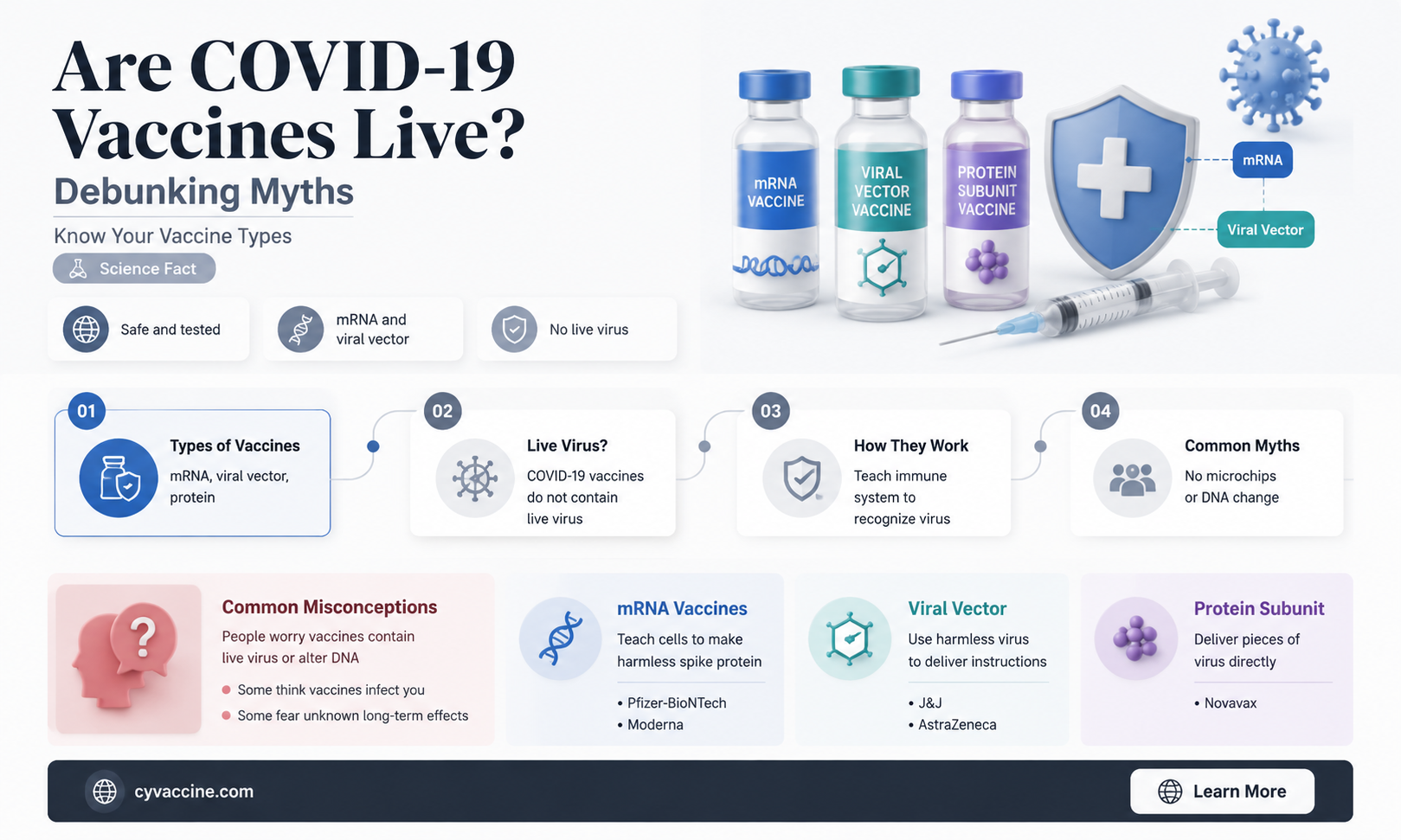
The question of whether COVID-19 vaccines contain live coronavirus has been a common concern among the public. It’s important to clarify that none of the authorized COVID-19 vaccines in use today—such as those developed by Pfizer-BioNTech, Moderna, Johnson & Johnson, or AstraZeneca—contain live coronavirus. Instead, these vaccines use different technologies, including mRNA (Pfizer and Moderna), viral vector (Johnson & Johnson and AstraZeneca), or protein subunit approaches, to teach the immune system to recognize and fight the virus without exposing the body to the actual virus itself. This ensures that the vaccines cannot cause COVID-19 infection, making them safe and effective for widespread use.
| Characteristics | Values |
|---|---|
| Are COVID-19 vaccines live? | No, none of the authorized COVID-19 vaccines in the U.S. contain live virus. |
| Vaccine Types | mRNA (Pfizer-BioNTech, Moderna), Viral Vector (Johnson & Johnson), Protein Subunit (Novavax) |
| mRNA Vaccines | Do not contain live virus; use genetic material to instruct cells to produce a harmless protein (spike protein). |
| Viral Vector Vaccines | Use a modified, harmless virus (not COVID-19) to deliver genetic instructions; does not contain live COVID-19 virus. |
| Protein Subunit Vaccines | Contain harmless pieces of the COVID-19 virus (spike protein) but no live virus. |
| Risk of Causing COVID-19 | None; vaccines cannot cause COVID-19 infection. |
| Immune Response | Triggers immune response without exposing the body to the live virus. |
| Storage Requirements | Varies by vaccine type (e.g., mRNA vaccines require ultra-cold storage initially). |
| Authorized for Use | Pfizer-BioNTech, Moderna, Johnson & Johnson, Novavax (in the U.S. and other regions). |
| Global Availability | Widely distributed globally, with varying access depending on region. |
| Booster Recommendations | Boosters recommended for enhanced protection, especially against variants. |
| Safety Profile | Thoroughly tested in clinical trials; monitored for safety post-authorization. |
| Common Side Effects | Pain at injection site, fatigue, headache, muscle pain, fever (mild and temporary). |
| Effectiveness Against Variants | Generally effective, though efficacy may vary slightly with new variants. |
| Approval Status | Fully approved or authorized for emergency use by regulatory bodies (e.g., FDA, EMA). |
Explore related products

$16.53 $17.99





What You'll Learn
- Vaccine Types: mRNA, viral vector, protein subunit, and inactivated virus vaccines explained briefly
- Live vs. Non-Live: Key differences between live-attenuated and non-replicating vaccines
- COVID-19 Vaccine Categories: Which COVID-19 vaccines are live or non-live
- Safety Concerns: Are live vaccines safe for immunocompromised individuals
- Efficacy Comparison: How do live and non-live vaccines compare in effectiveness
![]()
Vaccine Types: mRNA, viral vector, protein subunit, and inactivated virus vaccines explained briefly
The COVID-19 vaccines have sparked a global conversation about vaccine technology, with many curious about whether these vaccines contain live viruses. The answer lies in understanding the diverse types of vaccines developed to combat the coronavirus. Each type employs a unique strategy to train our immune system, and none of them contain live, intact SARS-CoV-2 viruses capable of causing disease.
MRNA Vaccines: The Genetic Instructors
These vaccines, exemplified by Pfizer-BioNTech and Moderna, deliver genetic material called mRNA encased in lipid nanoparticles. Once inside our cells, the mRNA acts as a blueprint, instructing them to produce a harmless piece of the virus’s spike protein. This triggers an immune response without exposing the body to the virus itself. Notably, mRNA does not alter our DNA. Dosage typically involves two shots, 3–4 weeks apart, with a booster recommended after 6 months. Ideal for ages 5 and up, these vaccines boast efficacy rates around 95% after full vaccination.
Viral Vector Vaccines: The Trojan Horses
Vaccines like AstraZeneca and Johnson & Johnson use a modified, harmless virus (the vector) to deliver genetic instructions for the spike protein. Unlike mRNA vaccines, the vector virus enters cells directly. Johnson & Johnson’s single-dose approach simplifies administration, while AstraZeneca requires two doses, 4–12 weeks apart. These vaccines are suitable for adults, with efficacy ranging from 67% to 90% depending on the variant. Rare side effects, such as blood clots, have been reported but are extremely uncommon.
Protein Subunit Vaccines: The Precision Tools
Novavax’s vaccine falls into this category, delivering lab-made spike proteins directly to the immune system. Adjuvants, substances that enhance immune response, are added to improve efficacy. This type avoids genetic material altogether, making it a familiar choice for those wary of newer technologies. Administered in two doses, 3 weeks apart, it’s approved for adults and has shown 90% efficacy against symptomatic infection. Its storage requirements (standard refrigeration) make it accessible in resource-limited settings.
Inactivated Virus Vaccines: The Traditional Approach
Vaccines like Sinovac and Sinopharm use whole SARS-CoV-2 viruses that have been inactivated (killed) to prevent replication. This method has been used for decades in vaccines like those for polio and hepatitis A. Multiple doses (typically two or three) are required to build immunity, with intervals of 2–4 weeks. While efficacy varies (50–80%), these vaccines are widely used globally, particularly in countries with limited access to mRNA or viral vector options. They’re suitable for adults and, in some cases, adolescents.
Understanding these vaccine types clarifies why none are "live" in the traditional sense. Each harnesses distinct mechanisms to prepare the immune system, offering a spectrum of choices tailored to global needs, logistical constraints, and individual preferences. Whether through genetic instructions, protein delivery, or inactivated viruses, these vaccines collectively represent a triumph of scientific innovation in the fight against COVID-19.
Iowa's Vaccination Lag: Unraveling the Barriers to Immunization Progress
You may want to see also
Explore related products






![]()
Live vs. Non-Live: Key differences between live-attenuated and non-replicating vaccines
The COVID-19 vaccines have sparked a global conversation about vaccine types, with a key distinction emerging between live-attenuated and non-replicating vaccines. Understanding this difference is crucial for informed decision-making, especially as new variants and booster recommendations arise. Live-attenuated vaccines, such as the measles-mumps-rubella (MMR) vaccine, contain a weakened version of the virus that can still replicate within the body, albeit at a reduced rate. In contrast, non-replicating vaccines, like the Pfizer-BioNTech and Moderna COVID-19 vaccines, utilize messenger RNA (mRNA) or viral vector technology to deliver genetic instructions without allowing the virus to replicate.
Mechanism and Immunity: Live-attenuated vaccines mimic a natural infection, triggering a robust immune response that often confers long-lasting immunity. For instance, a single dose of the yellow fever vaccine (a live-attenuated vaccine) provides lifelong protection for most recipients. Non-replicating vaccines, however, require multiple doses to achieve comparable immunity. The Pfizer-BioNTech COVID-19 vaccine, for example, is administered as a 2-dose primary series (30 μg each) for individuals aged 12 and older, followed by a booster dose (typically 50 μg) to enhance protection against waning immunity and emerging variants.
Safety and Administration: Live-attenuated vaccines are generally contraindicated in immunocompromised individuals, as the weakened virus may cause severe complications. Pregnant women and those planning to conceive are also advised to avoid live vaccines, unless the benefits outweigh the risks. Non-replicating vaccines, on the other hand, are considered safer for these populations. The Moderna COVID-19 vaccine, for instance, is authorized for use in individuals aged 18 and older, with a 2-dose primary series (100 μg each) and a booster dose (50 μg) recommended for optimal protection. It’s essential to follow healthcare provider guidance regarding dosage intervals, typically 3-4 weeks between primary doses and at least 5 months before a booster.
Efficacy and Practical Considerations: While live-attenuated vaccines often provide superior efficacy with fewer doses, their storage and handling requirements can be more stringent. The MMR vaccine, for example, must be stored at 2-8°C (36-46°F) and protected from light. Non-replicating vaccines, particularly mRNA-based ones, require ultra-cold storage (-60°C to -80°C) for long-term preservation, although they can be stored at standard refrigerator temperatures (2-8°C) for a limited time. For instance, the Pfizer-BioNTech vaccine can be stored at 2-8°C for up to 5 days, making it more logistically feasible for widespread distribution.
Choosing the Right Vaccine: The decision between live-attenuated and non-replicating vaccines depends on individual health status, age, and specific vaccine availability. For COVID-19, non-replicating vaccines have been the cornerstone of global vaccination efforts due to their safety profile and adaptability to new variants. However, ongoing research into live-attenuated COVID-19 vaccines, such as the COVI-VAC platform, highlights the potential for alternative approaches in the future. Always consult healthcare professionals to determine the most suitable vaccine based on personal medical history and community transmission rates. Practical tips include scheduling vaccinations during periods of good health, staying hydrated, and monitoring for adverse reactions, such as fever or injection site pain, which are typically mild and resolve within a few days.
Monkeypox Vaccine: Availability, Effectiveness, and What You Need to Know
You may want to see also
Explore related products






![]()
COVID-19 Vaccine Categories: Which COVID-19 vaccines are live or non-live?
The COVID-19 vaccines authorized for use fall into distinct categories based on their technology, with a key distinction being whether they are live or non-live. Understanding this difference is crucial for informed decision-making, especially for individuals with specific health concerns or preferences. Live vaccines use a weakened (attenuated) form of the virus, while non-live vaccines employ other methods to trigger an immune response without introducing a live virus. Among the COVID-19 vaccines, none are live vaccines. This is a critical point, as live vaccines can pose risks for immunocompromised individuals or pregnant people, but COVID-19 vaccines sidestep these concerns entirely.
The most widely used COVID-19 vaccines—Pfizer-BioNTech and Moderna—are mRNA vaccines, a non-live category. These vaccines deliver genetic instructions to cells to produce a harmless piece of the SARS-CoV-2 spike protein, prompting the immune system to recognize and combat it. Notably, mRNA does not interact with DNA, and the vaccines do not contain live virus particles. Dosage typically involves two primary shots (30 micrograms for Pfizer, 100 micrograms for Moderna) followed by boosters as recommended. These vaccines are approved for individuals aged 5 and older, with specific formulations for younger age groups.
Another non-live category includes viral vector vaccines, such as Johnson & Johnson (Janssen) and AstraZeneca. These vaccines use a modified, harmless virus (e.g., adenovirus) to deliver genetic material encoding the spike protein. Like mRNA vaccines, they do not contain live SARS-CoV-2 virus. The Johnson & Johnson vaccine is a single-dose option (0.5 mL), while AstraZeneca requires two doses (0.5 mL each). These vaccines are particularly useful in settings where cold chain storage is challenging, as they often have less stringent refrigeration requirements compared to mRNA vaccines.
Protein subunit vaccines, such as Novavax, represent another non-live category. These vaccines contain purified pieces of the virus (e.g., the spike protein) combined with an adjuvant to enhance immune response. Novavax, for instance, uses moth cell-produced spike proteins and Matrix-M adjuvant. Dosage is typically two 0.5 mL shots, administered three to four weeks apart. This type of vaccine is appealing for those hesitant about newer technologies like mRNA, as it relies on a more traditional approach to vaccination.
In summary, all authorized COVID-19 vaccines are non-live, eliminating concerns associated with live vaccines. Whether mRNA, viral vector, or protein subunit, these vaccines offer safe and effective protection against severe COVID-19 outcomes. Practical tips include checking local guidelines for age-specific dosages, staying updated on booster recommendations, and consulting healthcare providers for personalized advice, especially for those with underlying health conditions. Understanding these categories empowers individuals to make confident choices in safeguarding their health.
Healthcare Providers: Higher Child Vaccination Rates?
You may want to see also
Explore related products






![]()
Safety Concerns: Are live vaccines safe for immunocompromised individuals?
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened forms of the virus that trigger an immune response without causing disease in healthy individuals. However, for immunocompromised individuals—those with weakened immune systems due to conditions like HIV, cancer treatments, or organ transplants—live vaccines pose unique risks. The concern lies in the possibility of the attenuated virus replicating excessively, potentially leading to severe illness. For instance, the varicella vaccine (for chickenpox) is contraindicated for severely immunocompromised patients because the weakened virus can cause disseminated disease. This raises critical questions about the safety of live vaccines in this vulnerable population, particularly in the context of COVID-19 vaccines, none of which are live but whose safety profiles must still be considered for immunocompromised individuals.
Analyzing the COVID-19 vaccines, it’s important to note that none of them—whether mRNA (Pfizer, Moderna), viral vector (Johnson & Johnson), or protein subunit (Novavax)—contain live coronavirus. This eliminates the primary risk associated with live vaccines for immunocompromised individuals. However, safety concerns remain due to their reduced immune response. Studies show that immunocompromised individuals, such as organ transplant recipients, produce lower antibody levels post-vaccination. For example, a 2021 study in *JAMA* found that only 17% of solid organ transplant recipients developed detectable antibodies after one dose of an mRNA vaccine. This highlights the need for tailored strategies, such as additional doses or adjusting immunosuppressive medications, to enhance protection without compromising their underlying conditions.
Instructively, healthcare providers must carefully assess the risks and benefits before administering any vaccine to immunocompromised patients. For COVID-19, the CDC recommends a three-dose primary series of mRNA vaccines (Pfizer or Moderna) for this group, followed by a booster. For those who received Johnson & Johnson initially, an additional mRNA dose is advised. Practical tips include scheduling vaccinations during periods of less intense immunosuppression, if possible, and monitoring for adverse reactions. For example, a transplant recipient might consult their physician to temporarily adjust their anti-rejection medications around vaccination, though this must be balanced against the risk of organ rejection. Clear communication between specialists is essential to ensure coordinated care.
Persuasively, while live vaccines are generally contraindicated for immunocompromised individuals, the non-live nature of COVID-19 vaccines makes them a safer option for this population. However, their reduced efficacy underscores the importance of herd immunity. When communities achieve high vaccination rates, the risk of exposure decreases for those who cannot mount a full immune response. This collective responsibility is particularly critical in settings like hospitals, nursing homes, and public spaces where immunocompromised individuals are more likely to be present. By prioritizing vaccination and adhering to public health measures, society can protect its most vulnerable members.
Comparatively, the safety profile of COVID-19 vaccines for immunocompromised individuals contrasts sharply with live vaccines like yellow fever or oral polio. For instance, the yellow fever vaccine, which is live, is strictly contraindicated for those with severe immunodeficiency due to documented cases of vaccine-associated viscerotropic disease. In contrast, COVID-19 vaccines have not shown such risks, though their effectiveness remains suboptimal in this group. This distinction emphasizes the importance of vaccine design in ensuring safety across diverse populations. As research progresses, developing vaccines that balance efficacy and safety for immunocompromised individuals will remain a priority in global health.
Approved COVID-19 Vaccines for Individuals Aged 16 and Older
You may want to see also
Explore related products






![]()
Efficacy Comparison: How do live and non-live vaccines compare in effectiveness?
The COVID-19 vaccines authorized for use are not live vaccines. They primarily fall into two categories: mRNA vaccines (Pfizer-BioNTech, Moderna) and viral vector vaccines (Johnson & Johnson, AstraZeneca). These non-live vaccines introduce either genetic material or a harmless virus to teach the immune system to recognize and combat the SARS-CoV-2 virus. Live vaccines, in contrast, use a weakened form of the virus itself, as seen in measles or chickenpox vaccines. This fundamental difference in design raises questions about how their effectiveness compares.
Live vaccines historically boast high efficacy, often providing lifelong immunity with a single or few doses. For instance, the measles vaccine is 97% effective after two doses. Non-live COVID-19 vaccines, however, require a two-dose regimen (three for immunocompromised individuals) and still necessitate boosters due to waning immunity and emerging variants. The Pfizer vaccine, for example, showed 95% efficacy in clinical trials but dropped to around 60-70% against the Delta variant and even lower against Omicron without boosters. This highlights a trade-off: live vaccines offer robust, long-lasting immunity but carry a small risk for immunocompromised individuals, while non-live COVID-19 vaccines are safer for broader populations but require more frequent administration.
The mechanism of action further explains these differences. Live vaccines mimic a natural infection, stimulating a strong cellular and humoral immune response. Non-live COVID-19 vaccines, particularly mRNA types, focus on producing spike proteins, triggering a targeted but less comprehensive immune memory. This specificity is advantageous for safety but may limit their effectiveness against rapidly mutating viruses like SARS-CoV-2. For instance, the Johnson & Johnson vaccine, a viral vector type, provides around 66% efficacy against symptomatic infection globally but offers robust protection against severe disease and hospitalization, showcasing the nuanced effectiveness of non-live approaches.
Practical considerations also play a role. Live vaccines often require strict storage conditions and cannot be given to those with weakened immune systems. Non-live COVID-19 vaccines, especially mRNA ones, initially required ultra-cold storage but have since been optimized for standard refrigeration, easing distribution. Additionally, the ability to quickly modify mRNA vaccines to target new variants is a significant advantage. For example, updated bivalent boosters now target both the original virus and Omicron subvariants, addressing the evolving nature of the pandemic.
In summary, while live vaccines historically excel in efficacy and durability, non-live COVID-19 vaccines offer a safer, more adaptable solution for a global health crisis. Their effectiveness, though requiring boosters, is tailored to balance immunity with accessibility and safety. Understanding these differences empowers individuals to make informed decisions about vaccination, particularly as new variants and vaccine technologies emerge.
Vaccines vs. Natural Immunity: Why Modern Medicine Wins Every Time
You may want to see also
Frequently asked questions
No, none of the authorized COVID-19 vaccines in the U.S. (Pfizer, Moderna, Johnson & Johnson) are live vaccines. They do not contain a live virus.
No, mRNA vaccines do not contain live coronavirus. They use genetic material (mRNA) to instruct cells to produce a harmless protein that triggers an immune response.
No, the Johnson & Johnson vaccine is a viral vector vaccine, not a live vaccine. It uses a modified, harmless adenovirus to deliver genetic instructions, but it does not contain live coronavirus.
No, COVID-19 vaccines cannot give you the coronavirus because they do not contain live virus. They are designed to safely trigger immunity without causing infection.
No, none of the COVID-19 vaccines authorized for use in the U.S. or most other countries are live attenuated vaccines. They use different technologies like mRNA or viral vectors.