The question of whether polio vaccines contain active or inactive components is a crucial aspect of understanding their mechanism and safety. Polio vaccines are primarily of two types: the oral polio vaccine (OPV), which uses a weakened (attenuated) form of the live virus, and the inactivated polio vaccine (IPV), which contains killed virus particles. OPV, being live but attenuated, stimulates a robust immune response in the gut, offering protection against all three polio strains, but carries a rare risk of vaccine-derived poliovirus. In contrast, IPV, composed of inactivated virus, is administered via injection, providing strong systemic immunity without the risk of causing polio, making it a safer option for individuals with weakened immune systems. The choice between active and inactive vaccines depends on factors like regional polio prevalence, immune status, and public health strategies.
| Characteristics | Values |
|---|---|
| Type of Vaccine | Both active (live attenuated) and inactive (inactivated) vaccines are available. |
| Live Attenuated Vaccine (OPV) | Contains a weakened form of the poliovirus that replicates in the intestine but does not cause disease in most individuals. |
| Inactivated Vaccine (IPV) | Contains killed poliovirus, incapable of replicating or causing disease. |
| Immunity | OPV provides both humoral (bloodstream) and mucosal (intestinal) immunity; IPV primarily provides humoral immunity. |
| Administration Route | OPV is administered orally; IPV is given via injection (intramuscular or subcutaneous). |
| Dose Schedule | OPV typically requires multiple doses; IPV is often given in a series of 3-4 doses. |
| Risk of Vaccine-Derived Polio | OPV carries a rare risk of vaccine-derived poliovirus (VDPV) causing paralysis in immunodeficient individuals or in under-immunized populations. |
| Storage Requirements | OPV requires refrigeration (2-8°C); IPV is more stable and can tolerate higher temperatures for short periods. |
| Global Usage | OPV has been the primary vaccine in global eradication efforts due to its ease of administration and ability to induce mucosal immunity; IPV is increasingly used in polio-free countries to avoid VDPV risks. |
| Cost | OPV is generally less expensive than IPV, making it more accessible in low-resource settings. |
| Current Recommendations | Many countries use a combination of IPV and OPV (sequential or mixed schedules) to maximize immunity while minimizing risks. |
Explore related products






What You'll Learn
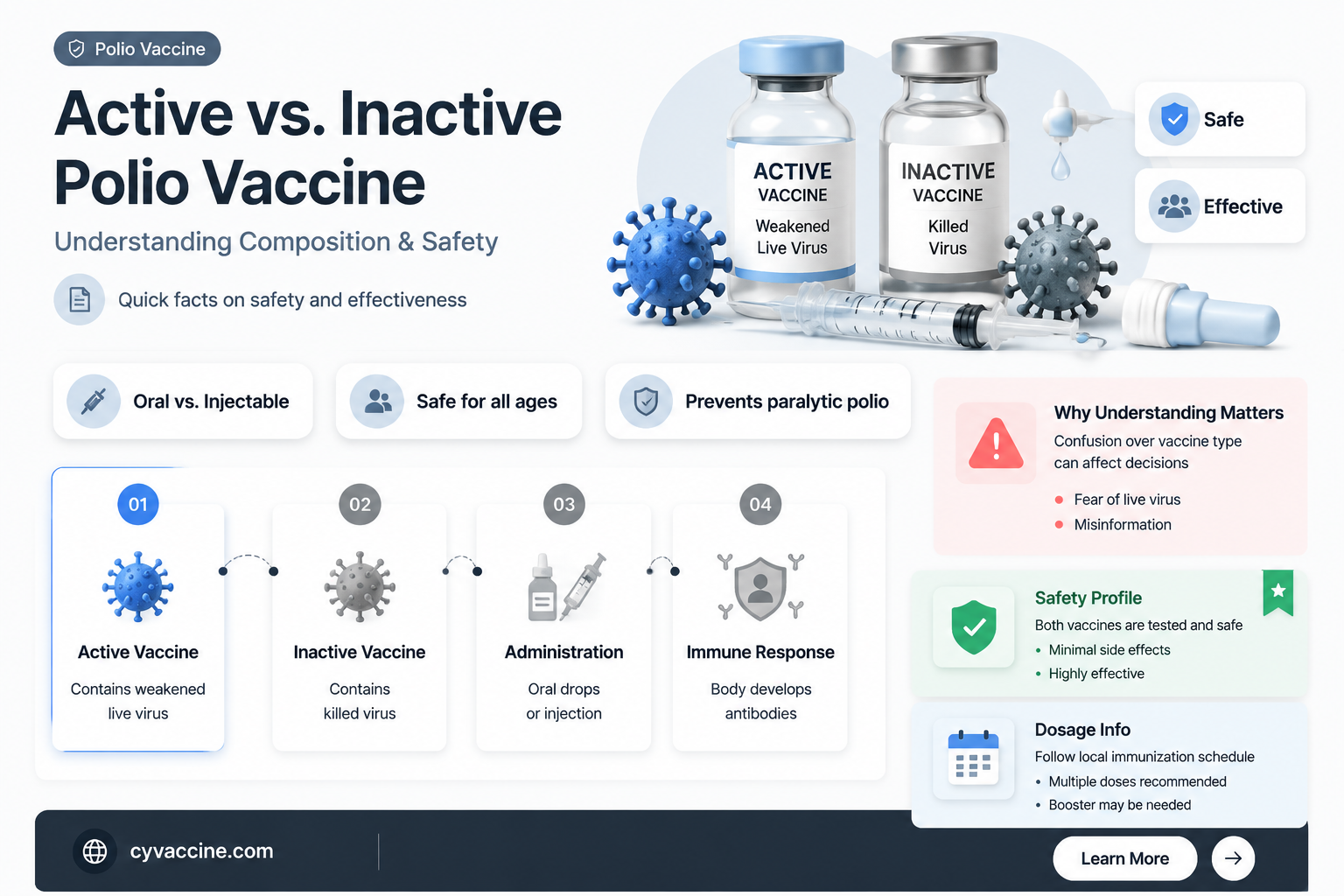
- Vaccine Types: Differentiating between oral (active) and injectable (inactive) polio vaccines
- Active Vaccine Mechanism: Live, weakened virus triggers immune response without causing disease
- Inactive Vaccine Mechanism: Killed virus stimulates immunity without replication risk
- Safety Comparison: Inactive vaccines safer for immunocompromised; active linked to rare risks
- Global Usage: Active vaccines in endemic areas; inactive preferred in polio-free regions
![]()
Vaccine Types: Differentiating between oral (active) and injectable (inactive) polio vaccines
Polio vaccines come in two primary forms: oral and injectable, each with distinct characteristics that influence their use and effectiveness. The oral polio vaccine (OPV) contains a live, attenuated (weakened) virus, making it an active vaccine. In contrast, the injectable polio vaccine, known as the inactivated polio vaccine (IPV), contains a killed virus, classifying it as an inactive vaccine. This fundamental difference in composition dictates their administration methods, immune responses, and suitability for different populations.
From an analytical perspective, the choice between OPV and IPV hinges on balancing efficacy and safety. OPV, administered as drops, stimulates both humoral (bloodstream) and mucosal (intestinal) immunity, providing robust protection against poliovirus transmission. However, its live nature carries a rare risk of vaccine-associated paralytic polio (VAPP), occurring in approximately 1 in 2.7 million doses. IPV, given as an injection, primarily triggers humoral immunity, eliminating the risk of VAPP but offering less protection against viral spread in the gut. This trade-off is critical in regions with varying polio prevalence and healthcare infrastructure.
Instructively, the administration of these vaccines follows specific guidelines. OPV is typically given in multiple doses, starting at 6 weeks of age, with a minimum interval of 4 weeks between doses. IPV, on the other hand, is often administered in a 3-dose series at 2, 4, and 6–18 months, followed by a booster at 4–6 years. For travelers to polio-endemic areas, the CDC recommends a single lifetime IPV booster for adults who completed their childhood series. Practical tips include ensuring proper storage (OPV requires refrigeration) and verifying vaccine availability, as global supply chains can affect accessibility.
Persuasively, the global shift from OPV to IPV in routine immunization schedules reflects evolving public health priorities. While OPV’s ability to induce intestinal immunity made it a cornerstone of polio eradication efforts, its rare but serious side effects prompted a transition to IPV in many countries. This change underscores the importance of tailoring vaccine strategies to local epidemiological contexts. For instance, countries nearing polio elimination prioritize IPV to minimize VAPP risks, while endemic regions may continue using OPV to interrupt viral transmission effectively.
Comparatively, the two vaccines exemplify the broader spectrum of vaccine technologies. OPV’s live, attenuated design mirrors vaccines like measles and mumps, offering durable immunity but requiring careful handling. IPV’s inactivated formulation aligns with vaccines such as hepatitis A, prioritizing safety over mucosal immunity. Understanding these distinctions empowers healthcare providers and policymakers to make informed decisions, ensuring optimal protection against polio while minimizing risks.
Descriptively, the experience of receiving these vaccines differs significantly. OPV’s oral administration is simple and painless, making it ideal for mass vaccination campaigns, especially in resource-limited settings. IPV, delivered via intramuscular or intradermal injection, may cause mild soreness at the injection site but is generally well-tolerated. Both vaccines play complementary roles in the global fight against polio, with OPV’s ease of use and IPV’s safety profile addressing distinct needs in diverse populations.
Coding for Vaccines: Debunking Myths and Uncovering Key Facts
You may want to see also
Explore related products






![]()
Active Vaccine Mechanism: Live, weakened virus triggers immune response without causing disease
The oral polio vaccine (OPV) is a prime example of an active vaccine mechanism, utilizing a live but weakened virus to stimulate a robust immune response. This vaccine contains attenuated strains of the poliovirus, which are designed to replicate in the gastrointestinal tract without causing paralysis or other severe symptoms of polio. When administered, typically as drops, the virus in OPV mimics a natural infection, prompting the body’s immune system to produce antibodies and activate memory cells. This dual-layered defense not only protects the individual but also reduces the spread of the virus in communities, contributing to herd immunity. For children under 5, who are most vulnerable to polio, OPV is often given in multiple doses (usually 3–4) to ensure full protection, with the first dose administered as early as 6 weeks of age in high-risk areas.
One of the key advantages of active vaccines like OPV is their ability to confer mucosal immunity, a critical defense mechanism against pathogens that enter the body through the mouth or nose. Unlike inactivated vaccines, which primarily generate systemic immunity, OPV triggers the production of IgA antibodies in the mucous membranes of the gut, where poliovirus initially replicates. This localized immune response is particularly effective in preventing viral shedding and transmission, making OPV a powerful tool in polio eradication campaigns. However, it’s essential to note that the live virus in OPV can, in rare cases (about 1 in 2.7 million doses), revert to a virulent form and cause vaccine-associated paralytic polio (VAPP). This risk is why OPV is being phased out in favor of the inactivated polio vaccine (IPV) in countries where polio has been eliminated.
From a practical standpoint, administering OPV requires minimal training and infrastructure, making it ideal for mass immunization campaigns in low-resource settings. The vaccine is stable at room temperature for a limited period, but proper storage between 2°C and 8°C is recommended to maintain its efficacy. Parents and caregivers should ensure their children receive all recommended doses, as partial vaccination leaves individuals susceptible to infection. In regions where polio remains endemic, such as Afghanistan and Pakistan, OPV continues to play a vital role in interrupting virus transmission. For travelers to these areas, the CDC advises receiving a dose of IPV before departure, as OPV is no longer used in the U.S. routine immunization schedule.
Comparatively, the inactivated polio vaccine (IPV) offers a safer alternative by using a killed virus, eliminating the risk of VAPP. However, IPV does not induce mucosal immunity or reduce viral shedding as effectively as OPV. This difference highlights the trade-offs between the two vaccines and underscores the importance of tailoring immunization strategies to local epidemiological contexts. In countries transitioning from OPV to IPV, a "sequential" approach is often adopted, where children receive one dose of IPV followed by OPV, combining the benefits of both vaccines. This hybrid strategy ensures strong individual protection while maintaining the community-level advantages of OPV.
In conclusion, the active vaccine mechanism exemplified by OPV demonstrates the power of using live, weakened viruses to trigger a comprehensive immune response. While its ability to confer mucosal immunity and halt transmission makes it indispensable in polio eradication efforts, the rare risk of VAPP necessitates careful consideration of its use. For healthcare providers and policymakers, understanding the nuances of OPV’s mechanism is crucial for designing effective vaccination programs. For parents, knowing how OPV works can alleviate concerns and reinforce the importance of completing the full vaccination series. As the world edges closer to polio eradication, the legacy of OPV serves as a testament to the ingenuity of active vaccine mechanisms in combating infectious diseases.
Federally Available Vaccines: Essential Immunizations for Children's Health and Safety
You may want to see also
Explore related products

$141.29 $179.99

$75.69 $119

$24.99

$6.99 $11.99


![]()
Inactive Vaccine Mechanism: Killed virus stimulates immunity without replication risk
The inactivated polio vaccine (IPV) contains a killed virus, incapable of replicating within the human body. This fundamental characteristic underpins its safety profile, particularly for individuals with compromised immune systems or those living in regions where wild poliovirus transmission has been eradicated. Unlike live attenuated vaccines, which carry a minuscule risk of reverting to a virulent form, IPV's non-replicating nature eliminates this concern entirely.
Example: The standard IPV schedule for infants in the United States consists of four doses: at 2 months, 4 months, 6-18 months, and 4-6 years. This regimen ensures robust immunity without the theoretical risks associated with live vaccines.
The mechanism of IPV's action relies on the immune system's ability to recognize and respond to viral antigens, even in the absence of viral replication. When the killed virus particles are injected, they are taken up by antigen-presenting cells, which process and display viral fragments on their surface. This presentation triggers the production of antibodies, primarily IgG, which circulate in the bloodstream and provide long-term protection against poliovirus infection.
Analysis: While IPV induces a strong humoral immune response, it is less effective at stimulating mucosal immunity compared to oral polio vaccine (OPV). This distinction is crucial in regions where poliovirus transmission persists, as mucosal immunity plays a critical role in preventing viral shedding and community spread.
From a practical standpoint, IPV offers several advantages, including its suitability for individuals with immunodeficiencies, pregnant women, and those with a history of allergic reactions to neomycin or polymyxin B. However, its administration requires intramuscular or subcutaneous injection, which may be less convenient than oral administration.
Caution: Although IPV is generally well-tolerated, mild side effects such as soreness at the injection site, fever, and irritability can occur. In rare cases, severe allergic reactions may develop, necessitating immediate medical attention.
In the context of global polio eradication efforts, IPV plays a complementary role to OPV. As countries transition from endemic to polio-free status, the risk of vaccine-associated paralytic poliomyelitis (VAPP) from OPV becomes a significant concern. IPV provides a safer alternative, allowing for the maintenance of population immunity without the risks associated with live vaccines.
Takeaway: The inactivated polio vaccine exemplifies the principle of using killed pathogens to stimulate immunity, offering a safe and effective means of protection against a once-devastating disease. Its unique mechanism, combined with a favorable safety profile, makes it an essential tool in the ongoing fight against polio.
To maximize the benefits of IPV, healthcare providers should adhere to recommended storage conditions (2-8°C) and administration techniques. Proper needle selection (e.g., 22-25 gauge for adults, 25-27 gauge for children) and injection site choice (vastus lateralis for infants, deltoid for older children and adults) are critical for ensuring optimal immunogenicity and minimizing adverse effects. By understanding the intricacies of IPV's mechanism and practical considerations, healthcare professionals can contribute to the sustained success of polio eradication initiatives.
Vaccines and Autism: Debunking Myths with Scientific Research
You may want to see also
Explore related products






![]()
Safety Comparison: Inactive vaccines safer for immunocompromised; active linked to rare risks
Polio vaccines come in two primary forms: inactivated (injectable) and live attenuated (oral). For immunocompromised individuals, the choice between these isn’t merely a preference—it’s a critical safety decision. Inactive polio vaccine (IPV), administered as a shot, contains no live virus, making it the safer option for those with weakened immune systems. In contrast, the oral polio vaccine (OPV), while highly effective, contains a weakened but live virus that, in rare cases, can revert to a virulent form and cause vaccine-associated paralytic polio (VAPP). This risk, though minuscule (approximately 1 in 2.7 million doses), is significant enough to warrant avoidance in immunocompromised populations.
Consider the practical implications for a child undergoing chemotherapy or an adult with HIV. For them, IPV is the recommended choice, as it eliminates the risk of vaccine-derived poliovirus infection. The CDC and WHO guidelines explicitly advise against OPV for such individuals, emphasizing the importance of IPV’s sterile formulation. Even household contacts of immunocompromised individuals are advised to avoid OPV to prevent shedding of the live virus, which could theoretically expose vulnerable family members. This layered approach underscores the principle of prioritizing safety in high-risk groups.
The dosage and administration of IPV further highlight its suitability for immunocompromised individuals. Typically given as a series of 3–4 doses starting at 2 months of age, IPV provides robust protection without overwhelming the immune system. Booster doses are recommended for adults traveling to polio-endemic regions, ensuring ongoing immunity without the risks associated with live vaccines. For example, a 65-year-old with rheumatoid arthritis on immunosuppressive therapy would receive IPV rather than OPV, even if they were previously vaccinated with OPV as a child.
While OPV’s role in global polio eradication is undeniable, its use in immunocompromised populations is a calculated risk that modern guidelines no longer endorse. IPV’s safety profile, combined with its efficacy, makes it the gold standard for protecting those most vulnerable to infection. For healthcare providers, the takeaway is clear: when in doubt, choose inactive. This simple rule safeguards patients whose immune systems cannot afford even the slightest gamble.
Grey's Anatomy Vaccine Trial: Unraveling Levi's Role in Medical Research
You may want to see also
Explore related products






![]()
Global Usage: Active vaccines in endemic areas; inactive preferred in polio-free regions
In regions where polio remains endemic, the oral polio vaccine (OPV), an active vaccine, is the cornerstone of eradication efforts. This live-attenuated vaccine is administered orally, typically in multiple doses starting at 6 weeks of age, with a minimum of three doses required for full protection. Its effectiveness lies in its ability to induce both humoral and mucosal immunity, preventing viral replication in the gut and shedding, which helps curb community transmission. However, the rarity of vaccine-associated paralytic polio (VAPP)—occurring in approximately 1 in 2.7 million doses—necessitates careful risk-benefit analysis in these areas. Despite this risk, OPV’s superior ability to interrupt wild poliovirus transmission makes it indispensable in high-risk settings.
Contrastingly, polio-free regions predominantly rely on the inactivated polio vaccine (IPV), which contains killed virus particles. Administered via intramuscular or subcutaneous injection, IPV is recommended in a four-dose series: at 2, 4, 6–18 months, and 4–6 years. While IPV does not induce mucosal immunity and thus does not prevent viral shedding, it effectively protects against paralytic disease. Its safety profile, devoid of VAPP risk, aligns with the priorities of regions where wild poliovirus circulation has been eliminated. For instance, the United States transitioned exclusively to IPV in 2000 after achieving polio-free status, minimizing even the rare risks associated with OPV.
The strategic shift from OPV to IPV in polio-free regions is not without challenges. IPV’s higher cost and logistical demands, such as cold chain maintenance and trained personnel for injection, can strain healthcare systems. However, its safety advantages outweigh these drawbacks in settings where the risk of poliovirus importation is low. Meanwhile, endemic countries often employ a sequential approach, using OPV for mass campaigns and IPV in routine immunization to balance efficacy and safety. This dual strategy ensures robust population immunity while minimizing VAPP cases.
Practical considerations further underscore the global usage divide. In endemic areas, OPV’s ease of administration—often delivered door-to-door during campaigns—maximizes coverage in hard-to-reach populations. Conversely, polio-free regions prioritize IPV’s safety, integrating it into routine childhood immunization schedules. Travelers from polio-free to endemic areas are advised to receive a single lifetime IPV booster if their last dose was over 10 years prior, ensuring continued protection without reintroducing live vaccine strains.
Ultimately, the choice between active and inactive polio vaccines reflects a nuanced balance of epidemiological context, risk tolerance, and resource availability. While OPV remains critical for eradicating polio in endemic areas, IPV’s safety and efficacy make it the preferred choice in polio-free regions. This tailored approach exemplifies global health’s adaptive strategies, ensuring that vaccination efforts are both effective and contextually appropriate.
Understanding the Design and Features of a Paper Vaccine Passport
You may want to see also
Frequently asked questions
Polio vaccines can be either active (live attenuated) or inactive (inactivated). The oral polio vaccine (OPV) contains weakened live viruses, while the injectable inactivated polio vaccine (IPV) contains killed viruses.
The inactivated polio vaccine (IPV) is more commonly used globally today due to its safety profile and reduced risk of vaccine-derived poliovirus cases compared to the live attenuated oral polio vaccine (OPV).
In extremely rare cases, the live attenuated oral polio vaccine (OPV) can revert to a virulent form and cause vaccine-associated paralytic polio (VAPP) or circulate as vaccine-derived poliovirus (VDPV). This is why IPV is preferred in many countries.