Polio vaccines have been a cornerstone of public health in the United States since their introduction in the 1950s, effectively eradicating the once-feared disease domestically. Today, polio vaccination is standard in the U.S., with the Centers for Disease Control and Prevention (CDC) recommending a series of inactivated polio vaccine (IPV) doses for all children, starting at 2 months of age. This routine immunization has maintained the country’s polio-free status since 1979, though global efforts continue to combat the disease in endemic regions. While polio is no longer a significant threat in the U.S., the vaccine remains a critical component of childhood immunization schedules, ensuring continued protection against potential reintroduction of the virus.
| Characteristics | Values |
|---|---|
| Standardization in US | Yes, polio vaccines are part of the standard immunization schedule. |
| Vaccine Types | Inactivated Polio Vaccine (IPV) is the only type used in the US. |
| Age Groups | Administered to children at 2 months, 4 months, 6-18 months, and 4-6 years. |
| Routine Schedule | 4 doses total, with the first dose at 2 months and the last by age 6. |
| Catch-Up Vaccination | Available for children who missed earlier doses. |
| Adult Vaccination | Generally not needed unless at high risk (e.g., travel to endemic areas). |
| Effectiveness | Highly effective in preventing polio (over 99% after 3 doses). |
| Safety | Safe with minimal side effects (e.g., soreness at injection site). |
| Mandatory for School | Required in most states for school entry, with exemptions varying by state. |
| Global Eradication Efforts | Supported by the US through the Global Polio Eradication Initiative. |
| Last Reported Case in US | 1979 (wild poliovirus); rare cases from vaccine-derived strains. |
| CDC Recommendation | Strongly recommends IPV for all children as part of routine vaccination. |
Explore related products






What You'll Learn
![]()
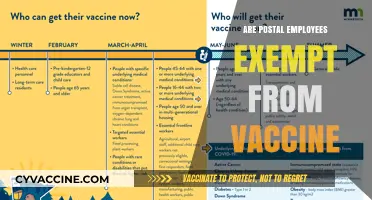
Polio vaccine schedule in the US
Polio vaccination in the United States follows a standardized schedule designed to ensure robust immunity from infancy. The Centers for Disease Control and Prevention (CDC) recommends a series of four doses of the inactivated poliovirus vaccine (IPV), administered at specific intervals to maximize protection. The first dose is given at 2 months of age, followed by subsequent doses at 4 months, 6-18 months, and 4-6 years. This schedule aligns with the routine childhood immunization timeline, making it convenient for parents and healthcare providers to ensure compliance.
The IPV is highly effective, offering over 99% protection against all three poliovirus types after the full series is completed. Unlike the oral polio vaccine (OPV), which is used in some countries, IPV cannot cause vaccine-derived poliovirus cases, making it the safer choice for countries like the U.S. where polio has been eradicated. Each dose contains 40 D-antigen units of Type 1, 8 D-antigen units of Type 2, and 32 D-antigen units of Type 3 poliovirus, ensuring a consistent and potent immune response.
For children who miss doses or start the series late, a catch-up schedule is available. Children aged 4 years or older who have received fewer than three doses should complete the series with the minimum interval of 4 weeks between doses. Adolescents and adults who are unvaccinated or incompletely vaccinated should receive a three-dose series, with the first two doses separated by 4-8 weeks and the third dose administered 6-12 months after the second. This flexibility ensures that individuals of all ages can achieve immunity, even if they fall behind on the standard schedule.
Travelers to polio-endemic or outbreak regions may require additional doses, regardless of their vaccination history. The CDC advises that adults who completed their childhood series receive a single lifetime IPV booster before travel. This precaution is particularly important due to the global effort to eradicate polio, as importing the virus into the U.S. remains a concern. Healthcare providers should consult the CDC’s travel health notices to determine if a booster is necessary for specific destinations.
Practical tips for parents include scheduling vaccinations during well-child visits to avoid missed doses and keeping a record of immunization dates. Schools and childcare facilities often require proof of vaccination, so maintaining updated records is essential. Additionally, parents should be aware that mild side effects, such as soreness at the injection site, are normal and typically resolve within a few days. By adhering to the polio vaccine schedule, families play a critical role in maintaining the U.S.’s polio-free status and contributing to global eradication efforts.
Bridgestone Arena: Vaccination Requirements for Entry
You may want to see also
Explore related products


$28.75



![]()
Types of polio vaccines used in the US
Polio vaccination in the United States relies on two distinct types: inactivated poliovirus vaccine (IPV) and oral poliovirus vaccine (OPV). While both target the same disease, their mechanisms, administration methods, and usage contexts differ significantly. Understanding these differences is crucial for informed decision-making and public health strategy.
IPV, the sole polio vaccine used in the U.S. since 2000, is administered through injection. This vaccine contains inactivated (killed) poliovirus, making it impossible to contract polio from the vaccine itself. The CDC recommends a four-dose series for children, given at 2 months, 4 months, 6-18 months, and 4-6 years. Adults traveling to polio-endemic areas or working in healthcare settings may require a booster dose. IPV boasts high efficacy, providing over 99% protection against paralytic polio after three doses.
OPV, while no longer used routinely in the U.S., plays a vital role in global polio eradication efforts. This live-attenuated vaccine is administered orally, making it easier to administer, especially in mass vaccination campaigns. However, a rare but serious drawback exists: vaccine-derived poliovirus (VDPV). In extremely rare cases, the weakened virus in OPV can revert to a virulent form, causing paralysis. This risk, albeit minuscule, led to the discontinuation of OPV in the U.S. where polio has been eradicated.
OPV's advantages lie in its ability to induce mucosal immunity, preventing viral shedding and transmission. This makes it a powerful tool in regions where polio remains endemic, helping to interrupt the virus's spread. The World Health Organization strategically employs OPV in targeted campaigns to eradicate the last remaining strains of wild poliovirus.
The choice between IPV and OPV hinges on the specific context. In polio-free countries like the U.S., IPV's safety profile and high efficacy make it the preferred choice. In regions battling active polio transmission, OPV's ability to halt viral spread outweighs the minimal risk of VDPV. This nuanced approach reflects the global health community's commitment to both individual protection and the ultimate goal of polio eradication.
Cuba's Childhood Vaccination Success: Rates, Strategies, and Global Impact
You may want to see also
Explore related products


$11.93 $21.99




![]()
Polio vaccine requirements for US schools
In the United States, polio vaccines are a cornerstone of public health, and their administration is tightly integrated into school entry requirements. Each state mandates that children receive a series of polio vaccinations before enrolling in kindergarten, with most requiring a minimum of three doses. These doses are typically administered as part of the inactivated poliovirus vaccine (IPV) schedule, starting at 2 months, 4 months, and 6-18 months of age, followed by a booster at 4-6 years. This structured approach ensures herd immunity and prevents the re-emergence of a disease once feared for its paralytic effects.
Compliance with these requirements is not just a bureaucratic formality but a critical public health measure. Schools act as both enforcers and educators, verifying vaccination records during enrollment and providing resources for parents to stay on track with their child’s immunization schedule. Exemptions are allowed in some states for medical, religious, or philosophical reasons, but these are increasingly scrutinized to prevent outbreaks. For instance, during the 2019 measles outbreak, states with stricter exemption policies saw lower transmission rates, underscoring the importance of minimizing vaccine refusal.
Practical tips for parents include scheduling vaccinations during well-child visits to avoid missed doses and keeping a detailed record of immunizations. The CDC’s Catch-Up Immunization Scheduler can assist families who fall behind, ensuring children meet school requirements without delay. Additionally, understanding the difference between IPV and the historically used oral polio vaccine (OPV) is key; IPV, the standard in the U.S., carries no risk of vaccine-derived poliovirus, making it safer for widespread use.
Comparatively, while polio has been eradicated in the U.S. since 1979, global travel and vaccine hesitancy pose ongoing risks. School vaccination requirements serve as a firewall, protecting not only individual students but also vulnerable populations, such as those with medical conditions that prevent vaccination. This dual role highlights why polio immunization remains a non-negotiable standard in U.S. education systems, despite the disease’s near disappearance domestically.
In conclusion, polio vaccine requirements for U.S. schools are a testament to the success of preventive medicine and the lessons learned from past epidemics. By adhering to these mandates, parents contribute to a collective shield against a once-devastating disease. Schools, in turn, play a vital role in maintaining this protection, ensuring that the next generation remains polio-free through rigorous enforcement and community education.
Is the TB Skin Test Included in Childhood Vaccinations?
You may want to see also
Explore related products






![]()
Polio vaccine coverage rates in the US
Polio vaccination in the United States is a cornerstone of public health, with coverage rates reflecting decades of successful immunization programs. According to the Centers for Disease Control and Prevention (CDC), approximately 93% of children aged 19-35 months receive the full series of polio vaccines, which typically includes four doses administered at 2 months, 4 months, 6-18 months, and 4-6 years of age. This high coverage rate is critical, as it not only protects individuals but also contributes to herd immunity, preventing the virus from circulating in communities. Despite this success, disparities exist, with lower coverage in certain states and among underserved populations, highlighting the need for targeted interventions.
Analyzing these coverage rates reveals both strengths and vulnerabilities in the U.S. immunization system. The polio vaccine, part of the routine childhood immunization schedule, is administered as the inactivated poliovirus vaccine (IPV), which is safe, effective, and has been in use since 2000. However, even a small drop in coverage can have significant consequences. For instance, a 5% decrease in vaccination rates could lead to a resurgence of polio, as the virus remains a threat in some parts of the world. Public health officials emphasize the importance of maintaining high coverage, especially in an era of vaccine hesitancy and misinformation, which can erode trust in established vaccines like IPV.
To ensure sustained high coverage, practical steps are essential. Parents and caregivers should adhere to the CDC’s recommended schedule, ensuring children receive doses at 2 months (first dose), 4 months (second dose), 6-18 months (third dose), and 4-6 years (booster). Schools and healthcare providers play a crucial role by requiring proof of vaccination for enrollment and offering catch-up doses for those who fall behind. Additionally, public health campaigns must address misinformation and emphasize the vaccine’s safety and efficacy, particularly in communities with lower uptake. For adults, especially those traveling to polio-endemic regions, a one-time IPV booster is recommended if they did not complete the childhood series.
Comparatively, the U.S. polio vaccine coverage rates outpace those of many other vaccines, such as the measles-mumps-rubella (MMR) vaccine, which faces higher resistance due to unfounded safety concerns. This success is partly due to the historical memory of polio’s devastating impact, which has fostered widespread acceptance of the vaccine. However, complacency remains a risk. Unlike diseases like measles, polio has not been seen in the U.S. since 1979, leading some to question the necessity of continued vaccination. Public health messaging must therefore balance celebrating eradication efforts with reminding the public that vaccination is the only way to keep polio at bay.
In conclusion, polio vaccine coverage rates in the U.S. are a testament to the power of immunization programs but require vigilance to maintain. By following the recommended schedule, addressing disparities, and combating misinformation, the nation can continue to protect its population from this once-feared disease. The story of polio vaccination is not just about numbers—it’s about the collective effort to safeguard future generations from a preventable tragedy.
Puppy Vaccination: The Two-Week Wait and Why
You may want to see also
Explore related products






![]()
Polio vaccine exemptions in US states
Polio vaccination rates in the U.S. hover around 93%, but this national average masks significant state-level disparities. While all 50 states mandate polio vaccination for school entry, exemptions create pockets of vulnerability. Understanding these exemptions is crucial for assessing polio's potential resurgence.
Let's examine the types of exemptions, their prevalence, and the implications for public health.
Medical exemptions, though rare, are universally accepted. These are granted for individuals with severe allergies to vaccine components or compromised immune systems. Non-medical exemptions, however, vary widely. Philosophical exemptions, based on personal beliefs, are permitted in 15 states, while religious exemptions are allowed in 44. States like Mississippi and West Virginia, with strict exemption policies, boast vaccination rates above 98%. Conversely, states with lenient exemptions, like Idaho and Oregon, see rates dip below 90%. This correlation underscores the impact of exemption policies on herd immunity.
A 2019 measles outbreak in Washington State, fueled by low vaccination rates in communities with high exemption rates, serves as a stark reminder of the consequences.
The process for obtaining exemptions differs across states. Some require a notarized statement, while others mandate consultation with a healthcare provider. Interestingly, states with more stringent requirements tend to have lower exemption rates. This suggests that even within the framework of allowing exemptions, measures can be taken to discourage their overuse.
The debate surrounding exemptions is complex. Proponents argue for individual liberty and religious freedom, while public health officials emphasize the collective responsibility to protect vulnerable populations. Striking a balance between these perspectives is challenging. Ultimately, the goal is to maintain high vaccination rates while respecting legitimate medical concerns and, where legally required, religious beliefs.
Polio's history as a devastating disease should not be forgotten. The success of vaccination campaigns has led to its near-eradication, but complacency could allow it to re-emerge. Understanding and addressing the nuances of exemptions is vital for safeguarding this hard-won victory.
Understanding Severe Allergic Reactions to Vaccines: Symptoms and Immediate Care
You may want to see also
Frequently asked questions
Yes, polio vaccines are part of the standard childhood immunization schedule in the US, as recommended by the Centers for Disease Control and Prevention (CDC).
The US exclusively uses the inactivated poliovirus vaccine (IPV), which is administered through injection. The oral polio vaccine (OPV) is not used in the US.
While the polio vaccine is recommended by the CDC, state laws determine vaccination requirements for school entry, and most states require it unless there is a medical or non-medical exemption.
Yes, polio vaccines remain necessary to prevent the reintroduction of the virus from other countries where it still exists and to maintain herd immunity.