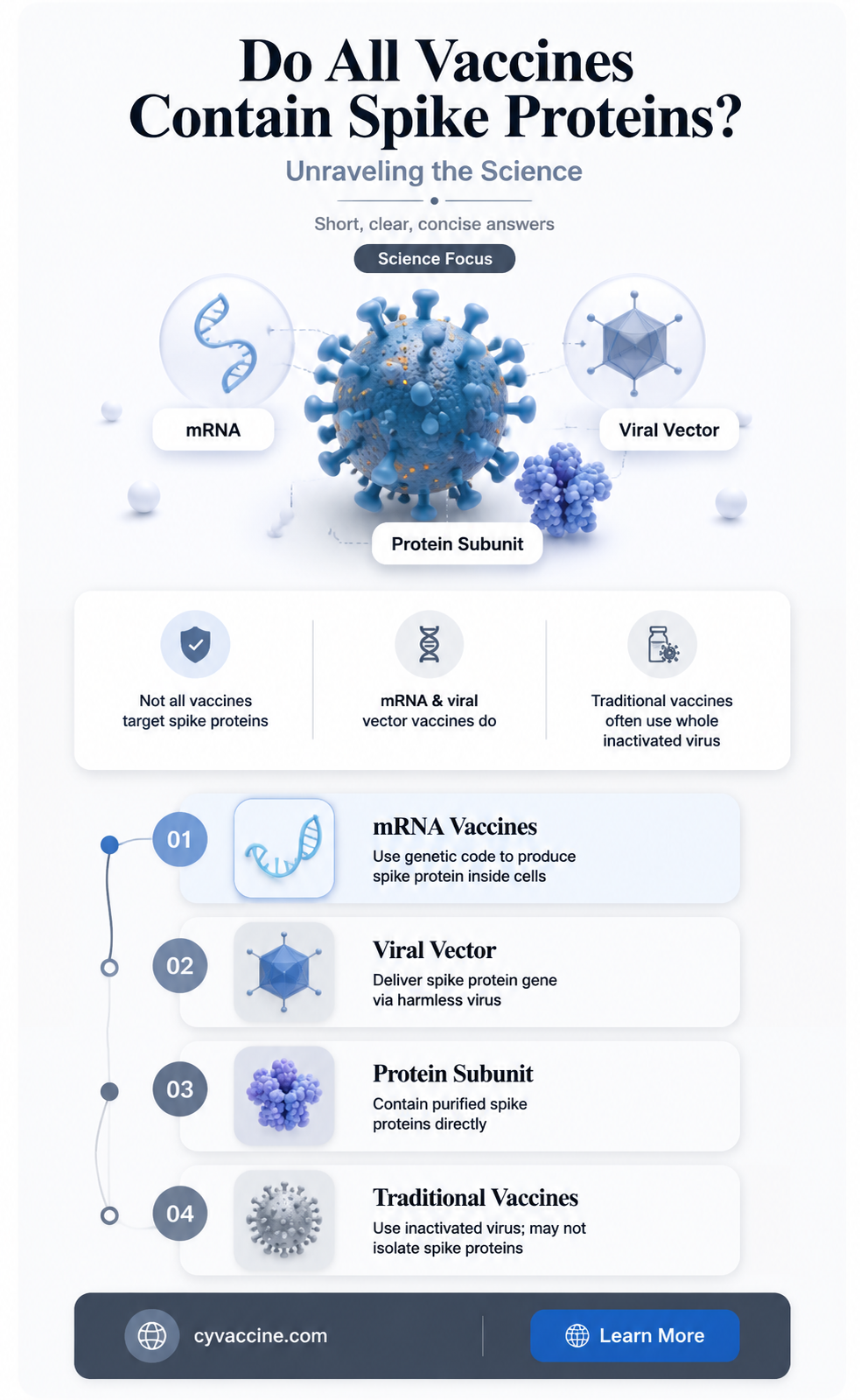
The question of whether spike proteins are present in all vaccines has gained attention, particularly in the context of COVID-19 vaccines, which use spike proteins as a key component to elicit an immune response. Spike proteins are specific to the SARS-CoV-2 virus and are not inherently found in all vaccines. Traditional vaccines, such as those for measles, mumps, or influenza, typically contain weakened or inactivated viruses, bacterial components, or purified antigens unrelated to spike proteins. mRNA and viral vector COVID-19 vaccines, however, are designed to instruct cells to produce the SARS-CoV-2 spike protein, triggering an immune response. Therefore, spike proteins are unique to certain vaccines and are not a universal component of all immunizations.
| Characteristics | Values |
|---|---|
| Presence in All Vaccines | No, spike proteins are not present in all vaccines. They are specific to certain types of vaccines, particularly mRNA and viral vector COVID-19 vaccines. |
| Vaccines Containing Spike Proteins | Pfizer-BioNTech (Comirnaty), Moderna (Spikevax), AstraZeneca (Vaxzevria), Johnson & Johnson (Janssen). |
| Function of Spike Proteins | Induce immune response by mimicking the SARS-CoV-2 virus's spike protein, teaching the immune system to recognize and combat the virus. |
| Vaccines Without Spike Proteins | Traditional vaccines (e.g., flu, measles, mumps, rubella) use inactivated viruses, live-attenuated viruses, or subunit proteins, not spike proteins. |
| Safety Profile | Spike proteins in COVID-19 vaccines are safe and degrade quickly after vaccination, with no long-term persistence in the body. |
| Misinformation | Claims that spike proteins are harmful or present in all vaccines are misinformation. They are specific to certain COVID-19 vaccines and are rigorously tested for safety. |
| Latest Research (as of 2023) | Studies confirm the safety and efficacy of spike protein-based vaccines, with no evidence of long-term adverse effects related to spike proteins. |
Explore related products






What You'll Learn
- COVID-19 Vaccines and Spike Proteins: Do all COVID-19 vaccines contain spike proteins
- Traditional Vaccines vs. Spike Proteins: Are spike proteins present in non-COVID vaccines
- mRNA Vaccines and Spike Proteins: How do mRNA vaccines utilize spike proteins
- Spike Protein Function: What role do spike proteins play in vaccine efficacy
- Safety of Spike Proteins: Are spike proteins in vaccines safe for humans
![]()
COVID-19 Vaccines and Spike Proteins: Do all COVID-19 vaccines contain spike proteins?
The COVID-19 pandemic spurred the rapid development of multiple vaccines, each employing distinct technologies to combat the virus. A central question arises: do all these vaccines utilize spike proteins, the key viral component enabling SARS-CoV-2 to infect cells? Understanding this is crucial for informed decision-making and addressing vaccine hesitancy.
Analyzing Vaccine Mechanisms
COVID-19 vaccines fall into three primary categories: mRNA (Pfizer-BioNTech, Moderna), viral vector (Johnson & Johnson, AstraZeneca), and protein subunit (Novavax). Both mRNA vaccines instruct cells to produce the spike protein, triggering an immune response. Viral vector vaccines deliver genetic material via a harmless virus to achieve the same effect. Novavax, however, directly injects lab-made spike proteins, paired with an adjuvant to enhance immunity. Notably, none of these vaccines contain live SARS-CoV-2 virus, ensuring they cannot cause COVID-19.
Comparing Spike Protein Delivery
While all approved COVID-19 vaccines target the spike protein, their methods differ. mRNA vaccines produce spike proteins within the body, a process that mimics natural infection without the virus’s harmful effects. Viral vector vaccines use a modified adenovirus to deliver spike protein instructions, a technique proven in Ebola vaccines. Protein subunit vaccines, like Novavax, administer pre-made spike proteins, a traditional approach seen in hepatitis B and pertussis vaccines. Each method has unique advantages, such as mRNA’s rapid scalability or protein subunit’s established safety profile.
Practical Considerations for Recipients
For individuals weighing vaccine options, understanding spike protein inclusion is vital. mRNA vaccines require two doses, typically 3–4 weeks apart, with a booster recommended 6 months later. Viral vector vaccines often need a single dose, though some countries recommend an mRNA booster for enhanced protection. Protein subunit vaccines, like Novavax, usually require two doses, 3–4 weeks apart. All vaccines are authorized for adults, with mRNA options available for children as young as 6 months. Consult healthcare providers to determine the best fit based on age, health status, and availability.
Addressing Concerns and Misinformation
Misconceptions about spike proteins have fueled vaccine hesitancy. Some falsely claim spike proteins cause harm, but extensive clinical trials and real-world data confirm their safety. The temporary presence of spike proteins post-vaccination is a normal immune response, not a cause for alarm. Additionally, no COVID-19 vaccine alters human DNA. By focusing on evidence-based facts, individuals can make informed choices, protecting themselves and their communities.
Takeaway: Spike Proteins as a Common Thread
While COVID-19 vaccines differ in technology, all approved options leverage the spike protein to induce immunity. Whether through mRNA, viral vectors, or protein subunits, this shared target ensures effective protection against severe illness and hospitalization. Understanding these mechanisms empowers individuals to trust in the science behind vaccination and take proactive steps toward public health.
Live vs. Killed Rabies Vaccines: Understanding the Key Differences
You may want to see also
Explore related products






![]()
Traditional Vaccines vs. Spike Proteins: Are spike proteins present in non-COVID vaccines?
Spike proteins, the key targets of COVID-19 vaccines, have become a household term, but their presence in other vaccines is a common misconception. Traditional vaccines, such as those for measles, mumps, and rubella (MMR), or influenza, do not contain spike proteins. Instead, they rely on different components of pathogens, like weakened or inactivated viruses, bacterial components, or specific antigens, to stimulate an immune response. For instance, the MMR vaccine uses live attenuated viruses, while the flu shot often contains inactivated virus particles. These vaccines have been safely administered for decades, with well-established dosing schedules—typically starting at 12–15 months for MMR and annually for influenza in adults and children over 6 months. Understanding this distinction is crucial for informed decision-making about vaccination.
To clarify further, spike proteins are unique to coronaviruses, including SARS-CoV-2, and are not a universal component of vaccines. Non-COVID vaccines target other parts of pathogens, such as the capsid proteins in the polio vaccine or the toxoids in the tetanus vaccine. For example, the DTaP vaccine (diphtheria, tetanus, and pertussis) for infants and children contains detoxified versions of bacterial toxins, not spike proteins. This targeted approach ensures the immune system learns to recognize and combat specific threats without unnecessary exposure to irrelevant components. Parents and caregivers should consult healthcare providers for age-appropriate dosing, such as the 5-dose DTaP series starting at 2 months, to ensure optimal protection.
A persuasive argument for the specificity of vaccine components lies in their design. Vaccines are meticulously engineered to mimic natural infections without causing disease, focusing on the most effective parts of pathogens. Spike proteins, while critical for COVID-19 vaccines, are irrelevant in vaccines like hepatitis B, which uses a recombinant surface antigen, or the pneumococcal conjugate vaccine, which targets bacterial polysaccharides. This precision underscores the scientific rigor behind vaccine development. For adults, the hepatitis B vaccine is typically administered in a 3-dose series over 6 months, while pneumococcal vaccines vary by age and health status. Recognizing this specificity builds trust in vaccine safety and efficacy.
Comparatively, the inclusion of spike proteins in COVID-19 vaccines represents a groundbreaking advancement in vaccine technology, particularly with mRNA and viral vector platforms. However, this innovation does not imply their presence in all vaccines. Traditional vaccines remain highly effective using established methods, as evidenced by the near-eradication of diseases like smallpox and the significant reduction in polio cases globally. For example, the oral polio vaccine, administered as drops, has been pivotal in low-income countries, while the inactivated injectable version is used in regions with low polio prevalence. This diversity in vaccine design highlights the adaptability of immunology to different pathogens, ensuring tailored protection without overcomplicating formulations.
In practical terms, understanding that spike proteins are not in non-COVID vaccines can alleviate concerns about vaccine ingredients. For instance, parents worried about the safety of childhood vaccines can focus on their proven track record rather than misinformation about spike proteins. The CDC’s recommended immunization schedule, which includes vaccines like varicella (chickenpox) and HPV, is designed to protect children at specific ages—varicella at 12–15 months and 4–6 years, and HPV starting at age 11–12. By debunking myths and emphasizing evidence-based practices, individuals can make confident choices about vaccination, ensuring broad immunity against preventable diseases.
Recommended Routine Schedule for the 4vHPV Vaccine: A Comprehensive Guide
You may want to see also
Explore related products






![]()
mRNA Vaccines and Spike Proteins: How do mRNA vaccines utilize spike proteins?
Spike proteins are not present in all vaccines, but they are a critical component of mRNA vaccines, particularly those developed to combat COVID-19. Traditional vaccines, such as those for measles or influenza, often use weakened or inactivated viruses, viral proteins, or toxins to elicit an immune response. In contrast, mRNA vaccines, like Pfizer-BioNTech and Moderna’s COVID-19 vaccines, take a revolutionary approach by delivering genetic instructions to cells, enabling them to produce a specific viral protein—the spike protein—that triggers immunity. This innovation marks a significant shift in vaccine technology, offering rapid development and highly targeted immune responses.
The role of the spike protein in mRNA vaccines is both precise and strategic. SARS-CoV-2, the virus causing COVID-19, uses its spike proteins to attach to human cells and initiate infection. mRNA vaccines exploit this mechanism by encoding only the genetic sequence for the spike protein, ensuring the immune system focuses on this critical target. Once injected, the mRNA enters muscle cells, where it is translated into spike proteins. These proteins are then displayed on the cell surface, prompting the immune system to recognize them as foreign and mount a defense. This process includes the production of antibodies and activation of T-cells, providing robust protection against the virus.
One of the key advantages of mRNA vaccines is their ability to generate a strong immune response with a relatively small dose. For instance, the Pfizer-BioNTech vaccine delivers 30 micrograms of mRNA in each of its two doses, while Moderna’s vaccine uses 100 micrograms per dose. This efficiency is partly due to the mRNA’s direct focus on the spike protein, which is highly immunogenic. Unlike traditional vaccines that may require larger quantities of antigen or adjuvants to stimulate immunity, mRNA vaccines achieve comparable or superior results with less material, reducing potential side effects and simplifying production.
Practical considerations for mRNA vaccines include storage and administration. These vaccines require ultra-cold storage (e.g., -70°C for Pfizer’s vaccine) to maintain mRNA stability, though advancements like Moderna’s formulation allow for storage at standard freezer temperatures. Once thawed, they must be used within a specific timeframe to ensure efficacy. For individuals receiving these vaccines, common side effects such as soreness at the injection site, fatigue, or mild fever are normal and indicate the immune system’s response. It’s essential to follow the recommended dosing schedule—typically two doses spaced 3–4 weeks apart—to achieve optimal protection.
In summary, mRNA vaccines leverage the spike protein’s central role in viral infection to create a highly effective and targeted immune response. By delivering genetic instructions for this protein, these vaccines train the body to defend against pathogens like SARS-CoV-2 with remarkable precision. Their innovative design not only ensures robust immunity but also sets a precedent for future vaccine development, particularly for emerging infectious diseases. Understanding this mechanism underscores the significance of spike proteins in modern vaccinology and highlights the transformative potential of mRNA technology.
Exploring the Limitations: A Key Weakness of DNA-Based Vaccines
You may want to see also
Explore related products






![]()
Spike Protein Function: What role do spike proteins play in vaccine efficacy?
Spike proteins are not present in all vaccines, but they are a critical component of mRNA and viral vector COVID-19 vaccines, such as those developed by Pfizer-BioNTech, Moderna, and AstraZeneca. These vaccines harness the spike protein’s unique structure to trigger an immune response, teaching the body to recognize and combat the SARS-CoV-2 virus. Unlike traditional vaccines that use weakened or inactivated pathogens, mRNA and viral vector vaccines deliver genetic instructions for cells to produce only the spike protein, avoiding the risks associated with introducing the entire virus. This targeted approach highlights the spike protein’s central role in vaccine efficacy, making it a key focus in modern immunology.
To understand the spike protein’s function, consider its natural role in the virus’s lifecycle. The spike protein acts as a key that allows the virus to enter human cells by binding to the ACE2 receptor. Vaccines exploit this mechanism by presenting a harmless version of the spike protein to the immune system. For instance, mRNA vaccines like Pfizer’s (30 µg dose) and Moderna’s (100 µg dose) deliver mRNA molecules encased in lipid nanoparticles, which instruct cells to produce the spike protein. Viral vector vaccines, such as AstraZeneca’s, use a modified adenovirus to deliver the spike protein gene. In both cases, the immune system identifies the spike protein as foreign, producing antibodies and activating T-cells to neutralize it. This process creates immunological memory, ensuring a faster, more effective response if the actual virus is encountered.
The efficacy of spike protein-based vaccines is evident in their real-world performance. Clinical trials showed Pfizer’s vaccine to be 95% effective in preventing symptomatic COVID-19 in individuals aged 16 and older, while Moderna’s demonstrated 94.1% efficacy. AstraZeneca’s vaccine, though slightly lower at 76% efficacy, still provided robust protection, particularly against severe disease. These outcomes underscore the spike protein’s ability to elicit a strong immune response. However, efficacy can vary based on factors like age, dosage, and emerging virus variants. For example, older adults may produce fewer antibodies post-vaccination, necessitating booster doses to maintain protection. Practical tips include adhering to recommended dosing intervals (e.g., 3–4 weeks for mRNA vaccines) and staying updated on booster guidelines to ensure sustained immunity.
A comparative analysis reveals why spike protein-based vaccines are not universal. Traditional vaccines, such as those for influenza or measles, often use whole viruses or viral components, not isolated spike proteins. For instance, the flu vaccine contains inactivated viral particles, while the measles vaccine uses a live attenuated virus. These approaches differ fundamentally from the precision of spike protein-based vaccines, which minimize side effects by avoiding unnecessary viral material. However, this specificity also means spike protein vaccines are highly tailored to their target pathogen, limiting their applicability to diseases where the spike protein is not a dominant antigen. This distinction highlights the importance of understanding the pathogen’s biology when designing vaccines.
In conclusion, the spike protein’s role in vaccine efficacy is both precise and transformative. By mimicking the virus’s entry mechanism without introducing its harmful effects, spike protein-based vaccines achieve high efficacy rates while maintaining safety. Their success in combating COVID-19 has set a precedent for future vaccine development, particularly for emerging infectious diseases. However, their application is not universal, as not all pathogens rely on spike proteins for infection. For practical implementation, healthcare providers should emphasize proper dosing, monitor variant-specific efficacy, and educate patients on the importance of completing vaccine regimens. This targeted approach ensures that the spike protein’s potential is maximized in the ongoing fight against infectious diseases.
Exploring the Latest Research: Are There Vaccines for HIV?
You may want to see also
Explore related products






![]()
Safety of Spike Proteins: Are spike proteins in vaccines safe for humans?
Spike proteins, a key component of COVID-19 vaccines, have been the subject of intense scrutiny and debate. These proteins, which enable the virus to attach to and enter human cells, are also the primary target of the immune response triggered by vaccines. The safety of spike proteins in vaccines is a critical question, especially given the rapid development and deployment of COVID-19 vaccines. To address this, it’s essential to examine the scientific evidence, regulatory approvals, and real-world data surrounding their use.
From an analytical perspective, the safety of spike proteins in vaccines is supported by rigorous clinical trials and ongoing post-authorization monitoring. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines, which encode for the spike protein, were tested in trials involving tens of thousands of participants across diverse age groups, including adolescents and older adults. These trials demonstrated a high safety profile, with the most common side effects being mild to moderate, such as pain at the injection site, fatigue, and headache. Regulatory bodies like the FDA and EMA have set strict standards for vaccine approval, ensuring that any rare adverse events, like myocarditis in young males, are identified and managed. Dosage adjustments, such as lower doses for children aged 5–11, further enhance safety by minimizing risks while maintaining efficacy.
Instructively, understanding the role of spike proteins in vaccines can alleviate concerns. Unlike the SARS-CoV-2 virus, which uses the spike protein to cause infection and disease, vaccines deliver only a harmless genetic blueprint (mRNA) or a stabilized version of the protein. This triggers an immune response without causing illness. Practical tips for vaccine recipients include staying hydrated, resting after vaccination, and monitoring for severe symptoms like chest pain or difficulty breathing, which should be reported immediately. For parents, explaining to children that the vaccine is like a "training manual" for their immune system can make the process less daunting.
Comparatively, the safety of spike proteins in vaccines stands in stark contrast to the risks posed by COVID-19 infection itself. The virus’s spike protein, when part of the intact virus, can lead to severe complications such as respiratory failure, blood clots, and long-term organ damage. Vaccines, on the other hand, present the spike protein in a controlled manner, allowing the immune system to recognize and neutralize it without the dangers of viral replication. Studies show that vaccinated individuals are significantly less likely to experience severe disease, hospitalization, or death compared to the unvaccinated, underscoring the safety and efficacy of this approach.
Persuasively, the global impact of spike protein-based vaccines cannot be overstated. As of 2023, billions of doses have been administered worldwide, with real-world data consistently affirming their safety. Countries with high vaccination rates have seen dramatic reductions in COVID-19-related deaths and hospitalizations, even amid emerging variants. While no medical intervention is entirely risk-free, the benefits of spike protein vaccines far outweigh the rare risks. Public health officials emphasize that vaccination remains the most effective tool in combating the pandemic, protecting not only individuals but also vulnerable populations through herd immunity.
In conclusion, the safety of spike proteins in vaccines is well-established through scientific research, regulatory oversight, and real-world evidence. By focusing on dosage precision, monitoring for rare side effects, and comparing vaccine risks to those of COVID-19 infection, it becomes clear that these vaccines are a safe and essential tool in public health. Practical steps, such as staying informed and following post-vaccination guidelines, can further enhance their safety and effectiveness.
Preventing Blood Clots Post-Vaccination: Essential Tips for a Safe Recovery
You may want to see also
Frequently asked questions
No, spike proteins are not present in all vaccines. Spike proteins are specific to mRNA and viral vector COVID-19 vaccines, such as Pfizer-BioNTech and Moderna, which teach cells to produce the SARS-CoV-2 spike protein to trigger an immune response. Traditional vaccines, like those for influenza or measles, do not contain spike proteins.
Not all COVID-19 vaccines use spike proteins. While mRNA and viral vector vaccines (e.g., Pfizer, Moderna, Johnson & Johnson) focus on the spike protein, other types like inactivated virus vaccines (e.g., Sinovac, Sinopharm) contain the entire virus in a non-infectious form, which includes but is not limited to the spike protein.
No, spike proteins in vaccines are not harmful to the body. They are designed to trigger a safe and effective immune response without causing disease. The spike proteins produced by COVID-19 vaccines are temporary and quickly broken down by the body after immunization. Extensive testing and monitoring confirm their safety.