The hepatitis B vaccine schedule in 1990 marked a significant milestone in public health efforts to combat the spread of hepatitis B virus (HBV) infections. During this period, vaccination programs were being established and refined globally, with a focus on high-risk groups such as infants, healthcare workers, and individuals with specific behavioral or occupational risks. The 1990 schedule typically recommended a series of three doses, often administered at 0, 1, and 6 months, to ensure robust immunity against HBV. This era laid the groundwork for widespread hepatitis B vaccination, contributing to a substantial reduction in chronic infections and related complications like liver disease and cancer in subsequent decades.
Explore related products






What You'll Learn
- Vaccine Introduction Timeline: When and where the hepatitis B vaccine was first introduced globally
- Initial Dosing Schedule: Recommended dosage and timing for the hepatitis B vaccine in 1990
- Target Population: Specific groups prioritized for vaccination during the early 1990s
- Vaccine Efficacy Data: Early studies on the effectiveness of the hepatitis B vaccine
- Global Adoption Rates: How quickly countries adopted the hepatitis B vaccine schedule in 1990
![]()
Vaccine Introduction Timeline: When and where the hepatitis B vaccine was first introduced globally
The hepatitis B vaccine's global rollout began in the early 1980s, marking a pivotal moment in the fight against a virus responsible for chronic liver disease and cancer. France was the first country to introduce the vaccine in 1982, initially targeting high-risk groups such as healthcare workers and individuals with multiple sexual partners. This early adoption set the stage for broader implementation, as other countries observed the vaccine's efficacy and safety profile. By the late 1980s, several European nations and the United States had begun integrating the vaccine into their public health programs, though primarily for at-risk populations.
The United States took a significant step in 1991 by recommending universal vaccination for infants, a move that shifted the focus from reactive to preventive care. This decision was influenced by the vaccine's proven effectiveness in clinical trials, which demonstrated over 90% protection against hepatitis B infection. The recommended schedule for infants involved a series of three doses: the first at birth, the second at 1–2 months, and the third at 6–18 months. This timeline ensured robust immunity during early childhood, a critical period for preventing chronic infection.
In contrast, China adopted a more aggressive approach in the early 1990s, implementing a nationwide vaccination program for newborns. This strategy was driven by the country's high prevalence of hepatitis B, with an estimated 9–10% of the population chronically infected. China's program included a birth dose followed by two additional doses at 1 and 6 months, aligning with the World Health Organization's (WHO) recommendations. By 2002, the vaccine had been administered to over 85% of Chinese infants, significantly reducing the disease burden.
Africa, a region heavily affected by hepatitis B, faced challenges in vaccine introduction due to limited resources and infrastructure. However, pilot programs in the late 1990s and early 2000s demonstrated the feasibility of integrating the vaccine into existing immunization schedules. Countries like The Gambia and Uganda led the way, showing that even in resource-constrained settings, high coverage rates could be achieved through community engagement and healthcare worker training. The WHO's endorsement of the vaccine in 1992 as part of the Expanded Program on Immunization (EPI) further accelerated its adoption across the continent.
Practical tips for implementing the hepatitis B vaccine globally include ensuring cold chain maintenance to preserve vaccine potency, training healthcare providers on proper administration techniques, and educating communities about the importance of completing the full dose series. For travelers or individuals in high-risk groups, accelerated schedules (e.g., 0, 1, and 2 months, with a booster at 12 months) can provide rapid protection. Monitoring vaccine coverage and disease incidence through surveillance systems is also crucial for evaluating program impact and identifying gaps.
By the end of the 1990s, the hepatitis B vaccine had become a cornerstone of global health efforts, with over 100 countries incorporating it into their routine immunization programs. This timeline highlights the importance of early adoption, strategic planning, and international collaboration in combating a preventable disease. As of today, the vaccine remains one of the most effective tools in reducing hepatitis B-related morbidity and mortality worldwide.
The Dawn of Vaccines: Tracing Their Origins in the United States
You may want to see also
Explore related products






![]()
Initial Dosing Schedule: Recommended dosage and timing for the hepatitis B vaccine in 1990
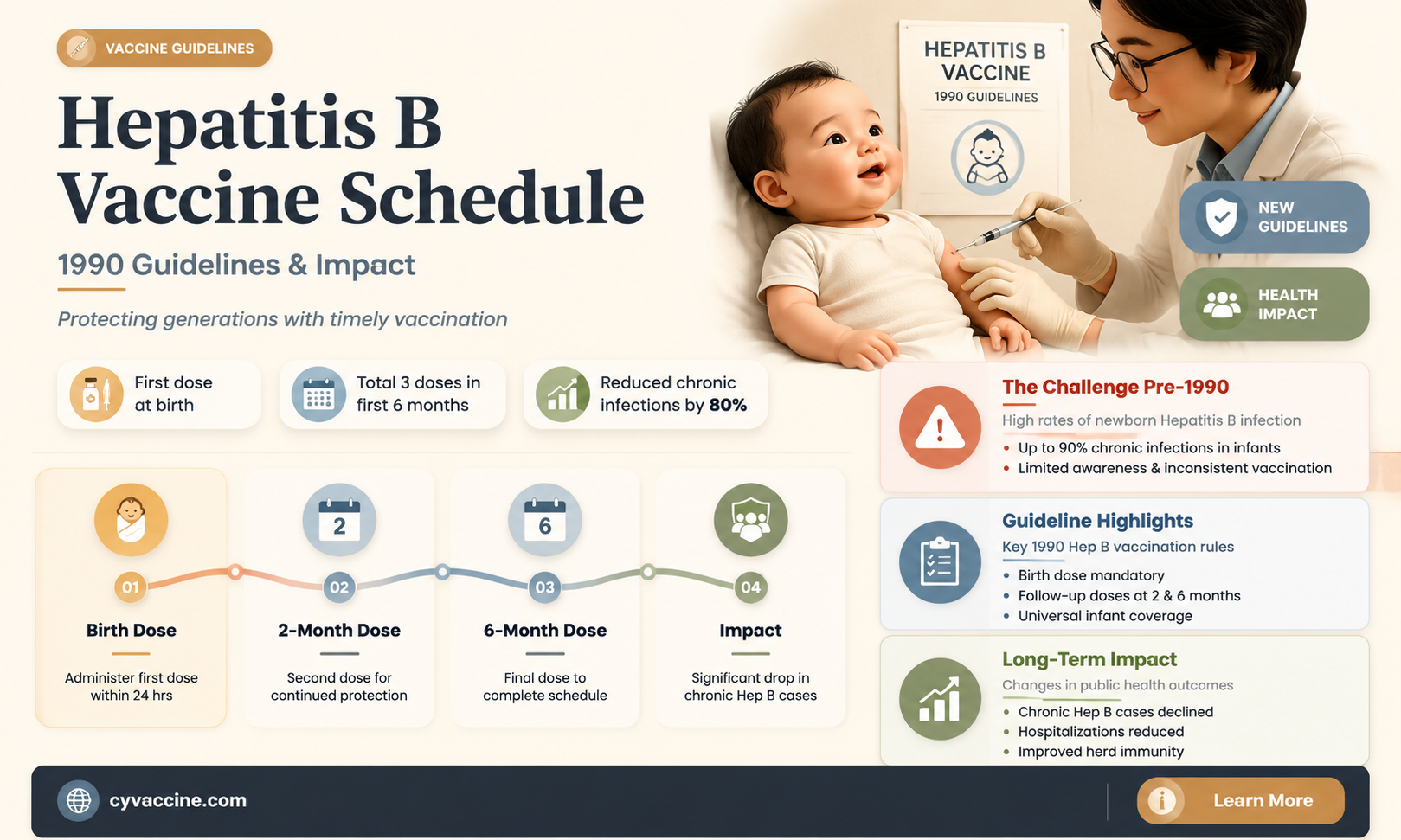
In 1990, the hepatitis B vaccine was a relatively new addition to the immunization landscape, and its dosing schedule reflected the medical community's evolving understanding of the virus and vaccine efficacy. The initial dosing schedule was designed to provide robust protection against hepatitis B, a potentially life-threatening liver infection. For infants born to infected mothers, the recommendation was clear: administer the first dose of the vaccine within 12 hours of birth, followed by two additional doses at 1 month and 6 months of age. This accelerated schedule aimed to prevent perinatal transmission, a critical window for intervention.
For older children and adults, the 1990 guidelines prescribed a three-dose series, typically given at 0, 1, and 6 months. Each dose consisted of 10 micrograms of the recombinant hepatitis B surface antigen protein, delivered intramuscularly. This regimen was based on clinical trials demonstrating that this dosage and timing elicited a strong immune response in over 90% of recipients. Notably, the vaccine was considered safe and well-tolerated, with mild side effects such as soreness at the injection site being the most common complaints.
One key consideration in 1990 was the importance of completing the full vaccine series. Partial vaccination was recognized as less effective in conferring long-term immunity, underscoring the need for adherence to the schedule. Healthcare providers were advised to educate patients about the importance of follow-up doses, particularly the final dose at 6 months, which was crucial for boosting antibody levels. For individuals at high risk of exposure, such as healthcare workers or those with multiple sexual partners, timely completion of the series was non-negotiable.
Practical implementation of the 1990 schedule required careful planning, especially in resource-limited settings. Vaccines needed to be stored at 2°C to 8°C to maintain potency, and healthcare facilities had to ensure consistent supply to avoid delays in dosing. For travelers or individuals with unpredictable schedules, providers often recommended keeping a written record of doses received to facilitate timely completion of the series. Despite these challenges, the 1990 dosing schedule marked a significant step forward in global hepatitis B prevention, laying the groundwork for future refinements in vaccine delivery and policy.
Understanding Post-Vaccination Elderly Deaths: Facts, Risks, and Reassurance
You may want to see also
Explore related products






![]()
Target Population: Specific groups prioritized for vaccination during the early 1990s
During the early 1990s, the hepatitis B vaccine rollout prioritized high-risk groups to maximize impact with limited resources. Healthcare workers topped the list due to their occupational exposure to blood and bodily fluids. This included doctors, nurses, laboratory technicians, and emergency responders. The Centers for Disease Control and Prevention (CDC) recommended a three-dose series, typically administered at 0, 1, and 6 months, to ensure robust immunity. Booster doses were not routinely required for this group unless antibody levels waned over time.
Infants born to hepatitis B-positive mothers were another critical target. Without vaccination, these newborns faced a 90% risk of chronic infection. The CDC mandated a unique schedule for this group: a dose within 12 hours of birth, followed by the standard 1- and 6-month doses. This aggressive approach aimed to block mother-to-child transmission, a leading cause of chronic hepatitis B globally. Pediatricians were instructed to verify maternal hepatitis B status during prenatal care to ensure timely intervention.
Hemodialysis patients and individuals with chronic liver disease were also prioritized due to their heightened susceptibility to infection and severe outcomes. For these groups, the vaccine dosage remained consistent with the general population, but careful monitoring of antibody response was advised. Patients with end-stage renal disease often required higher doses or additional boosters due to immune system compromises. Vaccination clinics in dialysis centers became a practical strategy to streamline access for this vulnerable population.
Men who have sex with men (MSM) and injection drug users were targeted due to behavioral risk factors. Public health campaigns focused on outreach in community settings, such as clinics and harm reduction programs. For MSM, the vaccine was often paired with counseling on safer sex practices. Injection drug users received doses in syringe exchange programs, where staff could also address broader health needs. This dual approach—vaccination plus education—aimed to curb transmission in these high-risk networks.
By focusing on these specific groups, the early 1990s hepatitis B vaccination strategy laid the groundwork for broader immunization efforts. Each population required tailored approaches, from accelerated infant schedules to integrated outreach for at-risk adults. This targeted method not only prevented infections but also reduced the long-term burden of chronic liver disease and hepatocellular carcinoma. Practical tips, such as verifying maternal hepatitis B status and co-locating vaccination services in high-risk settings, remain relevant for modern immunization programs.
Unraveling Anti-Vaccine Protesters' Claims: Myths, Misinformation, and Real Concerns
You may want to see also
Explore related products






![]()
Vaccine Efficacy Data: Early studies on the effectiveness of the hepatitis B vaccine
The hepatitis B vaccine emerged in the late 1970s, but its widespread adoption and rigorous evaluation began in the 1980s. Early studies in the 1980s and early 1990s focused on demonstrating the vaccine’s ability to induce protective antibody levels and prevent infection in high-risk populations. These trials were pivotal in establishing the vaccine’s efficacy and informing the 1990 immunization schedules. For instance, a 1986 study published in *The New England Journal of Medicine* showed that a three-dose series of plasma-derived hepatitis B vaccine provided 95% protection against clinical hepatitis B in gay men, a group at high risk for infection. This laid the groundwork for broader recommendations.
One of the key metrics in early efficacy studies was the seroprotection rate, defined as the proportion of vaccinated individuals achieving an antibody level of ≥10 mIU/mL. Trials consistently demonstrated that a standard three-dose schedule (0, 1, and 6 months) induced seroprotection in over 90% of healthy adults and adolescents. For example, a 1991 study in *Vaccine* reported that 98% of healthcare workers achieved protective antibody levels after completing the series. However, these studies also highlighted variability in response, particularly in older adults and immunocompromised individuals, prompting later research into adjusted dosing or additional boosters.
Pediatric populations were another critical focus of early studies, as preventing perinatal transmission and childhood infection was essential for long-term disease control. A landmark trial in 1987, conducted in Taiwan, demonstrated that vaccinating newborns of hepatitis B surface antigen (HBsAg)-positive mothers, combined with hepatitis B immune globulin (HBIG), reduced chronic infection rates from 38% to 10%. This led to the inclusion of the hepatitis B vaccine in the 1990 childhood immunization schedule, starting with a birth dose followed by doses at 1–2 months and 6–18 months. The success of this strategy in high-prevalence regions underscored the vaccine’s potential to break the cycle of transmission.
Despite the vaccine’s proven efficacy, early studies also identified challenges. For example, a 1990 study in *JAMA* noted that individuals with chronic liver disease or end-stage renal disease had lower seroprotection rates, often requiring higher antigen doses or additional doses. Additionally, concerns about waning immunity emerged, though long-term follow-up studies in the late 1990s would later confirm that protection persisted for at least 15–20 years in most vaccinated individuals. These findings emphasized the need for tailored vaccination strategies and ongoing monitoring.
In summary, early studies on the hepatitis B vaccine’s efficacy provided robust evidence of its effectiveness in preventing infection and chronic disease, particularly in high-risk groups. These findings directly influenced the 1990 vaccination schedules, which prioritized at-risk populations and infants. Practical takeaways from this era include the importance of completing the full three-dose series, the critical role of the birth dose in preventing perinatal transmission, and the need for individualized approaches in immunocompromised individuals. This foundational research not only validated the vaccine’s utility but also set the stage for its global impact in reducing hepatitis B prevalence.
Booster Jab: Am I Fully Vaccinated in the UK?
You may want to see also
Explore related products






![]()
Global Adoption Rates: How quickly countries adopted the hepatitis B vaccine schedule in 1990
By 1990, the hepatitis B vaccine had been available for nearly a decade, yet global adoption rates varied dramatically. High-income countries like the United States and France had already integrated the vaccine into routine childhood immunization schedules, typically starting at birth with a three-dose series (0, 1, 6 months). In contrast, many low- and middle-income countries faced barriers such as cost, infrastructure limitations, and competing public health priorities, delaying widespread implementation. This disparity highlights the complex interplay between economic resources and public health policy in vaccine rollout.
Consider the case of Thailand, a middle-income country that launched a nationwide hepatitis B vaccination program in 1992, just after the 1990 benchmark. The program targeted infants and adolescents, with a catch-up campaign for older children. This swift action was driven by high hepatitis B prevalence and political commitment, demonstrating how local epidemiology and leadership can accelerate adoption. Meanwhile, some African nations, where hepatitis B is endemic, did not introduce the vaccine until the late 1990s or early 2000s, underscoring the challenges of resource-constrained settings.
Analyzing these patterns reveals a critical takeaway: global health initiatives like Gavi, the Vaccine Alliance, which launched in 2000, have since played a pivotal role in closing the adoption gap. By providing financial support and technical assistance, such programs have enabled more countries to adopt the hepatitis B vaccine schedule. However, the 1990 landscape underscores the importance of early investment in vaccine infrastructure and the need for tailored strategies to address regional disparities.
For countries still lagging in hepatitis B vaccination, practical steps include leveraging international partnerships, prioritizing at-risk populations (e.g., healthcare workers and infants), and integrating the vaccine into existing immunization programs. Dosage consistency is key: the standard schedule of three doses (0.5 mL for infants, 1 mL for adolescents/adults) ensures optimal immunity. Monitoring seroconversion rates post-vaccination can also help identify gaps in coverage or vaccine efficacy, ensuring the program’s success.
In retrospect, the 1990 adoption rates of the hepatitis B vaccine serve as a reminder of the persistent global inequities in healthcare access. While progress has been made, the lessons from this era remain relevant today, particularly as new vaccines emerge. Rapid, equitable adoption requires not just scientific innovation but also political will, financial commitment, and a focus on strengthening health systems worldwide.
Joel Osteen's Perspective on Vaccines: Faith, Health, and Responsibility
You may want to see also
Frequently asked questions
In 1990, the typical hepatitis B vaccine schedule involved a series of three doses. The first dose was administered at birth or as soon as possible, followed by a second dose at 1–2 months of age, and a third dose at 6–18 months of age.
Yes, the hepatitis B vaccine was available and recommended for infants in 1990, particularly in high-risk groups or regions with higher prevalence of the disease. However, universal infant vaccination was not yet widely implemented in all countries.
Yes, the schedule for adults in 1990 typically involved three doses administered over a 6-month period (0, 1, and 6 months). This differed from the infant schedule, which was designed to provide protection earlier in life.