Vaccinations are a cornerstone of public health, serving as a critical tool in disease prevention. When discussing whether vaccinations are a form of primary or secondary prevention, it is essential to understand the distinction between these two categories. Primary prevention involves measures taken to prevent diseases before they occur, such as immunizations that protect individuals from contracting infections in the first place. Secondary prevention, on the other hand, focuses on early detection and treatment of diseases to prevent their progression, such as screening tests for cancer. Vaccinations clearly fall under primary prevention because they aim to prevent the onset of diseases by stimulating the immune system to recognize and combat pathogens before exposure, thereby reducing the risk of infection and its associated complications. This classification highlights the proactive role of vaccines in safeguarding individual and community health.
| Characteristics | Values |
|---|---|
| Prevention Level | Vaccinations are primarily classified as primary prevention. |
| Definition | Primary prevention aims to prevent the onset of disease before it occurs. Vaccines work by stimulating the immune system to recognize and combat pathogens, preventing infection and disease. |
| Mechanism | Vaccines introduce antigens (weakened, dead, or parts of pathogens) to the immune system, triggering the production of antibodies and memory cells, which provide future protection. |
| Examples | MMR (Measles, Mumps, Rubella), Influenza vaccine, Hepatitis B vaccine, COVID-19 vaccines. |
| Target Population | Healthy individuals without the disease or exposure to the pathogen. |
| Outcome | Reduces the incidence of disease in the population by preventing infection. |
| Secondary Prevention Relevance | Vaccines are not considered secondary prevention, as secondary prevention focuses on early detection and treatment of asymptomatic diseases (e.g., cancer screenings). |
| Public Health Impact | Vaccinations have eradicated or significantly reduced the prevalence of diseases like smallpox and polio, demonstrating their effectiveness as primary prevention tools. |
| Cost-Effectiveness | Highly cost-effective by preventing diseases, reducing healthcare costs, and minimizing productivity losses. |
| Global Health Importance | Essential for achieving herd immunity and controlling infectious disease outbreaks worldwide. |
Explore related products






What You'll Learn
- Vaccine Types: Differentiating primary prevention vaccines from secondary prevention vaccines based on their mechanisms
- Disease Prevention: How vaccinations prevent diseases before or after exposure
- Immunity Role: Primary vs. secondary prevention in building or boosting immunity
- Public Health Impact: Vaccines' role in reducing disease spread and severity
- Examples: Highlighting vaccines as primary (e.g., MMR) or secondary prevention (e.g., HPV)
![]()
Vaccine Types: Differentiating primary prevention vaccines from secondary prevention vaccines based on their mechanisms
Vaccines are categorized into primary and secondary prevention types based on their mechanisms and the stage of disease intervention. Primary prevention vaccines act before infection occurs, training the immune system to recognize and neutralize pathogens. Examples include the measles, mumps, and rubella (MMR) vaccine, typically administered in two doses at 12–15 months and 4–6 years of age. These vaccines stimulate the production of antibodies and memory cells, ensuring rapid response to future exposures. In contrast, secondary prevention vaccines target individuals already exposed to a pathogen, aiming to prevent disease progression or severe outcomes. The hepatitis B vaccine, given as a three-dose series over 6 months, serves as both primary and secondary prevention, depending on the timing of administration relative to exposure.
Mechanistically, primary prevention vaccines rely on inducing long-term immunity through active immunization. They often use live-attenuated or inactivated pathogens, subunit proteins, or mRNA technology. For instance, the Pfizer-BioNTech COVID-19 vaccine, a primary prevention tool, delivers mRNA encoding the SARS-CoV-2 spike protein, prompting the body to produce neutralizing antibodies. Secondary prevention vaccines, however, may employ passive immunization, providing pre-formed antibodies or other immunomodulators to immediately combat infection. The rabies vaccine, administered post-exposure in a series of 4–5 doses over 14 days, combines active and passive strategies, including immunoglobulin injections to neutralize the virus while the immune system mounts a response.
A key differentiator lies in the timing and target population. Primary prevention vaccines are administered to healthy individuals, often as part of routine immunization schedules, to prevent infection altogether. Secondary prevention vaccines, such as the herpes zoster vaccine for shingles, are given to individuals at risk of developing severe disease after exposure. This vaccine, recommended for adults over 50, reduces the risk of shingles by 90% when administered as a two-dose series. The distinction highlights the importance of tailoring vaccine strategies to the specific needs of the population and the disease trajectory.
Practical considerations further distinguish these vaccine types. Primary prevention vaccines often require booster doses to maintain immunity, as seen with the tetanus vaccine, administered every 10 years. Secondary prevention vaccines, like the HPV vaccine, may be less effective if given after infection, underscoring the need for timely intervention. Healthcare providers must assess individual risk factors, such as age, occupation, and travel history, to determine the appropriate vaccine type and schedule. For example, healthcare workers may receive annual influenza vaccines as primary prevention, while travelers to endemic areas might need a yellow fever vaccine as both primary and secondary protection, depending on prior exposure.
In summary, differentiating primary and secondary prevention vaccines hinges on their mechanisms, timing, and target populations. Primary prevention vaccines proactively build immunity in healthy individuals, while secondary prevention vaccines intervene post-exposure to mitigate disease severity. Understanding these distinctions enables informed decision-making in vaccine administration, ensuring optimal protection against infectious diseases. By aligning vaccine type with disease stage and individual risk, healthcare systems can maximize the impact of immunization programs.
Are Vaccines Being Tested in Africa? Uncovering the Truth and Myths
You may want to see also
Explore related products






![]()
Disease Prevention: How vaccinations prevent diseases before or after exposure
Vaccinations are a cornerstone of primary prevention, acting before exposure to a pathogen to prevent disease altogether. This proactive approach harnesses the body’s immune system, training it to recognize and combat specific pathogens without the risk of actual infection. For instance, the measles, mumps, and rubella (MMR) vaccine, typically administered in two doses starting at 12–15 months of age, primes the immune system to produce antibodies against these viruses. If exposed later, the immune system responds swiftly, often preventing infection entirely or reducing its severity. This preemptive defense is why vaccines are categorized as primary prevention—they stop diseases before they start, rather than treating or managing them after exposure.
Contrast this with secondary prevention, which focuses on early detection and intervention after exposure but before symptoms appear. While vaccines do not fall into this category, their role can indirectly support secondary prevention efforts. For example, the HPV vaccine, recommended for adolescents aged 11–12, prevents infections that can lead to cervical cancer. If an individual is vaccinated and later exposed to HPV, their immune system neutralizes the virus, preventing persistent infection—a key factor in cancer development. Here, the vaccine’s primary preventive effect reduces the need for secondary interventions like frequent cancer screenings.
A critical distinction lies in the timing and mechanism of action. Primary prevention through vaccination occurs before exposure, creating a shield against potential pathogens. Secondary prevention, on the other hand, kicks in after exposure, aiming to mitigate harm. Consider the influenza vaccine, administered annually to individuals aged 6 months and older. It doesn’t wait for infection to occur; instead, it prepares the immune system to fend off the virus during flu season. This preemptive action is why public health campaigns emphasize vaccination as a first line of defense, not a reactive measure.
Practical implementation of primary prevention via vaccination requires adherence to recommended schedules and dosages. For example, the diphtheria, tetanus, and pertussis (DTaP) vaccine is given in a series of five doses starting at 2 months of age, with boosters later in life. This regimen ensures sustained immunity, preventing these diseases before exposure. Parents and caregivers play a vital role in ensuring children receive vaccines on time, as delays can leave them vulnerable. Similarly, adults must stay current with vaccines like Tdap and shingles vaccines, which protect against pathogens they may encounter later in life.
In summary, vaccinations epitomize primary prevention by preparing the body to resist diseases before exposure occurs. Their ability to confer immunity without infection distinguishes them from secondary prevention strategies, which address post-exposure scenarios. By following vaccination schedules and understanding their mechanisms, individuals and communities can maximize the benefits of this powerful preventive tool. Vaccines don’t just treat disease—they prevent it from taking hold in the first place.
Debunking Myths: False Claims About Combination Vaccines Exposed
You may want to see also
Explore related products






![]()
Immunity Role: Primary vs. secondary prevention in building or boosting immunity
Vaccinations serve as a cornerstone in the realm of preventive healthcare, but their role in building or boosting immunity often blurs the line between primary and secondary prevention. Primary prevention aims to prevent diseases before they occur, while secondary prevention focuses on early detection and intervention to halt disease progression. Vaccines, by design, primarily function as a primary prevention tool by stimulating the immune system to recognize and combat pathogens before exposure. For instance, the measles, mumps, and rubella (MMR) vaccine is administered to children as young as 12 months, providing immunity before potential exposure to these viruses. This proactive approach not only protects individuals but also contributes to herd immunity, reducing disease prevalence in communities.
However, the distinction isn’t always clear-cut. Some vaccines can also play a secondary prevention role in specific contexts. For example, the HPV vaccine is primarily preventive, but it can also act as a secondary measure for individuals already exposed to certain strains of the virus. Similarly, the hepatitis B vaccine, when given post-exposure (e.g., after a needle-stick injury), serves as secondary prevention by preventing infection from taking hold. This dual functionality highlights the adaptability of vaccines in different prevention strategies, depending on timing and risk factors.
Building immunity through vaccination involves a precise interplay of dosage and timing. For children, the CDC recommends a series of vaccines, such as the DTaP (diphtheria, tetanus, and pertussis) vaccine, administered in multiple doses at 2, 4, 6, and 15–18 months, followed by boosters. Adults, too, require periodic boosters, like the Tdap vaccine every 10 years, to maintain immunity. These schedules ensure that the immune system remains primed to respond effectively, whether as primary prevention or to reinforce waning immunity.
Boosting immunity through vaccination also requires consideration of individual factors, such as age, health status, and exposure risk. For older adults, vaccines like the high-dose flu shot or shingles vaccine (Shingrix) are tailored to address age-related immune decline. Pregnant individuals, on the other hand, are advised to receive the Tdap vaccine during each pregnancy to protect newborns from pertussis. These targeted approaches underscore the importance of personalized vaccination strategies in both primary and secondary prevention.
In practice, maximizing the immunity role of vaccines demands a combination of adherence to vaccination schedules, awareness of risk factors, and proactive healthcare engagement. For instance, travelers to regions with high malaria prevalence should receive the malaria vaccine (Mosquirix) as primary prevention, while those already exposed might require additional antimalarial medications as secondary prevention. By understanding the nuanced roles of vaccines, individuals and healthcare providers can optimize immunity-building efforts, ensuring protection at every stage of life.
Las Vegas Vaccination Rates: Tracking COVID-19 Immunization Progress
You may want to see also
Explore related products






![]()
Public Health Impact: Vaccines' role in reducing disease spread and severity
Vaccines stand as a cornerstone of public health, primarily functioning as a primary prevention measure by preventing diseases before they occur. Unlike secondary prevention, which focuses on early detection and treatment of existing conditions, vaccines act proactively, stimulating the immune system to recognize and combat pathogens before infection takes hold. This mechanism not only protects individuals but also disrupts the chain of disease transmission, reducing community spread. For instance, the measles vaccine, administered in two doses starting at 12 months of age, confers 97% immunity, effectively halting outbreaks in populations with high vaccination rates.
Consider the herd immunity effect, a direct consequence of widespread vaccination. When a critical portion of a population is vaccinated—typically 90-95% for highly contagious diseases like measles—the pathogen struggles to find susceptible hosts, protecting even unvaccinated individuals, such as newborns or immunocompromised persons. This phenomenon underscores vaccines’ dual role: individual protection and collective disease suppression. For example, the HPV vaccine, recommended for adolescents aged 11-12, not only prevents cervical cancer but also reduces the transmission of human papillomavirus, a leading cause of genital warts and other cancers.
Beyond preventing infection, vaccines significantly reduce disease severity in breakthrough cases. The COVID-19 vaccines illustrate this point vividly. While no vaccine offers 100% protection against infection, studies show that vaccinated individuals are 10 times less likely to experience severe illness, hospitalization, or death compared to the unvaccinated. This reduction in severity alleviates strain on healthcare systems, ensuring resources are available for other critical needs. Similarly, the annual influenza vaccine, though variable in efficacy (40-60%), consistently lowers the risk of severe complications, particularly in high-risk groups like the elderly and pregnant women.
Practical implementation of vaccine programs requires strategic planning and public engagement. Vaccination schedules, such as the CDC’s recommended timeline for childhood immunizations, must be adhered to for optimal efficacy. For instance, the DTaP vaccine, given in five doses starting at 2 months, provides robust protection against diphtheria, tetanus, and pertussis. However, success hinges on addressing vaccine hesitancy through education and accessible services. Mobile clinics, school-based programs, and reminder systems can improve uptake, particularly in underserved communities.
In conclusion, vaccines’ role in public health extends far beyond individual immunity. As a primary prevention tool, they curb disease spread, foster herd immunity, and mitigate illness severity, creating a healthier, more resilient society. By prioritizing vaccination, we not only protect ourselves but also contribute to a global effort to eradicate preventable diseases.
Vaccination vs. Anti-Vaccination: Understanding the Core Beliefs and Evidence
You may want to see also
Explore related products






![]()
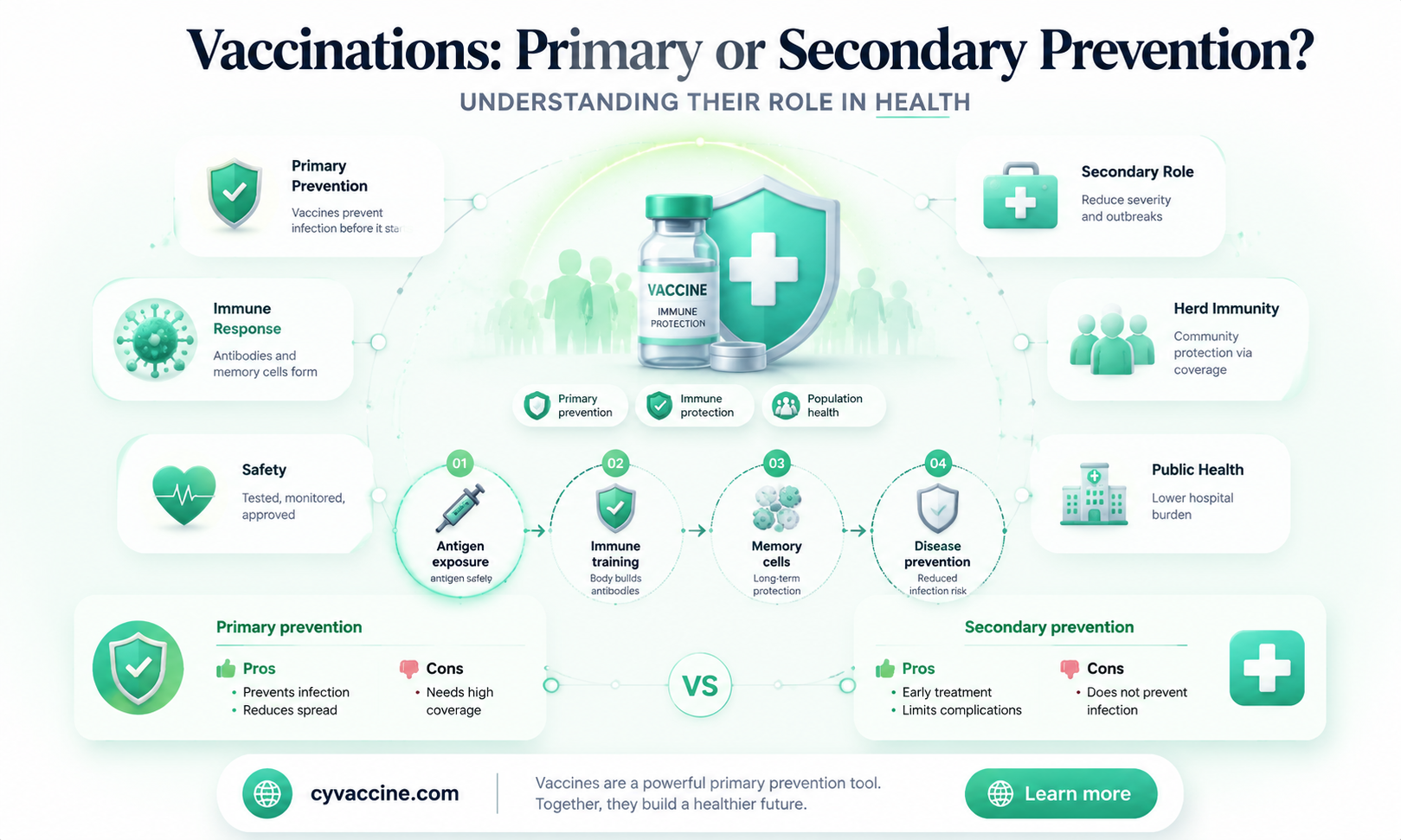
Examples: Highlighting vaccines as primary (e.g., MMR) or secondary prevention (e.g., HPV)
Vaccines like the MMR (Measles, Mumps, Rubella) shot are quintessential examples of primary prevention because they stop diseases before they occur. Administered in two doses—the first at 12–15 months and the second at 4–6 years—this vaccine confers lifelong immunity to 97% of recipients. By preventing measles, a highly contagious virus with complications like pneumonia and encephalitis, it eliminates the risk of infection entirely, aligning with the core goal of primary prevention: avoiding disease onset.
In contrast, the HPV (Human Papillomavirus) vaccine exemplifies secondary prevention when used in certain contexts. While it primarily prevents HPV infection—a precursor to cervical cancer—it is often administered to adolescents aged 11–12, before potential exposure. However, when given to individuals already exposed to HPV, it acts as secondary prevention by halting the progression to precancerous lesions. This dual role highlights how a vaccine’s classification depends on the timing and population targeted, with screening (e.g., Pap smears) complementing its secondary prevention function.
Consider the Hepatitis B vaccine, another example of primary prevention. Given in a three-dose series—typically at birth, 1–2 months, and 6–18 months—it blocks transmission of the virus, which can cause chronic liver disease. For adults at risk (e.g., healthcare workers), accelerated dosing (0, 1, and 6 months) ensures rapid immunity. By preventing initial infection, it eliminates the risk of complications like cirrhosis and liver cancer, firmly placing it in the primary prevention category.
The influenza vaccine illustrates a unique case of annual primary prevention. Unlike MMR or Hepatitis B, its protection wanes yearly due to viral mutations, requiring seasonal administration. Targeting high-risk groups (e.g., elderly, pregnant women) and the general population, it reduces infection rates and hospitalizations. While it doesn’t confer lifelong immunity, its proactive approach—preventing infection before exposure—solidifies its role as primary prevention, despite its recurring nature.
Finally, the tetanus vaccine (part of the DTaP/Tdap series) demonstrates primary prevention with a twist. Administered in childhood (5 doses by age 6) and boosted every 10 years, it neutralizes tetanus toxin, preventing lockjaw from bacterial spores entering wounds. Since tetanus isn’t transmitted person-to-person, the vaccine doesn’t curb spread but instead blocks toxin effects, ensuring the disease never manifests. This proactive blockade underscores its primary prevention status, even in the absence of infectious transmission dynamics.
Live Vaccines: Unlocking Cell-Mediated Immunity's Power and Longevity
You may want to see also
Frequently asked questions
Vaccinations are primarily considered a form of primary prevention because they prevent diseases before they occur by building immunity against specific pathogens.
No, vaccinations are not typically classified as secondary prevention. Secondary prevention focuses on early detection and treatment of a disease, whereas vaccines prevent the disease from occurring in the first place.
Primary prevention, like vaccinations, aims to prevent diseases before they occur. Secondary prevention, on the other hand, involves measures like screening and early intervention to detect and treat diseases in their early stages.
Booster shots are still considered primary prevention because they reinforce immunity to prevent disease, rather than treating or detecting an existing condition.