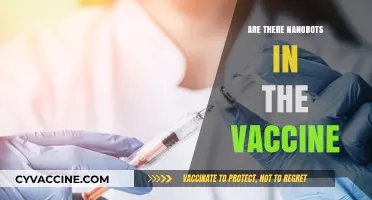
The question of whether there are medical exceptions for vaccines is a critical aspect of public health discussions, as it balances the benefits of immunization with individual health considerations. Medical exceptions, also known as contraindications, are specific health conditions or circumstances that may make vaccination unsafe or inadvisable for certain individuals. These exceptions are typically determined by healthcare professionals and can include severe allergies to vaccine components, compromised immune systems due to conditions like HIV or cancer treatments, or a history of severe adverse reactions to previous vaccinations. While vaccines are generally safe and effective for the majority of the population, recognizing and respecting these exceptions is essential to ensure patient safety and maintain trust in vaccination programs. Understanding these exceptions also highlights the importance of personalized medical advice and the need for robust public health policies that accommodate diverse health needs.
| Characteristics | Values |
|---|---|
| Medical Exemptions Availability | Yes, medical exemptions for vaccines are available in many countries. |
| Qualifying Conditions | Severe allergic reactions (e.g., anaphylaxis), immunodeficiency disorders, specific chronic illnesses, or other documented medical contraindications. |
| Documentation Required | Written statement from a licensed healthcare provider detailing the medical reason for exemption. |
| Approval Authority | Varies by country/region; often requires approval from public health authorities or schools. |
| Vaccines Covered | Exemptions typically apply to specific vaccines (e.g., MMR, COVID-19) based on individual medical history. |
| Temporary vs. Permanent | Exemptions can be temporary (e.g., during illness) or permanent (e.g., chronic conditions). |
| Legal Recognition | Legally recognized in many jurisdictions, but policies differ (e.g., U.S. states, EU countries). |
| Impact on Public Health | Exemptions are granted sparingly to balance individual health needs with community immunity. |
| Recent Trends | Increased scrutiny during outbreaks (e.g., COVID-19) to prevent misuse of exemptions. |
| Examples of Conditions | Severe immunodeficiency, history of thrombosis with thrombocytopenia syndrome (TTS), or active chemotherapy treatment. |
Explore related products






What You'll Learn
![]()
Allergic Reactions to Vaccine Components
Vaccines, while generally safe, can trigger allergic reactions in a small subset of individuals due to specific components like gelatin, egg protein, or preservatives. These reactions range from mild, such as hives or swelling, to severe, like anaphylaxis, which requires immediate medical attention. For instance, the measles-mumps-rubella (MMR) vaccine contains trace amounts of gelatin, a known allergen for some. Similarly, influenza vaccines are often cultivated in chicken eggs, posing a risk to those with egg allergies. Identifying these components beforehand is crucial for healthcare providers to assess risk and determine if vaccination is safe or if an alternative should be considered.
For individuals with known allergies to vaccine components, a graded challenge may be recommended under medical supervision. This involves administering the vaccine in small, incremental doses to monitor for reactions. For example, someone with an egg allergy might receive the flu vaccine in three divided doses over an hour, starting with 10% of the full dose. If no reaction occurs, the remaining vaccine is given. This method has proven effective in safely vaccinating those with mild to moderate egg allergies, particularly in adults and older children. However, this approach is not suitable for severe allergies or a history of anaphylaxis, where vaccination risks may outweigh benefits.
Healthcare providers must carefully review a patient’s medical history before administering vaccines, especially for those with a history of allergic reactions. The Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP) provide guidelines for managing such cases. For instance, the mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna) do not contain egg or gelatin, making them safer options for individuals with these allergies. Similarly, the recombinant flu vaccine (Flublok) is egg-free and recommended for those with severe egg allergies. These alternatives highlight the importance of personalized vaccine selection based on individual risk factors.
Practical tips for patients include carrying an updated list of known allergies and discussing them with healthcare providers before vaccination. Wearing a medical alert bracelet can also be lifesaving in emergencies. For parents, keeping a detailed record of a child’s allergic reactions and sharing it with pediatricians ensures informed decision-making. In cases of uncertainty, allergy testing may be conducted to confirm sensitivities to specific vaccine components. While rare, allergic reactions underscore the need for vigilance and tailored approaches in vaccination programs to ensure safety without compromising immunity.
Safeguarding Kids: Natural Strategies to Prevent Infectious Diseases
You may want to see also
Explore related products




![]()
Immunocompromised Individuals and Vaccine Safety
Immunocompromised individuals face unique challenges when it comes to vaccine safety. Their weakened immune systems, often due to conditions like HIV/AIDS, cancer treatments, organ transplants, or autoimmune diseases, can limit their ability to mount a robust response to vaccines. This raises critical questions about the efficacy and safety of standard immunization protocols for this population. While vaccines are generally safe, certain live-attenuated vaccines, such as MMR (measles, mumps, rubella) or varicella (chickenpox), pose risks of infection in immunocompromised patients. For instance, the varicella vaccine contains a weakened but live virus, which could potentially cause disease in someone with severely impaired immunity.
To navigate these risks, healthcare providers must carefully assess the individual’s degree of immunosuppression and the specific vaccine in question. For example, inactivated vaccines like the flu shot (IIV) or COVID-19 mRNA vaccines (Pfizer-BioNTech, Moderna) are generally considered safe for immunocompromised individuals because they do not contain live viruses. However, the immune response may be suboptimal, necessitating additional doses or closer monitoring. For instance, the CDC recommends a third dose of mRNA COVID-19 vaccines for moderately to severely immunocompromised individuals aged 5 and older, administered 28 days after the second dose.
Practical tips for immunocompromised individuals include maintaining open communication with healthcare providers to determine the safest vaccination schedule. Household members and close contacts should also be up-to-date on their vaccinations to create a protective "cocoon" around the immunocompromised person. For example, ensuring that family members receive the annual flu vaccine reduces the risk of transmission to a vulnerable individual. Additionally, immunocompromised patients should avoid live vaccines unless explicitly approved by their physician, and they should be cautious during disease outbreaks, taking extra precautions like masking and social distancing.
Comparatively, the approach to vaccinating immunocompromised individuals differs significantly from that of the general population. While healthy individuals typically follow standard dosing schedules, immunocompromised patients may require tailored regimens, such as higher doses or more frequent boosters. For example, individuals on chronic dialysis or with advanced HIV may need additional doses of the pneumococcal vaccine (PCV13 and PPSV23) to ensure adequate protection. This highlights the importance of personalized medicine in vaccinology, where one-size-fits-all strategies fall short for this vulnerable group.
In conclusion, ensuring vaccine safety for immunocompromised individuals requires a nuanced understanding of their immune status, the type of vaccine, and potential risks. By adopting a tailored approach, healthcare providers can maximize protection while minimizing harm. Patients and caregivers must stay informed, follow expert guidelines, and prioritize preventive measures to safeguard health in this high-risk population.
Add Your Vaccine Certificate to Health App: A Simple Guide
You may want to see also
Explore related products





![]()
Chronic Illnesses Affecting Vaccination Eligibility
Certain chronic illnesses can significantly impact an individual’s eligibility for vaccination, requiring careful consideration by healthcare providers. Conditions such as primary immunodeficiency disorders, where the immune system is compromised, often necessitate tailored vaccination plans. For example, patients with severe combined immunodeficiency (SCID) should avoid live-attenuated vaccines like MMR (measles, mumps, rubella) or varicella, as these can cause severe, even life-threatening, infections in immunocompromised individuals. Instead, inactivated vaccines, such as the injectable polio vaccine (IPV) or hepatitis B vaccine, are generally safe and recommended. Always consult an immunologist or primary care physician to determine the safest course of action for these patients.
Autoimmune diseases, such as rheumatoid arthritis or systemic lupus erythematosus (SLE), present another layer of complexity. While many vaccines are still safe for these patients, those on immunosuppressive therapies like high-dose corticosteroids or biologics (e.g., rituximab) may have a reduced immune response to vaccines. For instance, the CDC advises that patients on B-cell depleting therapies delay vaccination until at least 6 months after treatment completion, if possible, to ensure better immune response. In cases where vaccination cannot be delayed, providers may recommend additional doses or alternative schedules to maximize protection. Practical tip: Keep a detailed record of medications and treatments to share with your healthcare provider during vaccine consultations.
Chronic liver or kidney disease also affects vaccination eligibility, particularly for vaccines that require adjuvants or specific dosage adjustments. Patients with end-stage renal disease (ESRD), for example, often have weakened immune responses and may require higher doses or more frequent boosters of certain vaccines, such as hepatitis B. Similarly, individuals with chronic liver disease, especially cirrhosis, may need prioritized access to vaccines like hepatitis A and pneumococcal vaccines due to their increased risk of infection-related complications. Dosage adjustments should always be made under medical supervision, as over-vaccination can pose risks in these populations.
Finally, neurological disorders like epilepsy or multiple sclerosis (MS) generally do not contraindicate vaccination but require monitoring for potential side effects. For instance, fever, a common vaccine reaction, can lower the seizure threshold in epileptic patients, necessitating pre-emptive use of antipyretics like acetaminophen. Patients with MS, particularly those on disease-modifying therapies, should receive inactivated vaccines but avoid live vaccines unless specifically recommended by their neurologist. Comparative analysis shows that while chronic illnesses often complicate vaccination, individualized approaches can ensure both safety and efficacy, highlighting the importance of patient-specific care plans.
The Pertussis Vaccine: What's in a Name?
You may want to see also
Explore related products




![]()
Pregnancy and Vaccine Recommendations
Pregnancy significantly alters a woman's immune system, making her more susceptible to severe complications from certain vaccine-preventable diseases. This vulnerability extends to the developing fetus, which can be adversely affected by maternal infections. For instance, influenza during pregnancy increases the risk of preterm labor, low birth weight, and even fetal death. Similarly, rubella infection in early pregnancy can lead to congenital rubella syndrome, causing severe birth defects. These risks underscore the critical importance of vaccination during pregnancy, not only to protect the mother but also to safeguard the health of the unborn child.
The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) provide clear guidelines for vaccinating pregnant women. The flu vaccine, for example, is recommended for all pregnant women, regardless of trimester. This inactivated vaccine has been extensively studied and proven safe for both mother and fetus. It not only reduces the risk of influenza in the mother but also provides passive immunity to the newborn, protecting the infant during the first few months of life when they are too young to be vaccinated. Similarly, the Tdap vaccine (tetanus, diphtheria, and pertussis) is recommended during the third trimester of each pregnancy to protect the newborn from whooping cough, a potentially life-threatening illness in infants.
However, not all vaccines are advisable during pregnancy. Live attenuated vaccines, such as the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine, are generally contraindicated. These vaccines carry a theoretical risk of harming the developing fetus, although no definitive evidence of harm has been documented. Women who require these vaccines should be counseled to avoid pregnancy for at least four weeks after vaccination. This precautionary approach ensures the safety of both the mother and the fetus while addressing the need for immunization.
Practical considerations also play a role in vaccine recommendations during pregnancy. Healthcare providers should assess a woman’s individual risk factors, such as her health status, occupational exposure, and travel plans, to determine the most appropriate vaccination schedule. For example, a pregnant woman traveling to a region with a high incidence of yellow fever may need to weigh the risks and benefits of vaccination, as the yellow fever vaccine is live attenuated but may be necessary in certain circumstances. Clear communication between the healthcare provider and the patient is essential to make informed decisions.
In conclusion, pregnancy-specific vaccine recommendations balance the need to protect both mother and child against serious infections while minimizing potential risks. By adhering to evidence-based guidelines, healthcare providers can ensure that pregnant women receive the necessary vaccinations at the appropriate times. Pregnant women should also be encouraged to discuss their vaccination status with their healthcare provider early in pregnancy to address any concerns and develop a personalized immunization plan. This proactive approach can significantly reduce the burden of vaccine-preventable diseases during pregnancy and in the postpartum period.
Writing a Medical Exemption Letter for Vaccines: A Step-by-Step Guide
You may want to see also
Explore related products





![]()
Temporary Medical Conditions Delaying Vaccination
Certain acute illnesses and temporary health conditions can warrant a delay in vaccination, but not all sicknesses qualify. For instance, a mild cough or low-grade fever (below 101°F) typically aren’t reasons to postpone immunizations. However, moderate to severe acute illnesses, particularly those with fever above 101°F, require a pause. The rationale is straightforward: during such episodes, the immune system is already taxed, and introducing a vaccine could complicate recovery or obscure adverse reactions. Clinicians often recommend waiting until the individual is fully recovered, usually 2–4 weeks, before proceeding with vaccination.
Consider a child with a confirmed case of chickenpox. The varicella-zoster virus not only causes discomfort but also temporarily weakens the immune system. Administering a vaccine during this period could reduce its efficacy or overburden the body. Similarly, adults with active infections like pneumonia or bronchitis should delay vaccines until the infection clears. For those on high-dose corticosteroids (e.g., prednisone ≥20 mg/day for adults) or other immunosuppressive therapies, vaccination is generally postponed until treatment concludes or doses taper down, as these medications can interfere with immune response.
Pregnancy introduces another layer of complexity. While some vaccines (like Tdap) are recommended during pregnancy, others, such as live-attenuated vaccines (MMR, varicella), are contraindicated. Postpartum, however, temporary conditions like mastitis or postpartum fever may delay certain vaccines until the mother’s health stabilizes. Breastfeeding itself is not a contraindication, but acute illnesses during this period follow the same delay guidelines as non-lactating individuals.
Practical tips for navigating these delays include maintaining open communication with healthcare providers. Document the onset and duration of the acute illness, and note any medications being taken. For children, parents should track symptoms and recovery timelines to provide accurate information during follow-up appointments. If a vaccine series is interrupted, most guidelines allow for resumption at the next scheduled dose without restarting the series, though this varies by vaccine. Always consult a healthcare professional for personalized advice, as exceptions and nuances exist based on individual health profiles.
In summary, temporary medical conditions like acute infections, high fevers, or immunosuppressive treatments can delay vaccination, but the decision requires careful assessment. Mild illnesses rarely justify postponement, while moderate to severe cases demand a waiting period. Understanding these distinctions ensures vaccines are administered safely and effectively, balancing immediate health needs with long-term immunity goals.
Efficient Vaccine Delivery Systems in Nursing Homes: Ensuring Resident Safety
You may want to see also
Frequently asked questions
Yes, medical exceptions for vaccines exist for individuals with specific health conditions that could make vaccination unsafe. These include severe allergic reactions to vaccine components, certain immunodeficiencies, or being severely ill at the time of vaccination.
A qualified healthcare provider, such as a doctor or immunologist, determines if an individual qualifies for a medical exception based on their medical history, current health status, and potential risks associated with vaccination.
Conditions that may qualify include severe allergies to vaccine ingredients (e.g., gelatin, eggs, or preservatives), active untreated cancer, HIV/AIDS, or other immunocompromising conditions. Pregnant individuals or those with a history of severe adverse reactions to vaccines may also be considered.









![Personal Exemptions / Mildred McFall / A Pénz Bolondit (1989) / ENGLISH & Hungarian Language with Romanian Subtitles [European DVD Region 2 PAL]](https://m.media-amazon.com/images/I/71Y3SBUrBIL._AC_UL320_.jpg)