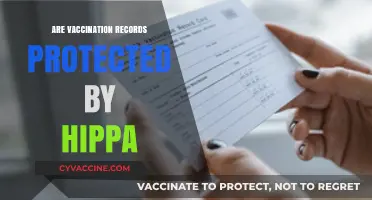
In recent years, concerns have emerged regarding the potential decline of vaccination rates in the United States, raising questions about public health implications and the resurgence of preventable diseases. Despite widespread scientific consensus on the safety and efficacy of vaccines, factors such as misinformation, vaccine hesitancy, and policy changes have contributed to a noticeable shift in immunization trends. Data from various sources, including the Centers for Disease Control and Prevention (CDC), suggest that vaccination coverage for certain diseases has plateaued or even decreased in some populations, particularly among children and adolescents. This trend is alarming, as it threatens to undermine decades of progress in disease prevention and could lead to outbreaks of once-controlled illnesses like measles and whooping cough. Understanding the underlying causes of this decline and addressing them through education, policy interventions, and community engagement is crucial to safeguarding public health and maintaining herd immunity.
| Characteristics | Values |
|---|---|
| Overall Trend (2023) | Mixed; some vaccines show decline, others stable or increasing |
| Childhood Vaccination Rates (2023) | Slight decline in some states; national average remains above 90% for key vaccines (e.g., MMR, DTaP) |
| COVID-19 Vaccination Rates (2023) | Plateaued; ~68% fully vaccinated, ~15% with updated boosters (CDC data) |
| Influenza Vaccination Rates (2022-2023) | ~50% among adults, ~60% among children; slight decline from previous years |
| HPV Vaccination Rates (2023) | ~59% of adolescents fully vaccinated; slower uptake compared to other vaccines |
| Geographic Disparities | Rural areas and Southern states generally lower vaccination rates |
| Socioeconomic Factors | Lower rates among uninsured, low-income, and minority populations |
| Vaccine Hesitancy (2023) | ~20-25% of adults express hesitancy or refusal for some vaccines |
| Political Influence | Partisan divide impacting COVID-19 and childhood vaccine acceptance |
| Misinformation Impact | Increased spread of vaccine misinformation on social media |
| School Exemption Rates | Rising non-medical exemptions in some states (e.g., Oregon, Idaho) |
| Public Health Efforts | Campaigns to combat misinformation and improve access in underserved areas |
Explore related products






What You'll Learn
![]()
Impact of misinformation on vaccine hesitancy
Misinformation has become a potent force in shaping public health decisions, particularly in the context of vaccine hesitancy. A single viral post or video can spread false claims about vaccine safety or efficacy faster than scientific corrections can counter them. For instance, the debunked link between the MMR vaccine and autism, originally published in 1998, continues to influence parental decisions decades later. This persistence highlights how misinformation, once rooted, can outlast its debunking, eroding trust in vaccines and contributing to declining vaccination rates in certain communities.
Consider the COVID-19 pandemic, where misinformation about vaccine side effects, fertility, and microchips fueled hesitancy. False claims that the vaccine could alter DNA or cause severe long-term effects led some individuals to delay or refuse vaccination. Social media platforms, while connecting people, amplified these narratives, creating echo chambers where misinformation thrived. Studies show that exposure to such content correlates with lower vaccination intent, particularly among younger age groups (18–34) who are heavy social media users. This demonstrates how misinformation not only spreads fear but also directly impacts behavior, potentially reversing decades of progress in vaccination coverage.
To combat this, public health campaigns must adopt strategies that address misinformation head-on. One effective approach is to engage trusted community leaders—doctors, teachers, or religious figures—to communicate accurate information. For example, pediatricians can emphasize that childhood vaccines are rigorously tested and spaced to minimize side effects, dispelling myths about "overloading" the immune system. Additionally, fact-checking organizations should collaborate with social media platforms to flag and remove harmful content swiftly. Practical tips for individuals include verifying sources before sharing information and encouraging open dialogue with healthcare providers to address concerns.
The comparative impact of misinformation is stark when examining vaccination rates in regions with high versus low exposure to false narratives. States with lower vaccine uptake often correlate with higher consumption of unverified news sources. Conversely, areas with strong public health infrastructure and proactive communication strategies have maintained higher vaccination rates. This comparison underscores the need for targeted interventions that not only correct misinformation but also build health literacy, empowering individuals to discern credible information from falsehoods.
Ultimately, the fight against vaccine hesitancy requires a multi-faceted approach that acknowledges the power of misinformation. By understanding its mechanisms, leveraging trusted voices, and fostering critical thinking, society can mitigate its impact. The takeaway is clear: addressing misinformation is not just about correcting facts but about rebuilding trust and ensuring that public health decisions are guided by evidence, not fear.
Vaccines' Triumph: Eradicating Deadly Diseases and Saving Lives Globally
You may want to see also
Explore related products






![]()
Regional disparities in vaccination rates
Vaccination rates in the United States are not uniformly declining; rather, they are stagnating or decreasing in specific regions, creating a patchwork of immunity that leaves some communities vulnerable. For instance, rural areas in states like Mississippi and Alabama often report lower vaccination rates compared to urban centers. This disparity is not merely a numbers game—it translates to higher risks of outbreaks for vaccine-preventable diseases like measles and pertussis. Understanding these regional differences requires examining socioeconomic factors, healthcare access, and local attitudes toward vaccines.
Consider the role of healthcare infrastructure in shaping vaccination trends. Urban areas typically have more clinics, pharmacies, and mobile vaccination units, making it easier for residents to access vaccines. In contrast, rural counties may have only one health department serving thousands of square miles, with limited hours and staffing. For example, in Montana, some residents must travel over 100 miles to reach the nearest vaccination site. This logistical barrier disproportionately affects elderly populations and low-income families, who may lack reliable transportation. To address this, policymakers could invest in telehealth solutions or incentivize healthcare providers to operate in underserved areas.
Socioeconomic status also plays a critical role in regional vaccination disparities. Counties with higher poverty rates, such as those in Appalachia, often have lower vaccination coverage. Financial strain can deter individuals from seeking preventive care, even when vaccines are technically free under programs like Vaccines for Children. Additionally, misinformation spreads more easily in communities with limited access to reliable health information. Public health campaigns must tailor their messaging to these regions, using trusted local figures like clergy or teachers to disseminate accurate information. Offering incentives, such as gift cards or discounts, could also encourage vaccination in low-income areas.
Cultural and political beliefs further exacerbate regional differences. In states like Idaho and Wyoming, skepticism toward government mandates has led to lower vaccination rates, particularly for COVID-19. This resistance is often rooted in a broader distrust of institutions, making it difficult for health officials to gain traction. A more effective approach might involve engaging community leaders to foster dialogue rather than imposing top-down solutions. For example, town hall meetings or social media campaigns featuring local success stories could help shift perceptions.
Ultimately, addressing regional disparities in vaccination rates requires a multi-faceted strategy. Policymakers must prioritize equitable healthcare access, especially in rural and low-income areas, while public health officials should design culturally sensitive campaigns that resonate with specific communities. By tackling these challenges head-on, the U.S. can ensure that vaccination rates do not continue to decline in vulnerable regions, protecting both individual health and collective immunity.
Essential Vaccinations for Indiana College Students: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Role of politics in declining rates
The politicization of vaccines has become a significant factor in the decline of vaccination rates in America. What was once a public health issue has now been thrust into the partisan arena, with far-reaching consequences. Republican and Democratic voters increasingly view vaccines through the lens of political identity rather than scientific consensus. This shift is evident in polling data: while 86% of Democrats say vaccines are very important for a child’s health, only 68% of Republicans agree, according to a 2023 Kaiser Family Foundation survey. This partisan gap has widened over the past decade, mirroring the broader polarization in American politics.
Consider the role of political rhetoric in shaping public perception. During the COVID-19 pandemic, vaccine mandates became a flashpoint, with conservative politicians and media outlets framing them as an infringement on personal liberty. This messaging resonated with a segment of the population already skeptical of government intervention, leading to a decline in vaccination rates among certain demographics. For instance, counties that voted for Donald Trump in 2020 had a 10% lower COVID-19 vaccination rate compared to counties that voted for Joe Biden, as reported by the CDC. Such disparities highlight how political narratives can override public health recommendations, even when lives are at stake.
To understand the mechanics of this decline, examine the legislative actions taken at the state level. In recent years, several Republican-led states have introduced bills to expand vaccine exemptions, citing individual freedom as justification. For example, in 2023, Idaho passed a law banning employers from requiring COVID-19 vaccines, while Florida prohibited schools from mandating any vaccines without parental consent. These policies not only undermine herd immunity but also signal to the public that vaccines are optional, rather than essential. Public health officials warn that such measures could lead to outbreaks of preventable diseases like measles, which saw a 30% increase in cases globally in 2022, according to the WHO.
A persuasive argument can be made that addressing this issue requires depoliticizing vaccines. Public health campaigns must focus on rebuilding trust across party lines, emphasizing the nonpartisan nature of science. For instance, partnering with trusted community leaders, regardless of their political affiliation, can help disseminate accurate information. Additionally, policymakers should avoid framing vaccine mandates as a political tool, instead presenting them as a necessary measure to protect public health. Practical steps include funding educational programs that explain vaccine development and efficacy in simple, accessible terms, targeting age groups like parents of young children (0–5 years) who are most likely to seek vaccination advice.
In conclusion, the role of politics in declining vaccination rates is a complex but solvable problem. By acknowledging the influence of partisan rhetoric and taking proactive steps to counteract it, America can reverse this dangerous trend. The key lies in reframing vaccines as a shared responsibility rather than a political battleground, ensuring that public health remains above the fray.
Vaccines: Immune System Friend or Foe?
You may want to see also
Explore related products






![]()
Effect of COVID-19 fatigue on uptake
COVID-19 fatigue has emerged as a silent but potent force eroding vaccination uptake in America. After years of lockdowns, mask mandates, and shifting guidelines, many individuals have grown weary of the pandemic’s demands. This exhaustion manifests in reduced motivation to seek out booster shots or vaccinate younger family members, particularly as the immediate threat of severe illness appears to wane. For instance, data from the CDC shows that while 80% of adults received their initial vaccine series, only 20% of eligible individuals have received the updated bivalent booster as of early 2023. This disparity highlights how fatigue translates into inaction, even when vaccines remain a critical tool for preventing severe outcomes.
To combat this trend, public health campaigns must pivot from fear-based messaging to practical, empathetic strategies. Instead of emphasizing dire statistics, focus on tangible benefits: fewer missed workdays, reduced healthcare costs, and the ability to safely engage in social activities. For parents hesitant to vaccinate children aged 6 months to 5 years, provide clear, age-specific dosage information—such as the lower 3-microgram dose for Pfizer’s pediatric vaccine compared to the 30-microgram adult dose. Pairing this with testimonials from trusted community figures can bridge the gap between fatigue and action.
A comparative analysis reveals that regions with higher vaccination rates often have localized, culturally tailored initiatives. For example, mobile clinics in rural areas or pop-up sites at community centers have proven effective in reaching populations overwhelmed by the logistics of scheduling appointments. Conversely, areas relying solely on broad, national campaigns have seen stagnation or decline in uptake. This suggests that addressing fatigue requires meeting people where they are—both physically and emotionally—rather than expecting them to re-engage with a system that feels increasingly distant.
Finally, a persuasive argument must be made for the long-term value of vaccination in a post-peak pandemic world. Fatigue often stems from the perception that COVID-19 is now just another seasonal illness, but this overlooks the cumulative risk of repeated infections. Studies show that even mild cases can lead to long-term health issues, such as cardiovascular complications or reduced lung function. Framing vaccination as a proactive step toward preserving overall health—not just preventing hospitalization—can resonate with those who feel desensitized to the pandemic’s urgency. By reframing the narrative, public health efforts can transform fatigue into a renewed commitment to protection.
Navigating the Vaccination Question: A Guide to Responding Confidently
You may want to see also
Explore related products






![]()
Trends in childhood vs. adult vaccinations
Childhood vaccination rates in the United States have historically been higher than adult rates, largely due to the structured immunization schedules tied to school entry requirements. For instance, the CDC reports that approximately 90% of children aged 19–35 months receive recommended doses of the measles, mumps, and rubella (MMR) vaccine, compared to only 30% of adults aged 19–64 who are up-to-date on tetanus, diphtheria, and pertussis (Tdap) boosters. This disparity highlights a critical gap in adult immunization, where vaccines like Tdap, shingles (Shingrix), and pneumococcal (PCV15/PPSV23) are often overlooked despite their proven efficacy in preventing severe illness. Unlike childhood vaccines, adult immunizations lack mandatory reminders or systemic tracking, leaving adherence largely to individual initiative or healthcare provider prompts.
The decline in adult vaccination rates is further exacerbated by misinformation and logistical barriers. While childhood vaccines are typically administered during pediatric visits, adults must actively seek out vaccines, often during sporadic primary care appointments. For example, only 45% of adults aged 50 and older have received the shingles vaccine, despite its 90% effectiveness in preventing a painful condition that affects 1 in 3 Americans. In contrast, childhood vaccines benefit from school-based mandates and public health campaigns, such as the annual push for flu shots in pediatric settings, which achieve coverage rates of 60–70% for influenza among children, compared to 40–50% in adults.
A comparative analysis reveals that adult vaccination hesitancy is fueled by different factors than childhood vaccine skepticism. While parental concerns about childhood vaccines often center on safety myths (e.g., debunked links to autism), adult hesitancy stems from perceived low risk of disease and mistrust of pharmaceutical incentives. For instance, only 27% of adults receive the annual flu vaccine, even though influenza causes 12,000–52,000 deaths annually in the U.S. In contrast, childhood flu vaccination rates are higher due to parental awareness campaigns and school-based clinics, demonstrating the power of structured systems in driving compliance.
To bridge this gap, healthcare providers should adopt proactive strategies tailored to adult populations. For example, pharmacists can administer vaccines like Tdap and shingles during prescription pickups, leveraging their accessibility. Employers can host workplace vaccination clinics, as seen in successful flu shot drives that increase adult participation by 20–30%. Additionally, integrating adult vaccine reminders into electronic health records (EHRs) and offering standing orders in clinics can streamline access. For instance, a 2021 study found that EHR-based prompts increased adult Tdap uptake by 15% within six months. By emulating the structured approach of childhood immunization programs, adult vaccination rates could significantly improve, reducing preventable diseases and healthcare costs.
Vaccination Status: What Can You Ask in an Interview?
You may want to see also
Frequently asked questions
Vaccination rates in America vary by demographic, age group, and vaccine type. While some specific vaccines, such as the COVID-19 vaccine, have seen declining uptake in certain populations, overall childhood vaccination rates for diseases like measles, mumps, and rubella (MMR) have remained relatively stable. However, there are concerns about localized declines in vaccination rates in some communities.
Factors contributing to declining vaccination rates include vaccine hesitancy fueled by misinformation, lack of access to healthcare services, political polarization around vaccines, and the rise of anti-vaccine movements. Additionally, the COVID-19 pandemic disrupted routine vaccination schedules for many, leading to temporary declines in some areas.
Declining vaccination rates in certain areas have led to outbreaks of preventable diseases like measles and pertussis. This poses risks not only to unvaccinated individuals but also to those who cannot receive vaccines due to medical reasons (herd immunity). Public health officials warn that continued declines could reverse decades of progress in disease prevention.