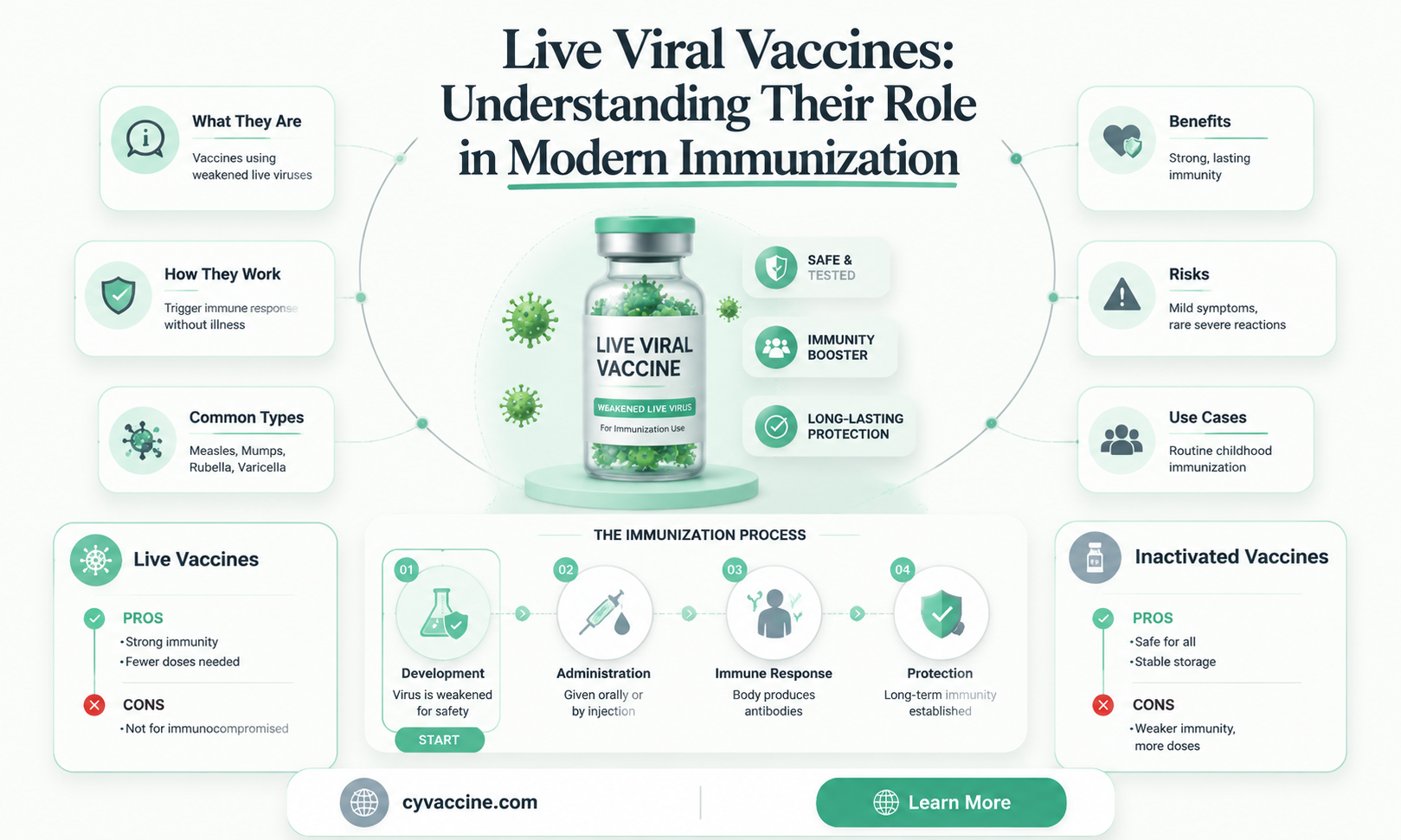
Live viral vaccines are a critical component of modern medicine, utilizing weakened or attenuated forms of viruses to stimulate a robust immune response without causing severe disease. These vaccines, such as those for measles, mumps, rubella (MMR), varicella (chickenpox), and yellow fever, are highly effective because they mimic natural infection, leading to long-lasting immunity. Unlike inactivated or subunit vaccines, live viral vaccines replicate within the body, triggering both humoral and cell-mediated immune responses. However, their use is carefully considered due to potential risks, such as reversion to virulence or adverse effects in immunocompromised individuals. Understanding the availability, mechanisms, and safety profiles of live viral vaccines is essential for informed public health decisions and disease prevention strategies.
| Characteristics | Values |
|---|---|
| Definition | Live viral vaccines contain weakened (attenuated) forms of the virus. |
| Mechanism | Stimulate a strong immune response by mimicking natural infection. |
| Examples | Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Yellow Fever, Oral Polio Vaccine (OPV), Rotavirus, Zoster (Shingles). |
| Immunity Type | Typically provides long-lasting, often lifelong immunity. |
| Dose Frequency | Usually requires fewer doses compared to inactivated vaccines. |
| Storage Requirements | Often requires refrigeration to maintain viability. |
| Safety | Generally safe but may cause mild symptoms similar to the disease. |
| Contraindications | Not recommended for immunocompromised individuals or pregnant women. |
| Shedding | Some live vaccines (e.g., OPV) can shed and rarely cause vaccine-derived disease. |
| Cost | Generally cost-effective due to fewer doses and long-lasting immunity. |
| Availability | Widely available globally, though access varies by region. |
| Development Time | Longer development time due to attenuation process. |
| Stability | Less stable than inactivated vaccines, requiring careful handling. |
| Public Perception | Occasionally faces skepticism due to misconceptions about safety. |
Explore related products






What You'll Learn
- Common Live Viral Vaccines: Examples include measles, mumps, rubella, varicella, and yellow fever vaccines
- Mechanism of Action: Live vaccines use weakened viruses to stimulate immune response without causing disease
- Safety Concerns: Rarely, live vaccines can cause mild illness or severe reactions in immunocompromised individuals
- Storage Requirements: Live vaccines often need refrigeration to maintain viral viability and effectiveness
- Contraindications: Not recommended for pregnant women, immunocompromised patients, or those with allergies to components
![]()
Common Live Viral Vaccines: Examples include measles, mumps, rubella, varicella, and yellow fever vaccines
Live viral vaccines are a cornerstone of preventive medicine, leveraging weakened forms of viruses to stimulate robust immune responses. Among the most widely recognized are the measles, mumps, rubella (MMR), varicella, and yellow fever vaccines. These vaccines contain attenuated viruses that replicate enough to trigger immunity but are too weak to cause severe disease in healthy individuals. For instance, the MMR vaccine is typically administered in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures long-term protection against three highly contagious diseases, with efficacy rates exceeding 95% after the second dose.
The varicella vaccine, targeting chickenpox, is another critical live viral vaccine. It is given in two doses, the first at 12–15 months and the second at 4–6 years, mirroring the MMR schedule. This vaccine not only prevents chickenpox but also reduces the risk of complications like bacterial infections and, later in life, shingles. Parents should note that mild side effects, such as soreness at the injection site or a mild rash, are common but transient. For travelers, the yellow fever vaccine is a live viral vaccine required for entry into certain countries. Administered as a single dose, it provides lifelong immunity and is recommended for individuals aged 9 months and older traveling to endemic areas.
Comparatively, live viral vaccines differ from inactivated or subunit vaccines in their mechanism of action. While inactivated vaccines use killed viruses, live vaccines mimic natural infection more closely, often requiring fewer doses for immunity. However, they are contraindicated in immunocompromised individuals due to the risk of the virus reverting to a virulent form. For example, pregnant women should avoid live viral vaccines like MMR and varicella, as theoretical risks to the fetus exist, though no evidence of harm has been documented.
Practical considerations for administering live viral vaccines include spacing them appropriately. If two live vaccines are not given simultaneously, they should be administered at least 4 weeks apart to ensure optimal immune response. Exceptions exist for the measles and varicella vaccines, which can be given concurrently without reducing efficacy. Storage is another critical factor; these vaccines require refrigeration at 2°C to 8°C to maintain potency. Healthcare providers must adhere to strict handling guidelines to avoid exposure to heat or light, which can degrade the vaccine.
In conclusion, live viral vaccines like MMR, varicella, and yellow fever are indispensable tools in public health. Their ability to confer long-lasting immunity with minimal doses makes them highly effective, though careful consideration of contraindications and administration protocols is essential. By understanding their unique characteristics and following best practices, healthcare providers and individuals can maximize the benefits of these vaccines while minimizing risks.
Where to Get the J&J Vaccine in Maryland: Locations & Availability
You may want to see also
Explore related products






![]()
Mechanism of Action: Live vaccines use weakened viruses to stimulate immune response without causing disease
Live viral vaccines represent a cornerstone of modern immunology, leveraging the body's natural defense mechanisms to confer long-lasting immunity. Unlike inactivated or subunit vaccines, live vaccines use attenuated (weakened) viruses that retain their ability to replicate but are incapable of causing severe disease in healthy individuals. This replication mimics a natural infection, triggering a robust immune response that includes the production of antibodies and the activation of memory cells. For instance, the measles, mumps, and rubella (MMR) vaccine contains live attenuated viruses that stimulate immunity without inducing the full-blown symptoms of these diseases. This approach ensures that the immune system is primed to recognize and neutralize the virus upon future exposure, providing durable protection.
The mechanism of action of live vaccines hinges on their ability to engage multiple arms of the immune system simultaneously. When administered, typically via injection or nasal spray, the weakened viruses infect cells and begin to replicate at a low level. This replication process alerts the innate immune system, which responds by releasing cytokines and chemokines to recruit immune cells to the site of infection. As the virus replicates, it is also presented to the adaptive immune system, where B cells produce antibodies and T cells mount a cellular response. The attenuated nature of the virus ensures that this process occurs without causing significant tissue damage or systemic illness. For example, the varicella-zoster vaccine (for chickenpox) uses a weakened strain of the virus that elicits immunity while avoiding the widespread rash and fever associated with the disease.
One of the key advantages of live vaccines is their ability to confer long-term immunity with minimal doses. Many live vaccines require only one or two administrations to achieve protective immunity, as the replication of the attenuated virus creates a sustained immune memory. For instance, the yellow fever vaccine, a live attenuated vaccine, provides lifelong immunity after a single dose in most individuals. However, this potency comes with specific considerations. Live vaccines are generally not recommended for individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, as the weakened virus could potentially cause disease in these populations. Additionally, live vaccines should not be administered to pregnant women due to theoretical risks to the fetus.
Practical tips for administering live vaccines include ensuring proper storage and handling to maintain the viability of the attenuated virus. Most live vaccines require refrigeration at 2°C to 8°C and must be protected from light. Healthcare providers should also be aware of potential interactions between live vaccines. For example, if two live vaccines are not administered on the same day, they should be spaced at least 4 weeks apart to avoid interference with immune responses. Age-specific guidelines are also critical; the rotavirus vaccine, a live oral vaccine, is typically given to infants in a series of doses starting at 6 weeks of age, as it is most effective when administered during early infancy.
In conclusion, live viral vaccines exemplify the elegance of immunological manipulation, using weakened viruses to stimulate a comprehensive immune response without causing disease. Their ability to confer long-lasting immunity with minimal doses makes them invaluable tools in public health. However, their use requires careful consideration of contraindications and practical guidelines to ensure safety and efficacy. By understanding the mechanism of action and adhering to best practices, healthcare providers can maximize the benefits of live vaccines while minimizing risks, contributing to the global effort to control and eradicate infectious diseases.
Vaccination Schedule: Diseases, Timelines, and Essential Immunizations Explained
You may want to see also
Explore related products






![]()
Safety Concerns: Rarely, live vaccines can cause mild illness or severe reactions in immunocompromised individuals
Live viral vaccines, such as those for measles, mumps, rubella (MMR), varicella (chickenpox), and yellow fever, contain weakened forms of the virus that trigger an immune response without causing full-blown disease in healthy individuals. However, their safety profile shifts dramatically in immunocompromised populations. For instance, the MMR vaccine, administered in two doses (typically at 12–15 months and 4–6 years), can lead to prolonged viral shedding or even vaccine-associated disease in those with weakened immunity. This risk underscores the importance of screening for conditions like HIV, leukemia, or recent chemotherapy before administration.
Consider the varicella vaccine, recommended for children over 12 months and adults without immunity. While it prevents severe chickenpox in most recipients, immunocompromised individuals may develop disseminated vaccine-strain varicella, a rare but serious complication. Similarly, the yellow fever vaccine, given as a single 0.5 mL dose, carries a higher risk of viscerotropic disease or neurologic complications in those with impaired immune systems. These examples highlight why live vaccines are contraindicated in specific groups, such as organ transplant recipients or individuals on high-dose corticosteroids.
The mechanism behind these risks lies in the vaccine’s design: live viruses replicate to stimulate immunity, but in immunocompromised hosts, this replication can spiral out of control. For example, the oral polio vaccine (OPV), though rarely used in developed countries today, historically caused vaccine-associated paralytic polio (VAPP) in about 1 in 2.7 million recipients, with immunocompromised individuals at significantly higher risk. This phenomenon illustrates the delicate balance between harnessing viral attenuation and ensuring safety across diverse populations.
To mitigate these risks, healthcare providers must adhere to strict guidelines. For instance, live vaccines should be avoided in individuals with severe combined immunodeficiency (SCID) or those undergoing stem cell transplants. In cases where vaccination is necessary, such as for travel-related yellow fever immunization, a thorough risk-benefit analysis is critical. Practical tips include verifying immune status through lab tests (e.g., CD4 counts in HIV patients) and spacing live vaccines by at least 4 weeks to minimize interaction.
While live vaccines remain cornerstone tools in disease prevention, their use in immunocompromised individuals demands vigilance. Rare but severe outcomes, such as vaccine-strain infections or systemic reactions, serve as reminders that one-size-fits-all approaches do not apply here. By prioritizing individualized assessment and adhering to contraindications, healthcare providers can maximize benefits while safeguarding vulnerable populations from unintended harm.
Understanding the Importance of Hepatitis B Vaccination for Your Health
You may want to see also
Explore related products






![]()
Storage Requirements: Live vaccines often need refrigeration to maintain viral viability and effectiveness
Live viral vaccines, such as those for measles, mumps, rubella (MMR), varicella (chickenpox), and yellow fever, rely on attenuated (weakened) viruses to stimulate immunity. Unlike inactivated vaccines, these live viruses remain viable but require careful handling to preserve their potency. One critical aspect of this is temperature control. Exposure to heat can degrade the viral components, rendering the vaccine ineffective. This is why the Centers for Disease Control and Prevention (CDC) mandates that live vaccines be stored between 2°C and 8°C (36°F and 46°F), a range that mimics refrigeration conditions. Deviations from this range, even for short periods, can compromise the vaccine’s efficacy, necessitating strict adherence to storage protocols in healthcare settings.
Consider the MMR vaccine, which is typically administered in two doses—the first at 12–15 months and the second at 4–6 years. If this vaccine is exposed to temperatures above 8°C for more than 72 hours, it may lose its potency, requiring the dose to be repeated. This is not merely an inconvenience; it can delay immunity in vulnerable populations, such as young children. Similarly, the varicella vaccine, given in two doses starting at 12–15 months, is highly sensitive to temperature fluctuations. Healthcare providers must use digital data loggers or temperature monitors in refrigerators to ensure consistent cooling and avoid accidental freezing, which can also destroy the live virus.
The logistical challenges of maintaining the cold chain are particularly acute in low-resource settings or during transportation. For instance, the yellow fever vaccine, a live-attenuated vaccine critical in endemic regions, must be kept refrigerated from manufacturing to administration. In remote areas without reliable electricity, solar-powered refrigerators or cold boxes with ice packs are often employed. Even in developed countries, power outages pose a risk, requiring backup generators or prompt relocation of vaccines to functional storage units. Failure to address these challenges can lead to vaccine wastage, increased costs, and gaps in immunization coverage.
Practical tips for healthcare providers include regularly calibrating refrigerator thermometers, storing vaccines in the middle of the unit (where temperatures are most stable), and avoiding overloading the refrigerator to ensure proper air circulation. Vaccines should never be placed in freezer compartments or near the door, where temperatures fluctuate most. Additionally, staff should be trained to handle vaccines properly, such as minimizing the time the refrigerator door is open and using vaccine carriers with cold packs for short-term transport. These measures, though seemingly minor, are essential to safeguarding the integrity of live viral vaccines and ensuring they confer the intended protection.
In summary, the storage requirements for live viral vaccines are not just technical details but critical determinants of their success. Refrigeration between 2°C and 8°C is non-negotiable, and even brief deviations can have significant consequences. From the MMR vaccine protecting children against three diseases to the yellow fever vaccine preventing outbreaks in high-risk areas, proper storage ensures these tools fulfill their life-saving potential. By prioritizing temperature control and adopting best practices, healthcare systems can maximize the impact of live vaccines, reinforcing their role as cornerstone interventions in global health.
Early Rabies Vaccination: Risks, Benefits, and What You Need to Know
You may want to see also
Explore related products






![]()
Contraindications: Not recommended for pregnant women, immunocompromised patients, or those with allergies to components
Live viral vaccines, such as those for measles, mumps, rubella (MMR), varicella (chickenpox), and yellow fever, are powerful tools in disease prevention. However, their use is not universal. Pregnant women, immunocompromised individuals, and those with allergies to vaccine components face specific risks that necessitate caution. These contraindications are rooted in the vaccines’ mechanism—live attenuated viruses, which, while weakened, retain the ability to replicate. For vulnerable populations, this replication can lead to unintended complications, making careful consideration essential before administration.
Pregnant women are advised to avoid live viral vaccines due to potential risks to the fetus. While no definitive evidence links these vaccines to congenital abnormalities, the theoretical risk of viral transmission to the fetus remains a concern. For example, the MMR vaccine is contraindicated during pregnancy, and women are encouraged to wait at least 4 weeks after vaccination before conceiving. In contrast, inactivated vaccines, such as the flu shot or Tdap, are safe and recommended during pregnancy, offering protection without the risks associated with live viruses. Pregnant women should consult healthcare providers to weigh risks and benefits, especially if traveling to areas with high disease prevalence.
Immunocompromised patients, including those with HIV/AIDS, cancer, or organ transplants, face heightened risks from live viral vaccines. Their weakened immune systems may struggle to control the attenuated virus, leading to vaccine-associated disease. For instance, the varicella vaccine can cause severe chickenpox-like illness in immunocompromised individuals. In such cases, healthcare providers often opt for passive immunization (e.g., immunoglobulins) or delay vaccination until immune function improves. Close contacts of immunocompromised patients should also be vaccinated to reduce disease transmission, a strategy known as cocooning.
Allergies to vaccine components, such as gelatin (in MMR and varicella vaccines) or antibiotics (in some formulations), pose another contraindication. Anaphylaxis, though rare, is a severe and immediate reaction that requires prompt medical attention. Individuals with a history of allergic reactions to vaccine components should undergo skin testing or desensitization protocols under medical supervision. Alternatively, component-free versions or adjusted formulations may be available. For example, gelatin-free MMR vaccines are used in some countries to mitigate this risk. Always disclose allergies to healthcare providers before vaccination to ensure safe administration.
In summary, while live viral vaccines are effective, their contraindications for pregnant women, immunocompromised patients, and those with allergies demand careful evaluation. Tailored approaches, such as alternative vaccines, timing adjustments, or allergy management, can mitigate risks. Healthcare providers play a critical role in assessing individual circumstances and recommending the safest course of action. By balancing protection and precaution, these vaccines can continue to safeguard public health without compromising vulnerable populations.
Is It Ever Too Late to Vaccinate Your Adult Cat?
You may want to see also
Frequently asked questions
Yes, there are several live viral vaccines in use today, including the measles, mumps, and rubella (MMR) vaccine, the varicella (chickenpox) vaccine, the rotavirus vaccine, and the yellow fever vaccine. These vaccines contain weakened (attenuated) forms of the virus that stimulate immunity without causing severe disease.
Live viral vaccines are generally safe for most healthy individuals, but they may not be recommended for people with weakened immune systems, pregnant women, or those with certain medical conditions. It’s important to consult a healthcare provider to determine if a live vaccine is appropriate for your specific situation.
While extremely rare, live viral vaccines can cause mild symptoms similar to the disease they prevent. For example, the MMR vaccine may cause a mild rash or fever, and the varicella vaccine may cause a mild chickenpox-like rash. However, these symptoms are typically much less severe than the actual disease and do not lead to serious complications in healthy individuals.