antigen to T cells, initiating an immune response.
Once activated, helper T cells release signaling molecules called cytokines, which stimulate B cells to mature into plasma cells. These plasma cells are the antibody factories of the immune system, producing Y-shaped proteins tailored to bind specifically to the antigen introduced by the vaccine. This binding neutralizes the pathogen, preventing it from infecting cells. For example, antibodies generated after a tetanus vaccine can neutralize the tetanus toxin, protecting against lockjaw. The production of antibodies typically peaks around 2–3 weeks after vaccination, depending on the vaccine type and individual immune response.
A critical aspect of this process is the formation of memory B cells, which persist long after the initial immune response has subsided. These cells "remember" the specific antigen and can rapidly produce antibodies upon re-exposure, providing long-term immunity. Booster shots, such as the Tdap vaccine recommended every 10 years for tetanus, diphtheria, and pertussis, reinforce this memory by reactivating memory B cells and enhancing antibody levels. This dual mechanism of immediate antibody production and long-term memory is why vaccines are so effective at preventing diseases.
Practical tips for optimizing antibody production include adhering to recommended vaccine schedules, as spacing doses appropriately (e.g., 3–4 weeks apart for some COVID-19 vaccines) allows for robust immune memory formation. Maintaining a healthy lifestyle—adequate sleep, balanced nutrition, and regular exercise—supports immune function. For older adults or immunocompromised individuals, consulting healthcare providers about additional doses or adjuvanted vaccines (e.g., shingles vaccines with adjuvants for enhanced response) can improve antibody production. Understanding this intricate process empowers individuals to make informed decisions about vaccination, ensuring maximum protection against preventable diseases.
Are Vaccines in Bananas? Unraveling the Myth and Facts
You may want to see also
Explore related products





![]()
Natural vs. Vaccine-Induced Antibodies
Vaccines and natural infections both trigger the production of antibodies, but the pathways and outcomes differ significantly. When you contract a disease naturally, your body responds by generating antibodies as part of a full-scale immune reaction, which can be unpredictable and sometimes severe. For instance, a natural COVID-19 infection prompts the immune system to produce antibodies against multiple viral components, including the spike protein and nucleocapsid protein. However, this process often comes with risks such as long-term health complications or even death, particularly in vulnerable populations like the elderly or immunocompromised. In contrast, vaccines are designed to introduce a controlled, safe version of the pathogen—either a weakened virus, a fragment of it, or its genetic material—to stimulate a targeted immune response. For example, mRNA vaccines like Pfizer-BioNTech and Moderna deliver instructions for cells to produce only the spike protein, focusing the immune system’s efforts on this critical component without exposing the body to the virus’s harmful effects.
Consider the duration and strength of antibody responses when comparing natural infection to vaccination. Natural infections often lead to a broader but variable antibody response, with levels peaking during acute illness and declining over months to years. Studies show that COVID-19 survivors can retain detectable antibodies for up to 12–18 months, though individual responses vary widely based on factors like disease severity and age. Vaccine-induced antibodies, however, are more consistent in their initial response but may wane faster. For instance, two doses of an mRNA COVID-19 vaccine typically produce peak antibody levels within 2–4 weeks, with a gradual decline over 6–12 months, necessitating booster doses to maintain protection. A booster shot administered 6 months after the initial series can increase antibody titers by 10–20-fold, providing robust defense against severe disease and hospitalization.
One critical advantage of vaccine-induced antibodies is their ability to be standardized and optimized for safety and efficacy. Vaccines undergo rigorous testing to determine the ideal dosage and schedule, ensuring a reliable immune response without the risks of natural infection. For example, the Pfizer-BioNTech COVID-19 vaccine is administered in two 30-microgram doses for individuals aged 12 and older, while children aged 5–11 receive a lower 10-microgram dose to balance efficacy and side effects. This precision is absent in natural infections, where the "dose" of the pathogen is uncontrolled and can overwhelm the immune system. Additionally, vaccines often include adjuvants—substances that enhance the immune response—to improve antibody production and longevity. This controlled approach allows vaccines to provide protection comparable to or even exceeding that of natural infection, particularly against severe outcomes.
Practical considerations also favor vaccine-induced antibodies in many scenarios. Vaccination campaigns can be scaled globally, offering protection to populations before they encounter the pathogen. For instance, the measles vaccine has led to a 73% reduction in deaths worldwide since 2000, demonstrating the power of proactive immunization. In contrast, relying on natural infection for immunity would result in widespread morbidity and mortality, especially in regions with limited healthcare resources. Furthermore, vaccines can be updated rapidly to address new variants, as seen with the Omicron-specific COVID-19 boosters. For individuals, staying up-to-date with recommended vaccine schedules—such as annual flu shots or COVID-19 boosters—is a practical way to maintain antibody levels and reduce the risk of infection and transmission.
In conclusion, while both natural infections and vaccines produce antibodies, the latter offers a safer, more controlled, and scalable solution. Vaccine-induced antibodies are tailored for efficacy, minimize health risks, and can be adapted to evolving pathogens. For optimal protection, individuals should follow vaccination guidelines, including booster doses, and avoid relying on natural infection as a means of immunity. This approach not only safeguards personal health but also contributes to community-wide disease prevention.
Comparing RSV Vaccines: Which One Offers Superior Protection?
You may want to see also
Explore related products






![]()
Duration of Vaccine-Generated Immunity
Vaccines and antibodies are not the same, though they are closely related in the context of immunity. Vaccines are biological preparations that stimulate the immune system to recognize and combat pathogens, while antibodies are proteins produced by the immune system in response to these pathogens or vaccines. Understanding the duration of vaccine-generated immunity is crucial for assessing how long protection lasts and when booster doses might be necessary.
The longevity of vaccine-induced immunity varies widely depending on the vaccine type and the pathogen it targets. For instance, the measles, mumps, and rubella (MMR) vaccine typically confers lifelong immunity after two doses, administered at 12–15 months and 4–6 years of age. In contrast, the tetanus vaccine requires booster shots every 10 years to maintain protection. This disparity highlights the importance of understanding the specific immune response each vaccine elicits. Factors such as the pathogen’s ability to mutate (e.g., influenza) or the vaccine’s formulation (live-attenuated vs. inactivated) play a significant role in determining immunity duration.
Analyzing the mechanisms behind vaccine-generated immunity reveals why some protections wane over time. Vaccines work by mimicking an infection, prompting the body to produce memory B and T cells. These cells "remember" the pathogen and can quickly respond if exposed again. However, memory cell populations decline naturally over years, and antibody levels drop accordingly. For example, the COVID-19 mRNA vaccines (Pfizer-BioNTech, Moderna) initially provide robust protection, but studies show antibody levels decrease significantly 6–12 months post-vaccination, particularly in older adults or immunocompromised individuals. This decline underscores the need for booster doses to re-stimulate the immune system.
Practical considerations for maintaining vaccine-generated immunity include adhering to recommended booster schedules and staying informed about updated guidelines. For instance, the annual influenza vaccine accounts for viral mutations, ensuring protection against circulating strains. Similarly, the shingles vaccine (Shingrix) requires two doses, 2–6 months apart, to achieve optimal immunity in adults over 50. Parents should ensure children complete their vaccination series on time, as delays can reduce efficacy. Additionally, lifestyle factors like adequate sleep, nutrition, and stress management can support overall immune function, complementing vaccine-induced protection.
In conclusion, the duration of vaccine-generated immunity is a dynamic and vaccine-specific phenomenon influenced by immunological, pathogen-related, and individual factors. While some vaccines offer decades-long protection, others require periodic boosters to sustain immunity. Understanding these differences empowers individuals to make informed decisions about their health and follow public health recommendations effectively. Regular consultation with healthcare providers ensures personalized guidance tailored to age, health status, and exposure risk.
Vaccine Rollout: Which States Prioritize 65+ for COVID-19 Shots?
You may want to see also
Explore related products






![]()
Antibody Role in Vaccine Efficacy
Vaccines and antibodies are not the same, but their relationship is pivotal to understanding immune protection. Vaccines are biological preparations that stimulate the immune system to recognize and combat pathogens, while antibodies are proteins produced by the immune system to neutralize or eliminate these threats. The efficacy of a vaccine hinges on its ability to induce a robust antibody response, which acts as the body’s first line of defense against infection. Without this antibody production, vaccines would fail to provide the long-term immunity they are designed to deliver.
Consider the COVID-19 mRNA vaccines, which have demonstrated high efficacy in preventing severe disease. These vaccines introduce genetic material that instructs cells to produce a harmless piece of the virus’s spike protein. The immune system responds by generating antibodies specific to this protein. Studies show that individuals with higher antibody titers post-vaccination are significantly less likely to experience symptomatic infection. For instance, a dose of 30 micrograms of the Pfizer-BioNTech vaccine has been shown to elicit a median antibody titer of 1,000 U/mL, offering robust protection for at least six months. This highlights the direct correlation between antibody levels and vaccine efficacy.
However, antibody production is not the sole measure of vaccine success. Some vaccines, like the Bacillus Calmette-Guérin (BCG) vaccine for tuberculosis, rely more on cellular immunity than antibody responses. Yet, for most viral vaccines, antibodies play a critical role in neutralizing pathogens before they can cause infection. For example, the measles vaccine induces antibodies that block the virus from entering host cells, achieving over 95% efficacy with a standard two-dose regimen. This underscores the importance of tailoring vaccine design to maximize the desired immune response, whether antibody-based or otherwise.
Practical considerations also influence antibody-driven vaccine efficacy. Age, underlying health conditions, and nutritional status can affect antibody production. For instance, older adults often mount weaker antibody responses due to immunosenescence, necessitating higher vaccine doses or adjuvants. Similarly, individuals with compromised immune systems may require additional booster shots to achieve protective antibody levels. To optimize vaccine efficacy, healthcare providers should assess patient-specific factors and adjust dosing or schedules accordingly.
In conclusion, while vaccines and antibodies are distinct entities, the latter is a cornerstone of vaccine efficacy, particularly for viral infections. Understanding the mechanisms by which vaccines stimulate antibody production allows for better design, administration, and personalization of immunization strategies. By focusing on this relationship, we can enhance the protective power of vaccines and address gaps in immunity across diverse populations.
Vaccine Protection: Does a Single Shot Work?
You may want to see also
Frequently asked questions
No, vaccines and antibodies are not the same. Vaccines are substances administered to stimulate the immune system to produce antibodies, while antibodies are proteins produced by the immune system to fight off specific pathogens.
Vaccines do not directly provide antibodies. Instead, they train the immune system to recognize and produce antibodies against a specific pathogen when exposed to it in the future.
Antibodies produced in response to vaccines may wane over time, but the immune system retains memory cells that can quickly produce antibodies if the pathogen is encountered again. Some vaccines require booster shots to maintain immunity.