The claim that peanut allergies are caused by vaccines is a topic that has circulated in public discourse, often fueled by misinformation and anecdotal evidence. However, scientific research and medical consensus overwhelmingly refute this assertion. Peanut allergies are primarily attributed to genetic predisposition, immune system responses, and environmental factors, with no credible studies linking them to vaccines. Vaccines undergo rigorous testing and monitoring to ensure safety, and their ingredients are thoroughly vetted to avoid allergens like peanuts. Misinformation about vaccines can lead to unwarranted fear and potentially harm public health by discouraging vaccination. It is crucial to rely on evidence-based information from reputable sources when addressing such claims.
| Characteristics | Values |
|---|---|
| Scientific Evidence | No credible scientific evidence supports a causal link between vaccines and peanut allergies. |
| Medical Consensus | Leading health organizations (e.g., CDC, WHO, AAP) state that vaccines do not cause peanut allergies. |
| Vaccine Ingredients | Vaccines do not contain peanut proteins or allergens. |
| Allergy Mechanisms | Peanut allergies are caused by immune responses to peanut proteins, not vaccine components. |
| Prevalence Trends | Rise in peanut allergies is attributed to factors like dietary changes, hygiene hypothesis, and genetic predisposition, not vaccines. |
| Clinical Studies | Numerous studies have found no association between vaccination and the development of peanut allergies. |
| Expert Opinions | Allergists and immunologists confirm no scientific basis for vaccines causing peanut allergies. |
| Public Misconceptions | Misinformation and anecdotal claims persist despite lack of evidence. |
| Safety Monitoring | Vaccine safety systems (e.g., VAERS, VSD) have not identified peanut allergies as a vaccine-related adverse event. |
| Conclusion | Vaccines are not a cause of peanut allergies; they are safe and essential for public health. |
Explore related products






What You'll Learn
- Vaccine Ingredients and Allergens: Do vaccine components like stabilizers or preservatives trigger peanut allergies
- Immune System Response: Can vaccines alter immune reactions, leading to peanut sensitivity
- Epidemiological Studies: Is there a correlation between vaccination rates and peanut allergy prevalence
- Cross-Reactivity Concerns: Do vaccine antigens cross-react with peanut proteins, causing allergies
- Scientific Evidence Review: What research supports or refutes the vaccine-peanut allergy link
![]()
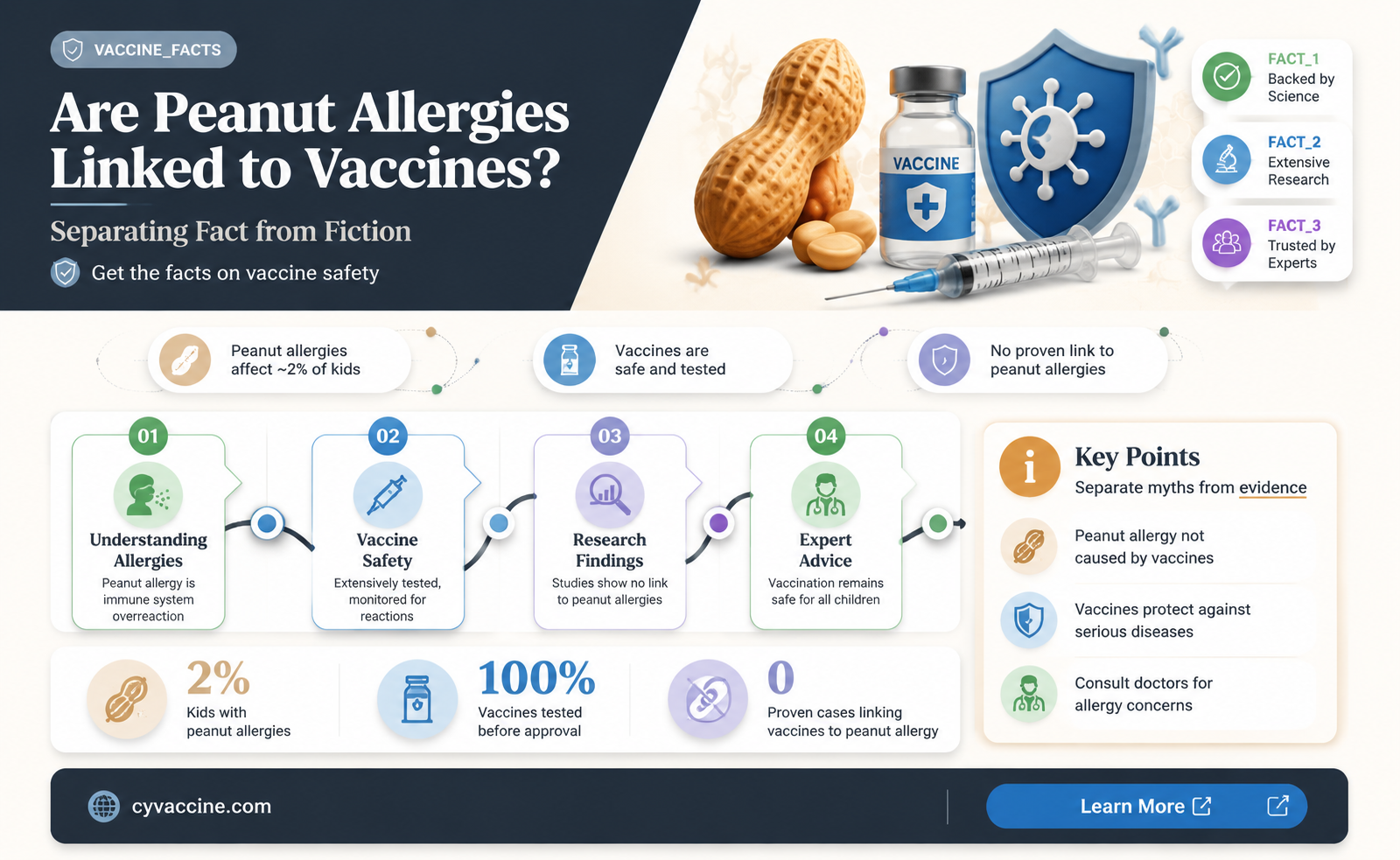
Vaccine Ingredients and Allergens: Do vaccine components like stabilizers or preservatives trigger peanut allergies?
Peanut allergies affect approximately 2% of children in the United States, prompting concerns about potential triggers, including vaccines. While vaccines contain various components like stabilizers and preservatives, none of the ingredients in routine childhood immunizations include peanut proteins or derivatives. Common stabilizers, such as gelatin or lactose, are derived from animal or milk sources, not peanuts. Preservatives like phenol or aluminum adjuvants are chemically synthesized and unrelated to peanut allergens. Despite this, misconceptions persist, fueled by misinformation linking vaccines to food allergies. Understanding the composition of vaccines is crucial for dispelling myths and ensuring informed decision-making.
Analyzing vaccine formulations reveals a strict adherence to safety standards that minimize allergen risks. For instance, the measles, mumps, and rubella (MMR) vaccine uses gelatin as a stabilizer, but it is sourced from pork, not peanuts. Similarly, the influenza vaccine occasionally contains egg proteins, yet peanut components are entirely absent. Regulatory agencies like the FDA and CDC mandate rigorous testing to identify potential allergens, ensuring that vaccines are safe for individuals with peanut allergies. Parents and caregivers should consult healthcare providers for specific concerns, as no scientific evidence supports a causal link between vaccine ingredients and peanut allergies.
A comparative examination of vaccine components and known allergens highlights the absence of peanut-derived substances. Unlike food products, which often carry allergen warnings, vaccines are formulated with non-allergenic stabilizers and preservatives. For example, the aluminum salts used in vaccines as adjuvants enhance immune response without introducing allergenic proteins. Even trace amounts of potential allergens are meticulously avoided during manufacturing. This contrasts with everyday foods, where cross-contamination with peanuts is a common concern. Vaccines, therefore, pose no greater risk of triggering peanut allergies than any other medical product.
Practical steps can help alleviate concerns for parents of children with peanut allergies. First, review the vaccine information sheet provided by healthcare providers, which details all ingredients. Second, discuss any specific allergies with a pediatrician or allergist before vaccination. Third, monitor for rare allergic reactions post-vaccination, though these are typically unrelated to peanut allergens. For example, anaphylaxis from vaccines is extremely rare (approximately 1.3 cases per million doses) and not linked to peanut components. By staying informed and proactive, caregivers can confidently protect their children through vaccination without fearing peanut allergy triggers.
The Discovery of Rabies Vaccine: Louis Pasteur's Lifesaving Breakthrough
You may want to see also
Explore related products





![]()
Immune System Response: Can vaccines alter immune reactions, leading to peanut sensitivity?
The immune system's response to vaccines is a tightly regulated process designed to build immunity without causing harm. Vaccines introduce antigens—harmless components of pathogens—to train the immune system to recognize and combat future threats. This process typically involves the production of antibodies and the activation of immune cells, such as T-cells and B-cells. However, concerns have arisen about whether vaccines might inadvertently alter immune reactions in ways that could lead to sensitivities, such as peanut allergies. While vaccines are rigorously tested for safety, the complexity of the immune system leaves room for questions about rare or unforeseen outcomes.
To understand the potential link between vaccines and peanut sensitivity, it’s crucial to examine how vaccines interact with the immune system. Vaccines primarily stimulate the adaptive immune response, which is specific to the pathogen being targeted. For example, the MMR vaccine triggers the production of antibodies against measles, mumps, and rubella. However, the immune system’s response is not always linear; it can sometimes be influenced by factors like the individual’s genetic predisposition, microbiome, or environmental exposures. Peanut allergies, on the other hand, involve an abnormal reaction by the immune system to peanut proteins, often mediated by Immunoglobulin E (IgE) antibodies. The question arises: could vaccines, by modulating immune responses, inadvertently increase susceptibility to such reactions?
Scientific studies have explored this question, with the majority concluding that there is no direct causal link between vaccines and peanut allergies. For instance, a 2015 study published in *JAMA Pediatrics* found no association between childhood vaccinations and the development of food allergies, including peanut allergies. Similarly, the Centers for Disease Control and Prevention (CDC) emphasizes that vaccines are not a risk factor for food allergies. However, some researchers suggest that the hygiene hypothesis—the idea that reduced early-life exposure to microbes increases allergy risk—could intersect with vaccine effects. Vaccines, by reducing certain infections, might theoretically alter immune development in ways that could influence allergy risk, though this remains speculative and unsupported by robust evidence.
Practical considerations for parents and caregivers include monitoring for allergic reactions after vaccination, though these are extremely rare. Symptoms of an allergic reaction to a vaccine (e.g., hives, swelling, difficulty breathing) typically occur within minutes to hours of administration and require immediate medical attention. Peanut allergies, however, are not a known side effect of vaccines. For children at high risk of peanut allergies, current guidelines recommend early introduction of peanut-containing foods under medical supervision, as this has been shown to reduce allergy risk. Vaccines, in contrast, play no role in this prevention strategy.
In conclusion, while vaccines are a cornerstone of public health, their role in altering immune reactions to cause peanut sensitivity is not supported by current evidence. The immune system’s response to vaccines is distinct from the mechanisms underlying peanut allergies, and no direct causal link has been established. Parents and caregivers should focus on evidence-based strategies for allergy prevention, such as early peanut introduction, while continuing to follow recommended vaccination schedules to protect against infectious diseases. As always, consultation with healthcare providers is essential for personalized advice.
Why Scientists Advocate for Stricter U.S. Vaccine Regulations
You may want to see also
Explore related products





![]()
Epidemiological Studies: Is there a correlation between vaccination rates and peanut allergy prevalence?
The rise in peanut allergies over recent decades has sparked numerous hypotheses, with some suggesting a link to vaccination rates. Epidemiological studies, which examine patterns and causes of health outcomes in populations, have been pivotal in exploring this potential correlation. By analyzing large datasets across different regions and time periods, researchers aim to determine whether vaccination practices might influence the prevalence of peanut allergies. However, establishing causation in such studies is complex, as numerous environmental and genetic factors also play a role.
One approach to investigating this relationship involves comparing peanut allergy rates in populations with varying vaccination coverage. For instance, countries with high vaccination rates, such as the United States or the United Kingdom, have reported increasing peanut allergy prevalence in children under the age of 5. Conversely, regions with lower vaccination rates, like certain parts of Africa or Asia, often exhibit lower peanut allergy incidence. While this observation might suggest a correlation, it is crucial to control for confounding variables, such as dietary habits, hygiene practices, and healthcare access, which differ significantly across these regions.
Another method employed in epidemiological studies is the analysis of temporal trends. Researchers examine whether increases in vaccination rates coincide with rises in peanut allergy diagnoses. For example, the introduction of the Hib vaccine in the 1990s and the subsequent rise in peanut allergies during the same period have been scrutinized. However, such temporal associations do not prove causation. Peanut allergies typically manifest in early childhood, often before the full vaccination schedule is completed, making it unlikely that vaccines directly trigger the allergy. Instead, factors like delayed introduction of peanuts into diets or changes in diagnostic practices may contribute to observed trends.
Practical considerations for parents and healthcare providers include monitoring children for allergic reactions after vaccination, though such reactions are rare and typically unrelated to peanut allergies. The American Academy of Pediatrics recommends introducing peanut-containing foods to infants as early as 4–6 months, particularly those at high risk, to reduce allergy development. This advice underscores the importance of focusing on evidence-based prevention strategies rather than unfounded concerns about vaccines.
In conclusion, while epidemiological studies provide valuable insights into potential correlations between vaccination rates and peanut allergy prevalence, they do not support a causal link. The complexity of allergy development, influenced by genetic predisposition, environmental factors, and dietary practices, necessitates a nuanced understanding. Parents and healthcare providers should prioritize proven strategies for allergy prevention and remain informed by rigorous scientific research.
Shingrix Vaccine Public Availability: A Timeline of Its Release
You may want to see also
Explore related products





![]()
Cross-Reactivity Concerns: Do vaccine antigens cross-react with peanut proteins, causing allergies?
Vaccine antigens are meticulously designed to target specific pathogens, but concerns about cross-reactivity with unrelated proteins, such as those in peanuts, persist. Cross-reactivity occurs when the immune system mistakes a harmless protein for a harmful one due to structural similarities. For instance, some vaccines use adjuvants or carrier proteins that could, in theory, share epitopes with peanut proteins. However, scientific evidence overwhelmingly indicates that such cross-reactivity is extremely rare. The proteins used in vaccines undergo rigorous testing to ensure they do not resemble common allergens, minimizing the risk of unintended immune responses.
Consider the example of the hepatitis B vaccine, which uses a yeast-derived recombinant protein. Studies have shown no increased risk of peanut allergies in vaccinated individuals, despite initial concerns. Similarly, the measles-mumps-rubella (MMR) vaccine, which contains attenuated viruses, has been extensively studied and found to have no association with peanut allergy development. These findings underscore the specificity of vaccine antigens and the immune system’s ability to differentiate between foreign invaders and harmless substances. Parents and caregivers can take reassurance from decades of data confirming the safety of vaccines in this regard.
To address cross-reactivity concerns, vaccine manufacturers adhere to strict guidelines. For example, the FDA requires allergenicity testing for all vaccine components, ensuring they do not contain peanut proteins or cross-reactive substances. Additionally, vaccines are formulated to avoid common allergens, and production facilities are often peanut-free to prevent contamination. For individuals with known severe allergies, healthcare providers may recommend precautions, such as administering vaccines in a medical setting equipped to handle anaphylaxis, though such cases are exceedingly rare.
Practical steps for parents include reviewing vaccine information sheets provided by healthcare providers and discussing any allergy concerns beforehand. Keeping a detailed medical history, including known allergies, ensures informed decision-making. While the theoretical risk of cross-reactivity exists, the actual incidence is negligible compared to the proven benefits of vaccination. By focusing on evidence-based practices, caregivers can confidently protect their children from vaccine-preventable diseases without fear of inducing peanut allergies.
Influenza B Strain Protection: What Vaccines Cover and Why
You may want to see also
Explore related products






![]()
Scientific Evidence Review: What research supports or refutes the vaccine-peanut allergy link?
The notion that vaccines cause peanut allergies has circulated in public discourse, often fueled by misinformation and anecdotal claims. To address this, a rigorous examination of scientific evidence is essential. Research to date has not established a causal link between vaccines and peanut allergies. The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) affirm that vaccines undergo extensive testing for safety and efficacy, with no credible studies linking them to peanut allergies. This lack of evidence underscores the importance of relying on peer-reviewed research rather than unsubstantiated claims.
Analyzing the biological plausibility of a vaccine-peanut allergy link reveals further inconsistencies. Vaccines are designed to stimulate the immune system to recognize and combat pathogens, not to introduce food allergens like peanuts. The ingredients in vaccines, such as adjuvants and stabilizers, are thoroughly tested and do not include peanut proteins. For instance, the MMR vaccine, often scrutinized in this context, contains no peanut derivatives. Scientific consensus maintains that peanut allergies arise from genetic predisposition, immune system dysfunction, and environmental factors, not from vaccination.
A 2015 study published in *The Journal of Allergy and Clinical Immunology* investigated the relationship between childhood vaccinations and food allergies, including peanut allergies. The researchers analyzed data from over 200,000 children and found no significant association between vaccines and the development of food allergies. Similarly, a 2019 review in *Vaccine* concluded that there is no epidemiological evidence supporting a causal relationship between vaccines and peanut allergies. These studies highlight the robustness of scientific inquiry in debunking unfounded claims.
Despite the lack of evidence, misinformation persists, often amplified by social media and anti-vaccine movements. This underscores the need for clear, accessible communication of scientific findings. Healthcare providers play a critical role in educating patients and parents about vaccine safety and the true causes of peanut allergies. Practical steps include discussing the rigorous testing vaccines undergo, emphasizing the absence of peanut proteins in vaccine formulations, and promoting evidence-based resources like the CDC and WHO websites.
In conclusion, the scientific evidence overwhelmingly refutes the claim that vaccines cause peanut allergies. Studies have consistently failed to find a causal link, and biological mechanisms do not support this hypothesis. By focusing on credible research and fostering informed dialogue, we can combat misinformation and ensure public trust in vaccination programs. Parents and caregivers should consult healthcare professionals for accurate information, prioritizing evidence over unfounded fears.
Vaccination Records: Can Businesses Legally Ask for Proof?
You may want to see also
Frequently asked questions
No, there is no scientific evidence to support the claim that vaccines cause peanut allergies. Peanut allergies are primarily due to genetic and environmental factors, not vaccinations.
No, vaccines like the MMR (measles, mumps, rubella) do not contain peanut ingredients. Vaccine components are thoroughly tested and do not include peanuts or peanut-derived substances.
No, vaccine adjuvants (substances that enhance immune response) are not linked to peanut allergies. Extensive research confirms that vaccines are safe and do not contribute to the development of food allergies.