Adenoviruses are a group of common viruses that can cause a range of illnesses, from mild respiratory symptoms to more severe conditions like pneumonia or conjunctivitis. Over the years, researchers have developed adenovirus vaccines primarily for military personnel, as certain adenovirus types have historically caused outbreaks in military training settings. Notably, the U.S. Food and Drug Administration (FDA) approved an oral adenovirus vaccine (Adenovirus Type 4 and Type 7 Vaccine, Live, Oral) in 2011 for use in military populations. Additionally, adenovirus vectors have gained prominence in modern vaccine technology, serving as a platform for vaccines like those developed for COVID-19 (e.g., AstraZeneca and Johnson & Johnson). While these vector-based vaccines are not adenovirus vaccines in the traditional sense, they utilize adenovirus components to deliver genetic material, highlighting the versatility of adenoviruses in vaccine development. As of now, the only FDA-approved adenovirus vaccine specifically targets Types 4 and 7 and is restricted to military use, though ongoing research continues to explore their potential in other applications.
| Characteristics | Values |
|---|---|
| Approved Adenovirus Vaccines | Yes, there are approved adenovirus vaccines. |
| Examples | - Ad26.COV2.S (Janssen/Johnson & Johnson): Approved for COVID-19. |
| - Gam-COVID-Vac (Sputnik V): Uses adenovirus vectors (Ad26 and Ad5). | |
| - Convidecia (CanSino Biologics): Uses Ad5 adenovirus vector. | |
| Type of Vaccine | Viral vector-based vaccines (non-replicating adenovirus vectors). |
| Target Diseases | COVID-19, Ebola, and others (depending on the specific vaccine). |
| Approval Status | Approved by various regulatory bodies (e.g., WHO, FDA, EMA). |
| Efficacy | Varies by vaccine; e.g., Janssen ~66-72%, Sputnik V ~91.6%. |
| Administration Route | Intramuscular injection. |
| Dose Regimen | Typically single dose (Janssen) or two doses (Sputnik V). |
| Storage Requirements | Varies; some require refrigeration (2-8°C), others stable at room temp. |
| Side Effects | Common: Pain at injection site, fatigue, headache, mild fever. |
| Rare Side Effects | Rare cases of thrombosis with thrombocytopenia (TTS) reported. |
| Populations Approved For | Adults (18+), with some variations by country and vaccine. |
| Development Timeline | Rapid development during the COVID-19 pandemic (2020-2021). |
| Manufacturers | Johnson & Johnson, Gamaleya Research Institute, CanSino Biologics. |
| Global Usage | Widely used in various countries, especially in low-resource settings. |
Explore related products






What You'll Learn
![]()
Adenovirus vaccine approvals by WHO and FDA
As of recent updates, the World Health Organization (WHO) and the U.S. Food and Drug Administration (FDA) have both played pivotal roles in evaluating and approving vaccines targeting adenoviruses. Notably, adenovirus type 4 and type 7 vaccines, such as the oral vaccine used by the U.S. military, have received FDA approval for preventing acute respiratory disease in military personnel aged 17 to 50. This approval is specific to a two-dose regimen administered at a minimum interval of 10 days, highlighting the vaccine’s targeted use in high-risk populations rather than the general public.
The WHO, while not approving vaccines for routine immunization against adenoviruses, has acknowledged their significance in specific contexts, such as military settings or outbreaks in closed populations. For instance, the WHO’s Strategic Advisory Group of Experts (SAGE) has reviewed adenovirus vaccines for their efficacy and safety, emphasizing the need for localized risk assessments before deployment. This contrasts with the broader approvals seen for COVID-19 vaccines, where adenovirus vector-based platforms like AstraZeneca and Johnson & Johnson received emergency use listings from the WHO and full approvals from the FDA.
A critical distinction lies in the purpose of adenovirus vaccines. Unlike COVID-19 vaccines, which target SARS-CoV-2, approved adenovirus vaccines primarily address specific adenovirus serotypes (e.g., types 4 and 7) known to cause severe respiratory illnesses in confined populations. The FDA’s approval process for these vaccines included rigorous clinical trials demonstrating 90% efficacy in preventing acute respiratory disease, with side effects limited to mild gastrointestinal symptoms in some recipients.
For healthcare providers and policymakers, understanding the scope of these approvals is essential. The FDA-approved adenovirus vaccine is not interchangeable with COVID-19 vaccines using adenovirus vectors, such as AstraZeneca’s ChAdOx1. While both utilize adenovirus technology, their targets and formulations differ significantly. Practitioners should educate patients about this distinction to avoid confusion, especially in regions where multiple adenovirus-based vaccines may be in circulation.
In summary, while the WHO and FDA have approved adenovirus vaccines, their applications remain niche, targeting specific serotypes and populations. The FDA’s approval of the oral adenovirus type 4 and type 7 vaccine for military use underscores its role in preventing respiratory outbreaks in high-risk settings. Meanwhile, the WHO’s cautious stance reflects the need for tailored public health strategies rather than widespread deployment. For those seeking protection against adenovirus-related illnesses, consulting healthcare providers for accurate information and adhering to approved dosage regimens is crucial.
The US Transition to Two MMR Vaccines: A Timeline
You may want to see also
Explore related products






![]()
Current adenovirus vaccines for humans and their uses
Adenovirus vaccines have evolved significantly, with several approved for human use, primarily targeting specific serotypes and populations. Among the most notable is the Adenovirus Type 4 and Type 7 Vaccine, Live, Oral (also known as Adenovirus Vaccine Type 4 and Type 7, Live, Oral), approved by the U.S. Food and Drug Administration (FDA) for military personnel. This vaccine, administered orally in a single dose, protects against acute respiratory disease caused by adenovirus types 4 and 7, which are prevalent in crowded settings like military barracks. It is recommended for recruits aged 17–50, with a standard dose of 1.0 mL, taken on an empty stomach for optimal absorption. The vaccine’s live, attenuated nature ensures robust immune response, though it is contraindicated for individuals with compromised immune systems.
Beyond military applications, adenovirus vectors have revolutionized vaccine development, particularly in the fight against COVID-19. The Oxford-AstraZeneca (ChAdOx1 nCoV-19) and Johnson & Johnson (Janssen) COVID-19 vaccines utilize adenovirus vectors (chimpanzee adenovirus and human adenovirus type 26, respectively) to deliver genetic material encoding the SARS-CoV-2 spike protein. These vaccines are administered intramuscularly, with a standard dose of 0.5 mL. The AstraZeneca vaccine requires two doses, spaced 4–12 weeks apart, while the Janssen vaccine is a single-dose regimen. Both are approved for adults aged 18 and older, offering high efficacy against severe disease and hospitalization. However, rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS), have led to specific usage guidelines, emphasizing informed decision-making.
Another critical application of adenovirus vaccines is in ebola prevention. The Ervebo vaccine, developed by Merck, uses a recombinant vesicular stomatitis virus (VSV) vector to express the Ebola virus glycoprotein. While not an adenovirus-based vaccine, its success highlights the broader utility of viral vectors in vaccine technology. In contrast, the Ad26.ZEBOV vaccine by Johnson & Johnson employs a human adenovirus type 26 vector, administered as a prime-boost regimen with a modified vaccinia Ankara (MVA) vector-based vaccine. This two-dose approach, with an interval of 56 days, has been approved in Europe and several African countries for individuals at high risk of Ebola exposure.
For travelers and specific at-risk groups, adenovirus vaccines in development target additional serotypes, such as types 3 and 5, which cause conjunctivitis and respiratory infections. Clinical trials are exploring intranasal formulations to enhance mucosal immunity, a critical defense against respiratory pathogens. These vaccines often require lower dosages (e.g., 0.1–0.2 mL) and may be suitable for children as young as 6 months, pending safety and efficacy data. Practical tips for recipients include avoiding food and drink for 1–2 hours post-vaccination to ensure optimal uptake, particularly for oral formulations.
In summary, current adenovirus vaccines serve diverse purposes, from military health to global pandemic and epidemic control. Their versatility as vectors underscores their potential in modern vaccinology. While approved vaccines target specific populations and diseases, ongoing research promises broader applications, emphasizing the importance of tailored dosing, administration routes, and informed usage to maximize benefits and minimize risks.
Smoking Post-Vaccination: Risks and Effects You Need to Know
You may want to see also
Explore related products






![]()
Adenovirus vaccines in military populations: history and status
Adenovirus infections have long posed a significant challenge to military populations due to their highly contagious nature and ability to cause outbreaks in close quarters. Recognizing this threat, the U.S. military developed and approved an adenovirus vaccine in 1971, targeting serotypes 4 and 7, which were responsible for acute respiratory disease (ARD) among recruits. This live, oral vaccine was administered to all military trainees until its discontinuation in 1999 due to manufacturing issues. During its use, it reduced ARD cases by 90%, demonstrating its efficacy in preventing outbreaks in high-density environments.
The absence of an adenovirus vaccine for two decades left military populations vulnerable, with ARD cases resurging. In 2011, the U.S. Food and Drug Administration (FDA) approved a new adenovirus vaccine, Adenovirus Type 4 and Type 7 Vaccine, Live, Oral (Adenovirus Vaccine), exclusively for military use. This vaccine is administered as a single dose of 0.5 mL orally to recruits aged 17–50 years during basic training. Its reintroduction has significantly reduced ARD incidence, reinforcing its critical role in military health preparedness.
Comparatively, while adenovirus-based vaccines have gained prominence in civilian populations (e.g., COVID-19 vaccines like AstraZeneca and Johnson & Johnson), the military’s adenovirus vaccine serves a distinct purpose. Unlike vector-based vaccines, which use adenoviruses as delivery systems, the military vaccine targets adenovirus infections directly. This distinction highlights the tailored approach required for military health needs, where preventing outbreaks of specific pathogens is paramount.
Implementing the adenovirus vaccine in military populations requires careful logistics. Recruits must receive the vaccine within the first two weeks of training to maximize protection during peak vulnerability periods. Side effects are generally mild, including sore throat and headache, but medical staff should monitor for rare adverse reactions. Additionally, maintaining a cold chain for vaccine storage is critical, as the live vaccine must remain refrigerated at 2–8°C.
In conclusion, the history and status of adenovirus vaccines in military populations underscore their indispensable role in maintaining operational readiness. From the 1971 vaccine to the 2011 reintroduction, these vaccines have proven effective in controlling ARD outbreaks. As military environments continue to evolve, ongoing research and investment in adenovirus vaccines remain essential to safeguarding troop health and mission success.
Mastering Shingrix Administration: Correct Technique for Optimal Vaccine Efficacy
You may want to see also
Explore related products




![]()
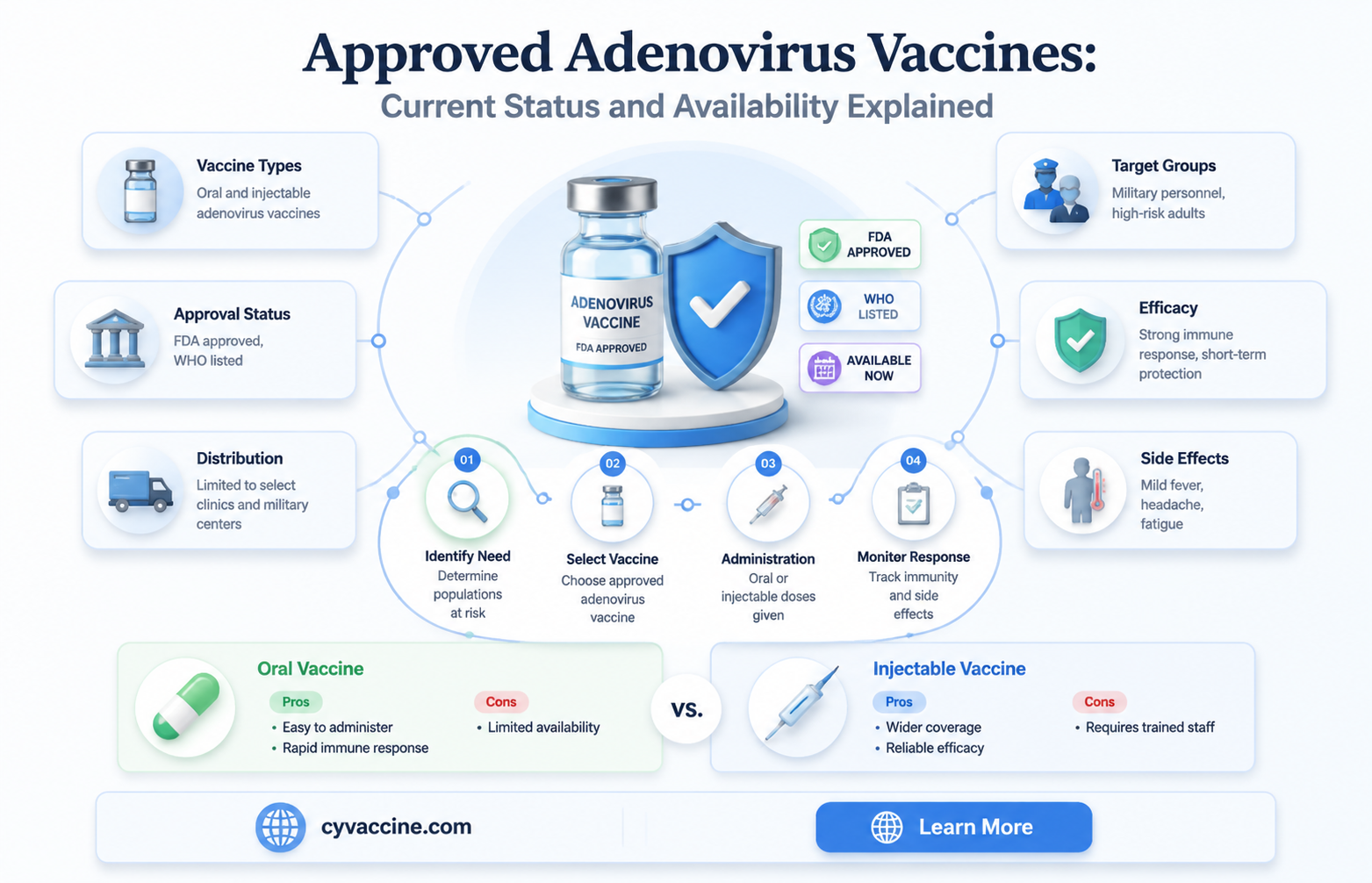
Clinical trials and efficacy of adenovirus vaccines
Adenovirus vaccines have undergone rigorous clinical trials to establish their safety and efficacy, particularly in preventing respiratory and gastrointestinal illnesses caused by specific adenovirus serotypes. One notable example is the U.S. military’s approved vaccine for adenovirus types 4 and 7, which was developed to protect recruits in high-risk training environments. Phase III trials involving over 10,000 participants demonstrated a 90% reduction in febrile adenovirus-related illnesses, with a standard two-dose regimen administered orally at a 1.5 mL volume per dose, spaced 1 to 2 months apart. This vaccine is recommended for active military personnel aged 17–50, highlighting its targeted application in specific populations.
In contrast to the military’s oral vaccine, adenovirus-based platforms have gained prominence in recent years for their role in delivering COVID-19 vaccines, such as AstraZeneca’s ChAdOx1 nCoV-19 and Johnson & Johnson’s Ad26.COV2.S. These vaccines utilize a non-replicating adenovirus vector (chimpanzee adenovirus and human adenovirus serotype 26, respectively) to express the SARS-CoV-2 spike protein. Clinical trials for these vaccines involved tens of thousands of participants across multiple countries, with efficacy rates ranging from 67% to 90% depending on dosing intervals and population demographics. For instance, a single dose of the Johnson & Johnson vaccine provided 66% protection against moderate to severe COVID-19 globally, rising to 72% in the U.S., with a standard 0.5 mL intramuscular injection.
A critical aspect of adenovirus vaccine efficacy is the immune response generated, which varies based on the vector and target antigen. For example, pre-existing immunity to the adenovirus vector can reduce vaccine effectiveness, as seen in some populations with high seroprevalence of adenovirus antibodies. To mitigate this, researchers have explored heterologous prime-boost strategies, such as combining adenovirus-vectored vaccines with mRNA or protein subunit vaccines. Studies have shown that a mixed regimen can enhance neutralizing antibody titers by up to 50%, particularly in older adults aged 65 and above, who often exhibit weaker responses to single-platform vaccines.
Despite their successes, adenovirus vaccines face challenges in balancing immunogenicity and reactogenicity. Common side effects, such as fatigue, headache, and injection site pain, are typically mild to moderate and resolve within 2–3 days. However, rare but serious adverse events, including vaccine-induced immune thrombotic thrombocytopenia (VITT), have been reported with certain adenovirus-vectored COVID-19 vaccines. These risks underscore the importance of post-authorization surveillance and tailored recommendations, such as restricting use in specific age groups or populations with predisposing conditions.
In summary, clinical trials have established adenovirus vaccines as effective tools for preventing specific diseases, with efficacy rates varying by serotype, vector, and target population. Practical considerations, such as dosing regimens, age-specific responses, and potential side effects, are crucial for maximizing their benefits. As research advances, ongoing trials and real-world data will continue to refine their application, ensuring they remain a valuable component of global public health strategies.
Did I Receive the Smallpox Vaccine as a Child?
You may want to see also
![]()
Adenovirus vector-based COVID-19 vaccines: approval and impact
Several adenovirus vector-based COVID-19 vaccines have been approved globally, marking a significant milestone in vaccine technology. The AstraZeneca (ChAdOx1 nCoV-19) and Johnson & Johnson (Janssen) vaccines are prime examples, utilizing modified adenoviruses to deliver genetic material encoding the SARS-CoV-2 spike protein. These vaccines have been authorized in over 100 countries, including the European Union, the United Kingdom, and India. Their approval was based on robust clinical trial data demonstrating efficacy rates ranging from 67% to 90%, depending on dosing regimens and populations studied. For instance, AstraZeneca’s vaccine is administered in two doses, typically 4 to 12 weeks apart, while Johnson & Johnson’s is a single-dose regimen, offering convenience and rapid immunity.
The approval of these vaccines has had a profound impact on global vaccination efforts, particularly in low- and middle-income countries. Their ease of storage—AstraZeneca’s vaccine can be kept at standard refrigerator temperatures (2°C to 8°C)—has made distribution more feasible in regions with limited cold chain infrastructure. However, their rollout has not been without challenges. Rare but serious side effects, such as vaccine-induced immune thrombotic thrombocytopenia (VITT), have led to age-based restrictions in some countries. For example, several European nations initially limited AstraZeneca’s vaccine to older adults (e.g., 55+) due to a higher risk of VITT in younger populations, though these restrictions have since been adjusted based on evolving data.
Comparatively, adenovirus vector-based vaccines have played a complementary role to mRNA vaccines like Pfizer and Moderna, which dominate in wealthier nations. Their lower cost and logistical advantages have made them critical tools in achieving global vaccine equity. For instance, COVAX, the global vaccine-sharing initiative, has distributed millions of AstraZeneca doses to low-income countries, underscoring their importance in bridging the immunization gap. However, public perception has been mixed, with some hesitancy fueled by media coverage of rare side effects and initial efficacy comparisons.
Practically, individuals receiving adenovirus vector-based vaccines should be aware of potential side effects, including injection site pain, fatigue, and headache, which are generally mild and resolve within a few days. In rare cases of severe symptoms, such as persistent headaches or unusual bruising, immediate medical attention is advised. For those with a history of severe allergies or specific medical conditions, consultation with a healthcare provider is recommended before vaccination. Pregnant and breastfeeding individuals are also advised to discuss the risks and benefits with their doctor, as data on these populations is still evolving.
In conclusion, adenovirus vector-based COVID-19 vaccines have been a vital component of the global pandemic response, offering accessible and effective protection against severe disease. Their approval and distribution highlight the importance of diverse vaccine platforms in addressing public health crises. While challenges remain, their impact on vaccination rates and global equity cannot be overstated, serving as a testament to scientific innovation and international collaboration.
When Should Kids Get the Influenza Type B Vaccine?
You may want to see also
Frequently asked questions
Yes, there are approved adenovirus vaccines, such as the ones developed for specific serotypes like adenovirus types 4 and 7, which are used by the U.S. military to protect against acute respiratory disease.
Yes, adenovirus vectors are used in some COVID-19 vaccines, such as AstraZeneca’s Vaxzevria (ChAdOx1) and Johnson & Johnson’s Janssen vaccine (Ad26), which have been approved in many countries.
Adenovirus vaccines, including those for COVID-19, have been deemed safe and effective by regulatory authorities like the FDA and WHO, though rare side effects such as blood clots or thrombosis with thrombocytopenia syndrome (TTS) have been reported.
Currently, there are no approved adenovirus vaccines for the common cold, as adenoviruses are just one of many viruses that cause colds, and developing a vaccine for all serotypes is challenging.
Yes, adenovirus vectors are being researched and used in vaccines for other diseases, such as Ebola (e.g., Johnson & Johnson’s Zabdeno) and malaria, with some already approved or in advanced clinical trials.