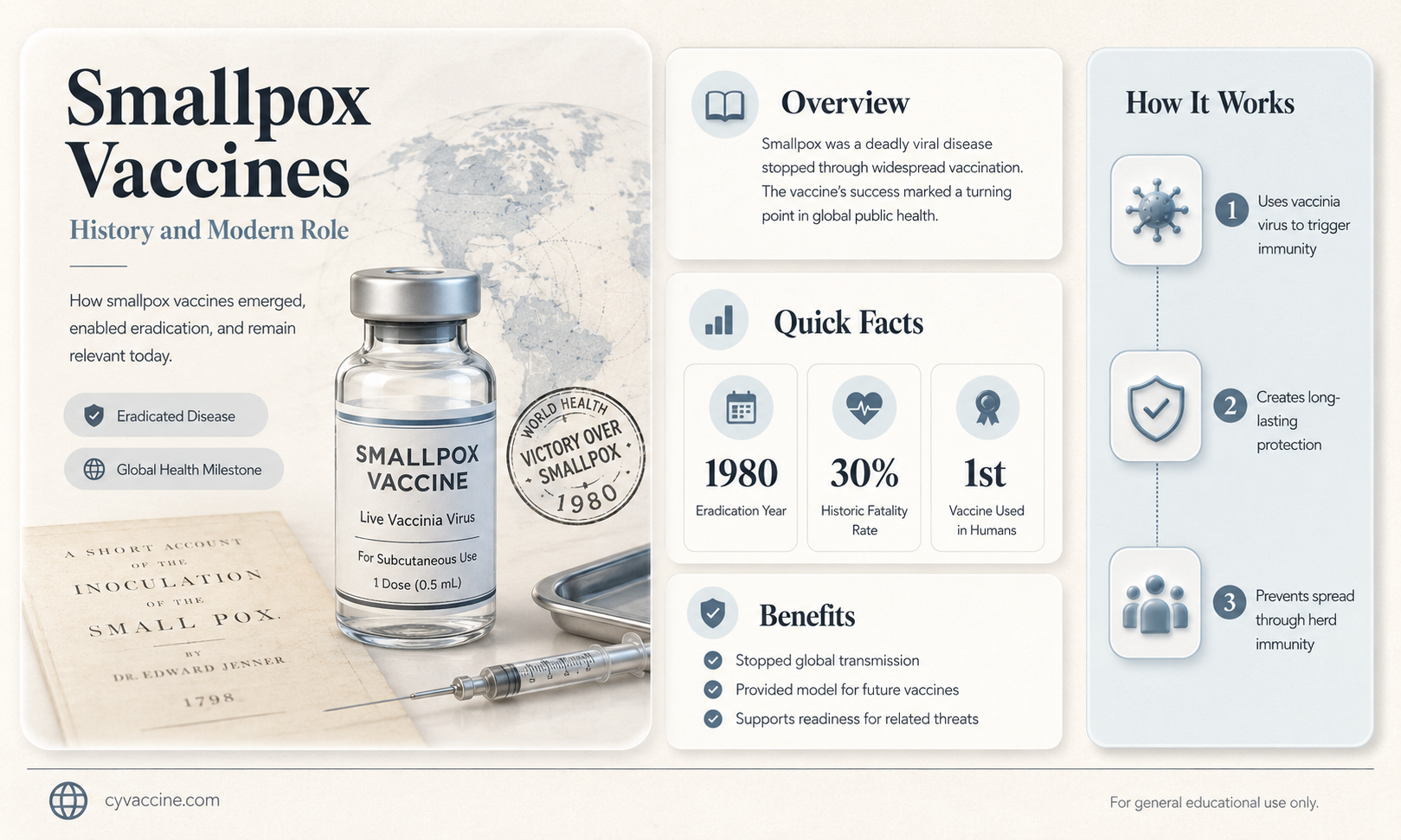
Smallpox, a devastating disease caused by the variola virus, was eradicated globally through a concerted vaccination campaign led by the World Health Organization (WHO) in the 20th century. The last known natural case occurred in 1977, and the disease was officially declared eradicated in 1980. While routine smallpox vaccination is no longer necessary for the general public, vaccines still exist and are stored in secure locations for emergency use, such as in the event of a bioterrorism threat. The original smallpox vaccine, developed by Edward Jenner in 1796, used the vaccinia virus, a related but less harmful virus. Modern smallpox vaccines, like ACAM2000, are derived from similar principles and remain a critical component of global preparedness against potential reemergence of the disease.
| Characteristics | Values |
|---|---|
| Vaccine Availability | Yes, smallpox vaccines exist. |
| Vaccine Types | First-generation (e.g., Dryvax), Second-generation (e.g., ACAM2000), Third-generation (e.g., MVA-BN, LC16m8) |
| Current Use | Not routinely administered due to smallpox eradication in 1980. Stockpiled for emergency use (e.g., bioterrorism). |
| Efficacy | Highly effective in preventing smallpox; estimated 95% protection. |
| Administration | Typically via scarification (pricking the skin) with a bifurcated needle. |
| Side Effects | Common: localized skin reactions, fever, headache. Rare: serious complications like progressive vaccinia or eczema vaccinatum. |
| Contraindications | Immunocompromised individuals, pregnant women, people with certain skin conditions (e.g., eczema). |
| Storage | Requires refrigeration (2–8°C) for stability. |
| Global Eradication | Smallpox was declared eradicated by WHO in 1980, thanks to vaccination campaigns. |
| Current Stockpiles | Held by WHO and select countries for emergency preparedness. |
| Research and Development | Ongoing research on safer, third-generation vaccines for potential future threats. |
Explore related products






What You'll Learn
- Historical smallpox vaccines development and their global eradication impact
- Modern smallpox vaccine availability and storage requirements for emergencies
- Smallpox vaccine effectiveness against related orthopoxviruses like monkeypox
- Side effects and risks associated with smallpox vaccination
- Global stockpiles of smallpox vaccines for potential bioterrorism threats
![]()
Historical smallpox vaccines development and their global eradication impact
Smallpox, a disease caused by the variola virus, has plagued humanity for millennia, leaving behind a trail of death and disfigurement. The development of smallpox vaccines marks one of the most significant triumphs in medical history, culminating in the disease's global eradication in 1980. The story begins in the late 18th century with Edward Jenner's groundbreaking observation that milkmaids who contracted cowpox, a milder disease, were subsequently immune to smallpox. This led to the creation of the first smallpox vaccine in 1796, using material from cowpox lesions. Jenner's method, though rudimentary by today's standards, laid the foundation for modern vaccination. The vaccine was administered by scratching the skin, introducing a small amount of cowpox virus to induce immunity. This technique, known as arm-to-arm vaccination, was widely adopted but carried risks of transmitting other diseases.
The 19th and early 20th centuries saw significant advancements in vaccine production and distribution. In 1880, Louis Pasteur developed methods to produce vaccines on a larger scale, improving consistency and safety. By the mid-20th century, the World Health Organization (WHO) launched a global smallpox eradication campaign, utilizing a freeze-dried vaccine that could be easily transported and stored. This vaccine, administered via a bifurcated needle, required only one dose to confer immunity in most individuals. The needle was dipped into the vaccine powder, and the skin was pricked 15 times in a small area, typically the upper arm. This method ensured a robust immune response while minimizing the amount of vaccine needed. Mass vaccination campaigns, coupled with surveillance and containment strategies, proved highly effective in interrupting the virus's transmission.
The impact of smallpox vaccines on global health cannot be overstated. Before eradication efforts, smallpox killed an estimated 300 million people in the 20th century alone, with a mortality rate of up to 30%. The disease disproportionately affected children and young adults, leaving survivors with permanent scars or blindness. The eradication of smallpox not only saved countless lives but also demonstrated the power of international collaboration in public health. The success of the smallpox campaign inspired similar efforts against other vaccine-preventable diseases, such as polio and measles. Economically, the eradication of smallpox has saved billions of dollars annually in healthcare costs and lost productivity.
Despite the triumph of smallpox eradication, the legacy of its vaccines continues to influence modern medicine. The bifurcated needle, developed specifically for smallpox vaccination, remains a standard tool in immunization programs worldwide. Additionally, the smallpox vaccine has been studied for its potential use against other orthopoxviruses, such as monkeypox, which has emerged as a growing concern in recent years. However, the cessation of routine smallpox vaccination after 1980 has left younger generations without immunity, raising concerns about the potential reintroduction of the virus, whether through natural means or bioterrorism. Stockpiles of smallpox vaccine are maintained by governments and international organizations as a precautionary measure, though their use is strictly regulated.
In conclusion, the development and global deployment of smallpox vaccines represent a monumental achievement in human history. From Jenner's pioneering work to the WHO's eradication campaign, these efforts have saved millions of lives and transformed public health strategies. The lessons learned from smallpox eradication remain relevant today, offering a blueprint for tackling other infectious diseases. As we face new challenges, such as emerging viruses and vaccine hesitancy, the story of smallpox vaccines serves as a powerful reminder of what can be achieved through scientific innovation, global cooperation, and unwavering commitment to public health.
Discovering Russia's COVID-19 Vaccine: What's the Name and Its Impact
You may want to see also
Explore related products






![]()
Modern smallpox vaccine availability and storage requirements for emergencies
Smallpox, a disease eradicated in 1980, still looms in the collective memory as a devastating pandemic. While the virus no longer circulates naturally, concerns about bioterrorism and accidental release have spurred the development and stockpiling of modern smallpox vaccines. These vaccines, primarily the ACAM2000 and Imvamune (also known as Imvanex or Jynneos), are stored in strategic reserves worldwide to ensure rapid deployment in case of an emergency.
Storage requirements for these vaccines are stringent to maintain efficacy. ACAM2000, a live vaccinia virus vaccine, must be stored between -15°C and -25°C (-5°F and -13°F) in its frozen state. Once thawed, it can be kept at 2°C to 8°C (36°F to 46°F) for up to 30 days. Imvamune, a third-generation non-replicating vaccine, offers more flexibility, with storage temperatures ranging from -25°C to -15°C (-13°F to 5°F) for long-term preservation and 2°C to 8°C (36°F to 46°F) for up to 8 weeks after thawing. These precise conditions are critical to prevent degradation and ensure the vaccines remain potent when needed.
In emergencies, rapid distribution is key. ACAM2000 is administered via a unique multiple puncture technique using a bifurcated needle, requiring careful training for healthcare workers. The standard dose is 0.0025 mL, applied to the upper arm. Imvamune, on the other hand, is given as a subcutaneous injection in a two-dose regimen, with doses spaced 28 days apart. Each dose is 0.5 mL, making it easier to administer but requiring careful tracking of recipients to ensure completion of the series.
Age restrictions and contraindications must be considered during deployment. ACAM2000 is approved for individuals aged 18 and older, while Imvamune is authorized for those aged 18 and above but has been studied in younger populations. Both vaccines are contraindicated in immunocompromised individuals, pregnant women, and those with certain skin conditions like eczema. In emergencies, risk-benefit assessments must be made swiftly to protect vulnerable populations without compromising safety.
Practical tips for emergency use include pre-positioning vaccines in regional hubs to reduce transportation time, ensuring cold chain integrity with backup power supplies, and training healthcare personnel in advance on administration techniques. Clear communication protocols are essential to coordinate distribution and monitor adverse reactions. While smallpox remains a threat only in theory, preparedness through proper vaccine storage and planning ensures that humanity remains one step ahead of potential outbreaks.
Mixing Vaccines: Safety, Efficacy, and What Science Says
You may want to see also
Explore related products






![]()
Smallpox vaccine effectiveness against related orthopoxviruses like monkeypox
The smallpox vaccine, originally developed to eradicate one of history's deadliest diseases, has demonstrated remarkable cross-protection against other orthopoxviruses, including monkeypox. This phenomenon is rooted in the genetic and structural similarities between these viruses, particularly in their surface proteins, which are primary targets of the immune response. Studies have shown that individuals vaccinated against smallpox during the eradication campaign of the 20th century retain significant immunity against monkeypox, with efficacy rates ranging from 85% to 90%. This residual immunity highlights the vaccine’s enduring legacy and its potential as a tool against emerging orthopoxvirus threats.
From a practical standpoint, the smallpox vaccine is administered as a single dose via a unique scarification method, where the vaccine is introduced into the skin using a bifurcated needle. This technique stimulates a robust immune response, producing neutralizing antibodies and memory cells that persist for decades. For individuals exposed to monkeypox, the vaccine can be used post-exposure prophylaxis (PEP) if administered within 4 to 14 days of contact. However, the vaccine’s availability is limited due to its historical discontinuation, and its use is typically reserved for high-risk groups, such as laboratory workers or those in outbreak zones.
A comparative analysis of the smallpox vaccine’s efficacy against monkeypox reveals both strengths and limitations. While it offers substantial protection, the vaccine’s reactogenicity, including side effects like fever, fatigue, and localized skin reactions, can deter its widespread use. Modern alternatives, such as the third-generation vaccines (e.g., MVA-BN and JYNNEOS), have been developed to mitigate these risks while maintaining efficacy. These newer vaccines are administered intramuscularly or subcutaneously, making them more accessible and safer for broader populations, including immunocompromised individuals and children.
Persuasively, the smallpox vaccine’s cross-protection underscores the importance of maintaining vaccine stockpiles and research infrastructure for orthopoxviruses. As monkeypox cases rise globally, the strategic use of smallpox vaccines in combination with newer formulations could serve as a critical stopgap measure. Public health agencies should prioritize educating at-risk populations about vaccination options, including dosage schedules (e.g., a two-dose regimen for JYNNEOS) and eligibility criteria. Additionally, ongoing surveillance and research are essential to monitor vaccine efficacy against evolving orthopoxvirus strains and ensure preparedness for future outbreaks.
In conclusion, the smallpox vaccine’s effectiveness against monkeypox exemplifies the enduring value of historical vaccination campaigns. While its use is constrained by availability and safety concerns, it remains a vital tool in the fight against orthopoxviruses. By integrating it with modern vaccines and adopting a proactive public health approach, we can maximize protection and minimize the impact of emerging threats. This dual strategy not only honors the legacy of smallpox eradication but also fortifies our defenses against the next viral challenge.
Was the Polio Vaccine Mandatory in the United States?
You may want to see also
Explore related products






![]()
Side effects and risks associated with smallpox vaccination
Smallpox vaccination, primarily using the Vaccinia virus, has been a cornerstone of public health, leading to the eradication of the disease. However, the vaccine is not without its side effects and risks, which must be carefully considered, especially in the context of its potential reintroduction for emergency preparedness. The most common side effect is a localized reaction at the vaccination site, known as the "take," which appears as a red, itchy lesion that progresses to a pustule and eventually scabs over. This is a normal immune response and typically resolves within 3 to 4 weeks. While this reaction is expected, it can be uncomfortable and may require careful management to prevent secondary infections.
Beyond localized reactions, systemic side effects can occur, particularly in individuals with compromised immune systems or certain medical conditions. These include fever, headache, fatigue, and muscle pain, usually appearing within a few days of vaccination. More severe but rare complications include postvaccinial encephalitis, an inflammation of the brain, which occurs in approximately 1 to 2 cases per million vaccinations. Another serious risk is progressive vaccinia, a condition where the Vaccinia virus continues to spread unchecked, often in immunocompromised individuals. This requires immediate medical attention and may necessitate the use of antiviral medications or Vaccinia immune globulin (VIG) for treatment.
Pregnant individuals and those with specific skin conditions, such as eczema or atopic dermatitis, face heightened risks. The Vaccinia virus can disseminate in these populations, leading to eczema vaccinatum, a severe and potentially life-threatening condition. For this reason, smallpox vaccination is contraindicated in pregnant individuals and those with a history of eczema or other exfoliative skin disorders. Household contacts of vaccine recipients, particularly children and immunocompromised individuals, are also at risk of contracting the Vaccinia virus through secondary transmission, emphasizing the need for strict adherence to post-vaccination care instructions.
Practical precautions can mitigate these risks. Vaccination sites should be kept clean and covered with a semi-occlusive bandage to prevent viral spread. Close contacts, especially those at higher risk, should avoid direct contact with the vaccination site until it is fully healed. Healthcare providers must screen potential recipients thoroughly, considering medical history, current health status, and living conditions. In the event of adverse reactions, prompt medical evaluation is critical, and treatments such as VIG should be administered as soon as possible to improve outcomes.
While the smallpox vaccine remains a powerful tool for preventing a devastating disease, its side effects and risks underscore the importance of targeted and cautious use. Balancing the benefits of immunity against the potential for harm requires careful patient selection, informed consent, and vigilant post-vaccination monitoring. As global health threats evolve, understanding and managing these risks will remain essential for any future smallpox vaccination campaigns.
Tonight's Vaccine Rollout: Stage Timings and What to Expect
You may want to see also
Explore related products

![]()
Global stockpiles of smallpox vaccines for potential bioterrorism threats
Smallpox, eradicated in 1980, remains a specter in global security due to its potential use as a bioterrorism agent. To counter this threat, strategic stockpiles of smallpox vaccines have been maintained worldwide. These reserves are not intended for routine immunization but serve as a critical defense mechanism in the event of a deliberate release of the virus. The vaccines in these stockpiles are primarily first-generation products, such as Dryvax, which were used during the eradication campaign. However, newer vaccines like ACAM2000 and third-generation candidates are also being developed to address safety concerns associated with older versions.
The management of these stockpiles involves careful consideration of vaccine efficacy, shelf life, and distribution logistics. For instance, ACAM2000, a FDA-approved vaccine, requires a single dose administered via a prong device that punctures the skin. This method, known as scarification, ensures a robust immune response. However, the vaccine is contraindicated for individuals with weakened immune systems, eczema, or those who are pregnant, highlighting the need for precise targeting in a crisis. Stockpiles must also account for rapid deployment, as the vaccine is most effective when administered within 4 days of exposure to the virus.
A comparative analysis of global stockpiling strategies reveals variations in approach. The United States, for example, maintains a stockpile of over 100 million doses of ACAM2000, supplemented by newer vaccines like JYNNEOS, which is safer for immunocompromised individuals. In contrast, the World Health Organization (WHO) holds a smaller reserve of 30 million doses, primarily for international response efforts. These differences underscore the balance between national security and global cooperation in bioterrorism preparedness.
Persuasively, the argument for maintaining and expanding these stockpiles rests on the unpredictable nature of bioterrorism threats. While smallpox no longer exists in nature, unverified stockpiles in rogue states or non-state actors pose a real risk. Vaccines not only serve as a deterrent but also provide a psychological buffer, reassuring populations that a response is possible. However, this strategy is not without challenges, including the cost of maintaining vaccines, ensuring their efficacy over time, and addressing public hesitancy toward vaccination in the absence of an immediate threat.
Practically, individuals should familiarize themselves with the basics of smallpox vaccination, particularly if they belong to high-risk groups such as healthcare workers or military personnel. Symptoms of vaccine side effects, like a sore arm or fever, are common but manageable. In the event of a bioterrorism incident, public health authorities would likely prioritize vaccination for those directly exposed and their close contacts. Staying informed about local and national preparedness plans can enhance personal and community resilience against this potential threat.
Live Vaccines and Pregnancy: Safety, Risks, and Recommendations Explained
You may want to see also
Frequently asked questions
Yes, there are vaccines for smallpox, and they were instrumental in the global eradication of the disease, which was declared by the World Health Organization (WHO) in 1980.
Smallpox vaccines are not routinely available to the general public, but stockpiles are maintained by governments and international organizations for emergency use in case of a bioterrorism threat or outbreak.
The smallpox vaccine has been shown to provide some cross-protection against monkeypox, a related virus. However, newer vaccines specifically designed for monkeypox are now available and preferred for that purpose.
The smallpox vaccine is generally safe, but it can cause side effects, particularly in individuals with weakened immune systems or certain skin conditions. It is not recommended for pregnant women, people with HIV/AIDS, or those with eczema or other skin disorders.