The question of whether health care workers are refusing COVID-19 vaccines has sparked significant debate and concern, as these individuals are on the front lines of the pandemic. While the majority of health care workers have been vaccinated, a notable minority in some regions have expressed hesitancy or outright refusal, citing reasons ranging from concerns about vaccine safety and efficacy to personal beliefs or mistrust in the rapid development process. This resistance raises critical issues about patient safety, workplace policies, and public health, as unvaccinated health care workers may pose risks to vulnerable populations and contribute to the spread of the virus. Understanding the motivations behind vaccine refusal and addressing these concerns through education, communication, and supportive policies is essential to increasing vaccination rates within this crucial workforce.
| Characteristics | Values |
|---|---|
| Prevalence of Refusal | Varies widely by region and country. In the U.S., estimates range from 10-30% of healthcare workers initially hesitant or refusing COVID-19 vaccines (as of late 2021/early 2022). |
| Primary Reasons for Refusal | Concerns about vaccine safety, side effects, and long-term effects; mistrust in rapid vaccine development; personal beliefs or misinformation; perceived low risk of severe COVID-19. |
| Demographics | Higher refusal rates among younger healthcare workers, those in long-term care facilities, and certain specialties (e.g., administrative staff vs. physicians). |
| Regional Differences | Higher refusal rates in regions with lower overall vaccination rates or higher vaccine hesitancy (e.g., Southern U.S., parts of Europe). |
| Impact of Mandates | Vaccine mandates in healthcare settings have significantly increased vaccination rates, with compliance often exceeding 90% post-mandate. |
| Professional Consequences | Refusal can lead to job loss, restricted duties, or legal challenges in mandated settings. |
| Public Health Impact | Unvaccinated healthcare workers pose risks to vulnerable patients and contribute to workplace outbreaks. |
| Trends Over Time | Hesitancy has decreased in many areas as more data on vaccine safety and efficacy became available, but pockets of resistance remain. |
| Influencing Factors | Political polarization, social media misinformation, and local cultural attitudes toward vaccines play significant roles. |
| Latest Data (as of 2023) | Most healthcare systems report high vaccination rates (>90%) due to mandates and education, though exact refusal rates vary by source and region. |
Explore related products




$11.93 $21.99


What You'll Learn
![]()
Reasons for refusal among health care workers
Health care workers, despite their proximity to medical information and the realities of disease, are not immune to vaccine hesitancy. A significant portion of this group, often estimated between 10-20% depending on the region and vaccine, express reluctance or outright refusal. This phenomenon warrants scrutiny, as it not only impacts individual health but also undermines public trust in medical institutions.
Understanding the reasons behind this refusal is crucial for developing effective strategies to address concerns and increase vaccination rates within this critical population.
One prominent reason for refusal stems from concerns about vaccine safety and side effects. Health care workers, intimately familiar with medical procedures and potential complications, may scrutinize vaccine data more critically. While clinical trials provide robust evidence of safety, the relatively rapid development and deployment of some vaccines, particularly mRNA-based ones, can fuel anxieties. Specific concerns often revolve around long-term effects, fertility implications, and the potential for rare but severe adverse reactions. Addressing these fears requires transparent communication about the rigorous testing processes, ongoing monitoring systems, and the statistical rarity of serious side effects compared to the risks posed by the diseases themselves.
Providing accessible, evidence-based information tailored to health care workers' level of understanding is paramount.
Historical and systemic distrust also plays a significant role in vaccine refusal among health care workers, particularly within marginalized communities. A legacy of unethical medical experimentation and ongoing healthcare disparities fosters a justified skepticism towards medical institutions. For example, the Tuskegee Syphilis Study, where Black men were deliberately denied treatment, casts a long shadow. Acknowledging this history and actively working to rebuild trust through culturally sensitive communication, diverse representation in clinical trials, and equitable healthcare access is essential.
Engaging community leaders and trusted figures within these communities can help bridge the gap and foster dialogue.
Individual beliefs and personal experiences further contribute to vaccine hesitancy. Some health care workers may hold religious or philosophical objections to vaccination, while others may have had negative experiences with vaccines in the past, either personally or through family members. Respecting individual beliefs while providing accurate information and addressing specific concerns is crucial. Open dialogue, empathy, and personalized risk-benefit discussions can help individuals make informed decisions.
Finally, workplace policies and mandates can inadvertently fuel resistance. While mandates can increase vaccination rates, they can also breed resentment and deepen mistrust. A more nuanced approach, combining education, incentives, and flexible policies that accommodate individual circumstances, may be more effective in the long term. For instance, offering paid time off for vaccination and recovery, providing on-site vaccination clinics, and fostering a culture of open communication can encourage voluntary uptake.
TB Vaccine's Surprising Role in Lowering Melanoma Risk Explained
You may want to see also
Explore related products






![]()
Impact of vaccine hesitancy on patient safety
Vaccine hesitancy among health care workers poses a direct threat to patient safety, particularly in vulnerable populations such as the elderly, immunocompromised individuals, and newborns. When health care workers refuse vaccines, they increase the risk of transmitting preventable diseases to patients. For instance, a study published in *Infection Control & Hospital Epidemiology* found that unvaccinated health care workers were 1.7 times more likely to transmit influenza to patients compared to their vaccinated counterparts. This risk extends beyond influenza to diseases like measles, pertussis, and COVID-19, where outbreaks in health care settings can have devastating consequences.
Consider the practical implications of a health care worker refusing the annual influenza vaccine. Despite the CDC’s recommendation for 100% vaccination rates among health care personnel, compliance often falls short, hovering around 80%. This gap leaves patients exposed, especially in long-term care facilities where residents are often over 65 years old and have weakened immune systems. A single unvaccinated worker can inadvertently introduce the virus, leading to outbreaks that result in severe complications or death. For example, during the 2017-2018 flu season, unvaccinated health care workers were linked to outbreaks in 15% of long-term care facilities, according to the CDC.
To mitigate this risk, health care facilities must implement evidence-based strategies. Mandatory vaccination policies, while controversial, have proven effective in increasing coverage rates. For instance, a 2019 study in *JAMA* showed that hospitals with mandatory flu vaccination policies achieved 98% compliance, compared to 75% in hospitals without such policies. Additionally, offering on-site vaccination clinics and providing education tailored to common concerns—such as debunking myths about vaccine side effects—can improve uptake. For COVID-19 vaccines, addressing hesitancy requires transparent communication about safety data, including the rare but serious risk of myocarditis (approximately 2-10 cases per 100,000 doses in young adults) and its significantly lower risk compared to complications from the disease itself.
Comparatively, countries with higher health care worker vaccination rates, such as France and Italy, have seen fewer health care-associated outbreaks during the COVID-19 pandemic. These nations achieved success through a combination of mandates, incentives, and public health campaigns. In contrast, the U.S., where vaccine hesitancy remains more prevalent, has reported higher rates of health care-associated infections. This disparity underscores the need for a multifaceted approach that balances individual choice with collective responsibility.
Ultimately, vaccine hesitancy among health care workers is not merely a personal decision—it is a patient safety issue. Facilities must prioritize evidence-based interventions, from mandatory policies to targeted education, to protect both workers and patients. By addressing hesitancy head-on, health care systems can reduce the risk of preventable outbreaks and uphold their duty to provide safe, effective care. Practical steps include tracking vaccination rates, offering annual training on vaccine benefits, and ensuring easy access to vaccines during all shifts. The goal is clear: to close the gap between recommendation and action, safeguarding patients in the process.
Are mRNA Vaccines New? A Look at Past Approvals
You may want to see also
Explore related products






![]()
Role of misinformation in vaccine refusal
Misinformation spreads like a virus, exploiting fear and uncertainty to undermine trust in vaccines. Health care workers, despite their medical training, are not immune to its influence. A 2021 study published in *Vaccine* found that 20% of surveyed nurses in the U.S. reported hesitancy toward the COVID-19 vaccine, with concerns about side effects and rushed development fueled by online misinformation. This highlights how even those with medical knowledge can be swayed by false narratives when they tap into existing anxieties.
Consider the "spike protein myth," a persistent piece of misinformation claiming the COVID-19 vaccine causes dangerous spike proteins to circulate in the body. This oversimplification of complex biology, often shared on social media, ignores the fact that spike proteins are a natural part of the immune response and are rapidly cleared by the body. Yet, this myth has been cited by some health care workers as a reason for refusing vaccination, demonstrating how misinformation can distort scientific understanding even among those in the medical field.
Combatting misinformation requires a multi-pronged approach. First, health care institutions must prioritize clear, accessible communication about vaccine safety and efficacy. This includes addressing specific concerns, such as the misconception that mRNA vaccines alter DNA (they do not) or that fertility is affected (extensive studies show no such link). Second, social media platforms need to enforce stricter policies against the spread of false information, flagging and removing content that contradicts established scientific consensus. Finally, health care workers themselves must commit to ongoing education, critically evaluating sources and staying informed about the latest research.
The role of misinformation in vaccine refusal among health care workers is not just a theoretical concern—it has real-world consequences. When those tasked with caring for the sick and vulnerable hesitate to get vaccinated, it erodes public trust and undermines collective immunity efforts. By understanding how misinformation spreads and taking proactive steps to counter it, we can protect both health care workers and the communities they serve.
Understanding Vaccine Composition: Key Components and Their Roles Explained
You may want to see also
Explore related products






![]()
Legal and ethical implications of refusal
Health care workers refusing vaccines raises complex legal and ethical questions that intersect patient safety, individual rights, and public health responsibilities. From a legal standpoint, mandatory vaccination policies for health care workers are increasingly upheld in courts, particularly during public health emergencies. For instance, in *Jacobson v. Massachusetts* (1905), the U.S. Supreme Court affirmed states’ authority to enforce vaccination laws to protect public health. However, such mandates must balance constitutional rights, such as religious exemptions under Title VII of the Civil Rights Act, which requires employers to accommodate sincerely held beliefs unless doing so causes undue hardship. In practice, hospitals like Houston Methodist faced lawsuits in 2021 when employees challenged their vaccine mandate, but courts largely sided with the employer, citing public safety as a compelling interest.
Ethically, the refusal of vaccines by health care workers challenges the principle of nonmaleficence—the duty to “do no harm.” Unvaccinated workers pose a direct risk to vulnerable patients, including immunocompromised individuals and the elderly, who may face severe outcomes from vaccine-preventable diseases. For example, a 2021 study in *The Lancet* found that 20% of COVID-19 cases in hospitals were linked to health care transmission. This raises questions about fiduciary responsibility: does a health care worker’s autonomy to refuse vaccination outweigh their obligation to protect patients? Ethical frameworks like utilitarianism would prioritize collective well-being, while deontological approaches might emphasize individual rights—a tension that institutions must navigate carefully.
Institutionally, hospitals and health systems face practical dilemmas in enforcing vaccine mandates. While termination is a legal option, it risks staffing shortages, particularly in rural or underserved areas. Alternatives like masking, testing, or reassigning unvaccinated workers to non-patient-facing roles are often implemented but may not fully mitigate risk. For instance, the CDC recommends N95 respirators for unvaccinated staff, but compliance and efficacy vary. Employers must also consider the ethical implications of such compromises: does allowing unvaccinated workers to remain employed, even with restrictions, undermine the credibility of public health messaging?
Globally, the legal and ethical landscape varies significantly. In France, health care workers face suspension without pay if unvaccinated, while in Sweden, mandates are rare, relying instead on high voluntary uptake. These differences highlight cultural and systemic factors influencing policy. For example, countries with strong public trust in health institutions, like Denmark, achieve near-universal vaccination rates without coercion. Conversely, in regions with vaccine hesitancy, mandates may provoke backlash, underscoring the need for education and engagement alongside legal measures.
Ultimately, the refusal of vaccines by health care workers demands a nuanced approach that balances legal authority, ethical obligations, and practical realities. Institutions should prioritize transparent communication, offering education and addressing concerns while enforcing policies that protect patients. Legal frameworks must remain adaptable to evolving public health threats, ensuring mandates are proportionate and equitable. Ethically, the profession’s core values of patient welfare and public trust must guide decision-making, even when individual rights are at stake. As vaccines remain a cornerstone of disease prevention, the health care sector’s response to refusal will set precedents for broader public health governance.
Global COVID-19 Vaccines: Availability, Effectiveness, and Worldwide Distribution
You may want to see also
Explore related products






![]()
Strategies to increase vaccine acceptance in health care
Health care workers, despite their medical expertise, are not immune to vaccine hesitancy. Studies show a concerning percentage, ranging from 10% to 30% depending on the region and vaccine type, express reluctance towards receiving recommended vaccinations. This hesitancy poses a significant risk, not only to their own health but also to the vulnerable patients they care for.
Addressing this issue requires a multi-pronged approach that goes beyond simply providing information.
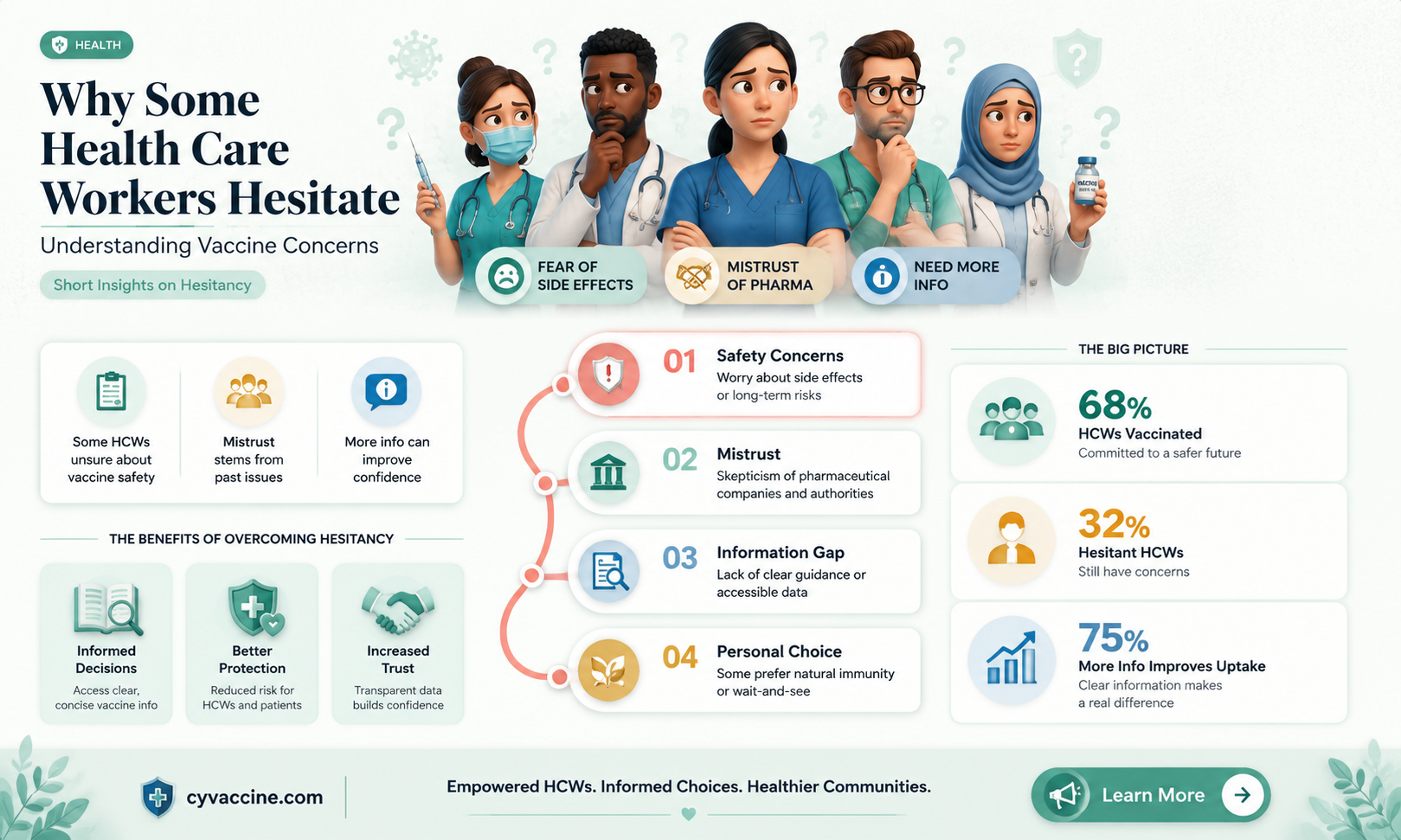
Understanding the "Why" Behind the Hesitancy:
Instead of dismissing concerns as irrational, it's crucial to understand the underlying reasons for vaccine hesitancy among health care workers. Common factors include fear of side effects, mistrust in pharmaceutical companies, and a perceived low personal risk of infection. Some may have experienced historical medical injustices within their communities, fueling skepticism. Others might rely on misinformation circulating online or through social networks. Tailoring interventions requires acknowledging these diverse motivations and addressing them with empathy and evidence-based information.
For instance, addressing fear of side effects could involve transparent communication about common, mild reactions and the rarity of severe adverse events.
Building Trust Through Peer Influence and Leadership:
Health care workers are more likely to accept vaccines when they see their colleagues and respected leaders doing the same. Implementing "vaccine champion" programs, where trusted peers share their positive experiences and address concerns, can be highly effective. Hospital leadership should actively promote vaccination, not just through mandates but by leading by example and openly discussing their own vaccination decisions. Town hall meetings, Q&A sessions with infectious disease specialists, and transparent communication about vaccine safety data can foster trust and encourage open dialogue.
Convenience and Accessibility: Removing Barriers to Action:
Even motivated individuals may face logistical hurdles. Offering on-site vaccination clinics during work hours, providing paid time off for vaccination and potential side effects, and streamlining the registration process can significantly increase uptake. Consider mobile vaccination units for staff working in remote locations or unconventional shifts. Making the process as convenient and hassle-free as possible removes unnecessary barriers and demonstrates organizational commitment to employee well-being.
Beyond Information: Addressing Emotional Concerns:
Simply providing factual information about vaccine efficacy and safety is often insufficient. It's essential to address the emotional aspects of vaccine hesitancy, such as fear, anxiety, and mistrust. One-on-one counseling sessions with trained professionals can provide a safe space for individuals to express their concerns and receive personalized guidance. Utilizing motivational interviewing techniques can help individuals explore their own values and motivations, ultimately leading to informed decision-making.
Daily Global Vaccine Rollout: Tracking Delivery Numbers and Progress
You may want to see also
Frequently asked questions
Yes, some health care workers have refused the COVID-19 vaccine, though the majority have been vaccinated. Reasons for refusal vary and may include concerns about vaccine safety, personal beliefs, or medical conditions.
The percentage varies by region and institution, but studies and reports suggest that refusal rates among health care workers range from 10% to 30%, depending on the location and demographic factors.
Common reasons include skepticism about the vaccine's rapid development, concerns about side effects, personal or religious beliefs, and a perceived low risk of severe illness from COVID-19.
Policies vary by country, state, and employer. Some institutions require vaccination as a condition of employment, while others may allow exemptions for medical or religious reasons, often with additional safety measures like testing or masking.
Unvaccinated health care workers may pose a risk to vulnerable patients, particularly those with weakened immune systems. This has led to concerns about increased transmission in health care settings and has prompted stricter vaccination mandates in many facilities.