The claim that dead babies are in vaccines is a harmful and entirely unfounded conspiracy theory that has been thoroughly debunked by medical and scientific communities. Vaccines are rigorously tested and regulated to ensure safety and efficacy, and their ingredients are transparently disclosed. The myth likely stems from a misunderstanding of fetal cell lines used in the development of some vaccines, such as those for rubella and chickenpox. These cell lines, derived from fetal tissue decades ago, are used in the production process but are not present in the final vaccine product. The use of these cell lines has saved millions of lives by enabling the creation of life-saving vaccines. Spreading misinformation about vaccines not only undermines public trust in science but also endangers public health by discouraging vaccination and increasing the risk of preventable diseases.
What You'll Learn
- Historical Misinformation Origins: Tracing false claims linking vaccines to dead fetal tissue
- Vaccine Development Ethics: Explaining ethical use of fetal cell lines in research
- Scientific Facts vs. Myths: Debunking claims of dead babies in vaccine production
- Religious Concerns Addressed: Clarifying vaccine morality for faith-based objections
- Public Health Impact: How misinformation harms vaccination rates and community health
![]()
Historical Misinformation Origins: Tracing false claims linking vaccines to dead fetal tissue
The origins of misinformation linking vaccines to dead fetal tissue can be traced back to a misunderstanding of the use of fetal cell lines in vaccine development. Certain vaccines, such as those for rubella, hepatitis A, and chickenpox, were developed using cell lines derived from fetal tissue obtained in the 1960s. These cell lines, like WI-38 and MRC-5, have been reproduced in labs for decades and are not directly sourced from new fetal tissue. However, anti-vaccine activists have distorted this scientific process, falsely claiming that vaccines contain "dead babies" or require ongoing fetal tissue harvesting. This misrepresentation exploits public ignorance about cell line cultivation and fuels moral outrage, despite the absence of intact fetal cells in vaccines.
To dissect this false claim, consider the rubella vaccine’s development. In the 1960s, researchers used lung cells from a legally aborted fetus to create the WI-38 cell line, which has since been used to produce the vaccine. The cells were cultured and replicated in a lab, not included in the final vaccine product. Modern doses contain only attenuated viruses and stabilizers, with no fetal tissue. Yet, misinformation campaigns often omit this distinction, conflating the historical origin of cell lines with the vaccine’s composition. This deliberate confusion preys on emotional triggers, such as religious or ethical concerns about abortion, to sow distrust in vaccination programs.
A comparative analysis reveals how this misinformation mirrors historical anti-vaccine narratives. In the 18th century, opponents of smallpox inoculation spread rumors of animal parts being injected into humans. Similarly, the "dead babies" myth taps into primal fears of contamination and moral transgression. Both examples illustrate how scientific processes, when stripped of context, can be twisted into horrifying narratives. Unlike past claims, however, modern misinformation spreads rapidly via social media, amplifying its reach and impact. Understanding this parallel helps explain why such falsehoods persist despite overwhelming scientific evidence to the contrary.
To counter this misinformation, educators and health professionals must focus on clarity and transparency. Start by explaining that fetal cell lines are a tool in vaccine development, not an ingredient. Use analogies, such as comparing cell lines to a recipe’s origin story—the ingredients used today are not the same as those from decades ago. Provide historical context to show how these cell lines have saved millions from diseases like rubella, which once caused severe birth defects. Finally, emphasize ethical safeguards: the original fetal tissue was obtained legally and with consent, and no new tissue is required for ongoing vaccine production. By addressing both scientific and ethical concerns, this approach can disarm the emotional appeal of the false claim.
Practically, parents and caregivers can take steps to verify vaccine information. Always consult reputable sources like the CDC, WHO, or peer-reviewed journals. Be wary of sensationalist language or unverified claims on social media. If unsure, ask a healthcare provider to explain the vaccine’s components and development process. For those with ethical concerns, consider the greater good: vaccines prevent diseases that historically caused widespread harm, including fetal deaths. By focusing on evidence and context, individuals can protect themselves and their communities from the dangers of misinformation.
Polio's Deadly Toll: Pre-Vaccine Era Fatalities Revealed
You may want to see also
![]()
Vaccine Development Ethics: Explaining ethical use of fetal cell lines in research
The development of vaccines often involves the use of fetal cell lines, a practice that has sparked ethical debates and misconceptions, such as the notion that "dead babies are in the vaccine." To clarify, fetal cell lines are not the same as fetal tissue; they are derived from cells taken from elective abortions decades ago and have been replicated in labs ever since. These cell lines, like WI-38 and MRC-5, are used because they are robust and reliable for growing viruses needed in vaccine production. For example, the rubella vaccine, which has prevented millions of congenital rubella syndrome cases, was developed using these cell lines. Understanding this distinction is crucial for addressing ethical concerns while appreciating the life-saving impact of these vaccines.
Ethical considerations in vaccine development using fetal cell lines center on the source of the original cells and the principles of respect for human life. The Catholic Church, for instance, has acknowledged the moral complexity of this issue, stating that while the use of such vaccines is morally acceptable when alternatives are unavailable, individuals should advocate for ethically derived solutions. Researchers and pharmaceutical companies must adhere to strict guidelines, ensuring transparency and informed consent in the original procurement process. This ethical framework balances the duty to prevent disease with the respect for the dignity of human life, even when historical practices raise discomfort.
From a practical standpoint, vaccines like those for hepatitis A, rabies, and chickenpox rely on fetal cell lines during production, but the final product contains no fetal cells or tissue. The cells are used to culture viruses, which are then purified and inactivated or attenuated. For parents administering vaccines to children, it’s important to note that the American Academy of Pediatrics recommends routine immunizations starting at birth, with specific doses tailored to age groups (e.g., the MMR vaccine at 12–15 months and 4–6 years). Understanding the science and ethics behind these vaccines can alleviate concerns and reinforce trust in their safety and necessity.
A comparative analysis highlights the ethical dilemmas in medical research. While fetal cell lines have been indispensable in vaccine development, ongoing efforts aim to find alternatives, such as using animal cells or synthetic biology. However, these methods are not yet as efficient or proven. Until viable alternatives emerge, the ethical use of existing cell lines remains a pragmatic choice, saving millions of lives annually. This underscores the need for continued dialogue between scientists, ethicists, and the public to navigate these complex issues collaboratively.
In conclusion, the ethical use of fetal cell lines in vaccine development is a nuanced issue that requires clarity and empathy. By distinguishing facts from misinformation, acknowledging historical contexts, and promoting transparency, society can uphold both scientific progress and moral principles. For those administering vaccines, such as healthcare providers, emphasizing the rigorous ethical guidelines and the absence of fetal material in the final product can help address concerns. Ultimately, the goal is to protect public health while respecting the values that define humanity.
Post-Vaccine Baby Behavior: What to Expect After 2-Month Shots
You may want to see also
![]()
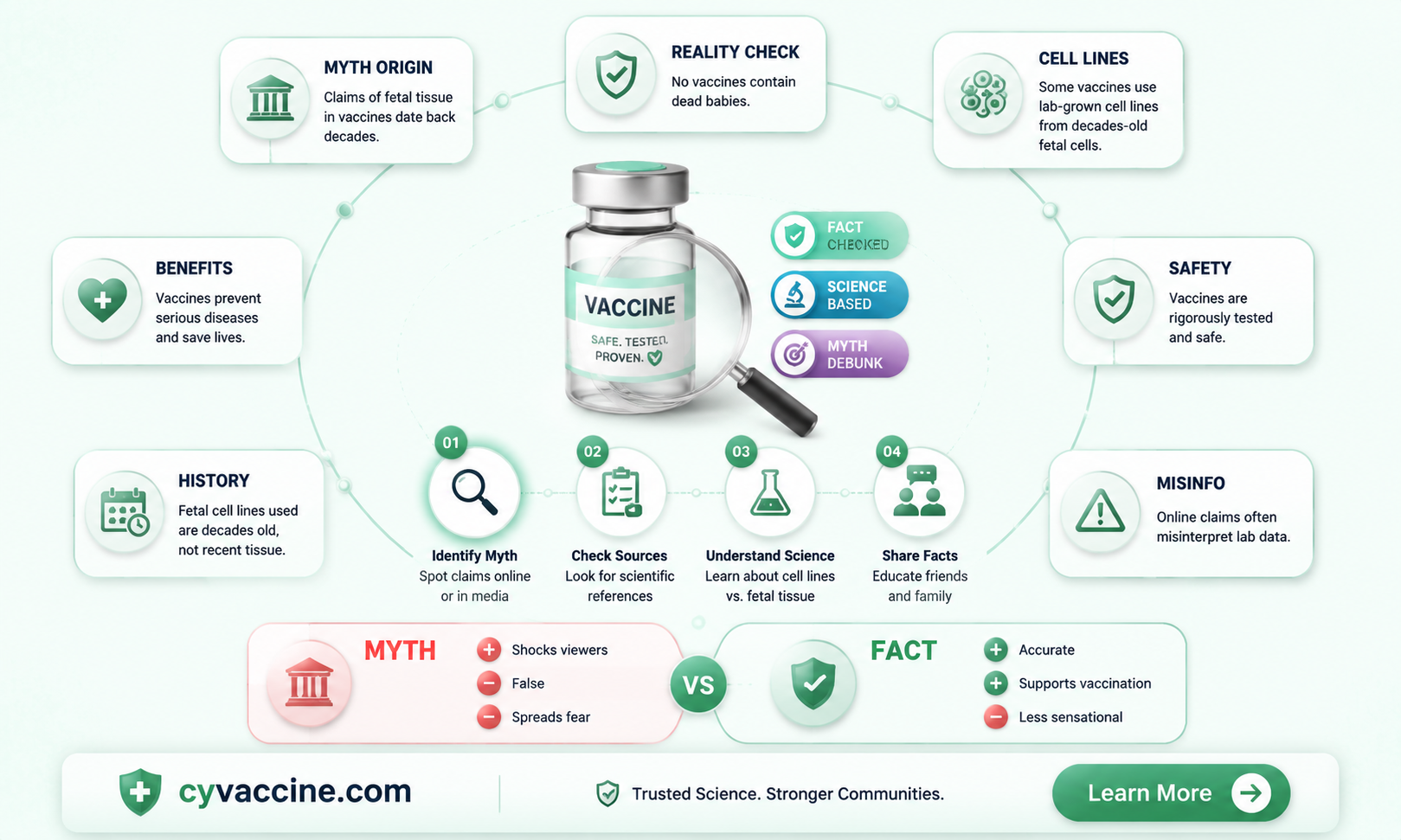
Scientific Facts vs. Myths: Debunking claims of dead babies in vaccine production
Vaccines are rigorously tested and regulated to ensure safety and efficacy, yet misinformation persists, including the disturbing claim that vaccines contain dead babies. This myth often stems from a misunderstanding of fetal cell lines used in vaccine development. To clarify, no vaccines contain dead babies or fetal tissue. Instead, some vaccines, such as those for rubella, hepatitis A, and chickenpox, are produced using cell lines derived from fetal tissue obtained in the 1960s. These cells, which have been replicated in labs for decades, are used to grow viruses for vaccine production. The original fetal tissue is not present in the final vaccine product, and its use has been ethically and scientifically justified to save millions of lives.
Consider the rubella vaccine, a prime example of how fetal cell lines have been instrumental in public health. Before its development, rubella caused severe birth defects and miscarriages. The vaccine, cultivated using the WI-38 cell line (derived from a single fetus in 1964), has nearly eradicated congenital rubella syndrome in many countries. This cell line has been used for over 50 years and is not replenished with new fetal tissue. The Vatican’s Pontifical Academy for Life has even acknowledged the moral acceptability of using such vaccines, emphasizing the greater good of preventing disease. This historical context underscores the scientific necessity and ethical considerations behind these practices.
Debunking the myth requires understanding the difference between fetal tissue and fetal cell lines. Fetal tissue refers to cells directly obtained from a fetus, while fetal cell lines are laboratory-grown cells that have been replicated indefinitely. Vaccines do not contain whole cells or tissue fragments from fetuses; they use purified components of viruses grown in these cell lines. For instance, the hepatitis A vaccine contains inactivated virus particles, not fetal cells. Regulatory bodies like the FDA and WHO ensure that vaccines meet strict purity standards, confirming that no fetal material remains in the final product. This distinction is critical in addressing misinformation.
Practical steps can help individuals discern fact from fiction. First, verify claims by consulting reputable sources such as the CDC, WHO, or peer-reviewed journals. Second, understand that vaccine production involves complex processes designed to eliminate contaminants, including any residual cells. Third, recognize the historical and ethical frameworks that govern the use of fetal cell lines, which prioritize public health while respecting moral concerns. By focusing on scientific evidence and regulatory oversight, individuals can confidently separate myths from reality and make informed decisions about vaccination.
Finally, the claim of "dead babies in vaccines" is a harmful misconception that undermines trust in life-saving medical interventions. It exploits emotional sensitivities to spread fear and distrust. In contrast, the scientific community’s transparent use of fetal cell lines highlights a commitment to both ethical standards and public health. Vaccines remain one of the most effective tools in preventing disease, and understanding their production processes is essential to combating misinformation. By embracing scientific facts, society can protect itself from both disease and the dangers of unfounded myths.
Unveiling Vaccines' Role in Boosting Human Immune System Activation
You may want to see also
![]()
Religious Concerns Addressed: Clarifying vaccine morality for faith-based objections
The misconception that vaccines contain dead babies stems from a twisted interpretation of fetal cell lines used in vaccine development. Some vaccines, like those for rubella and hepatitis A, were historically cultivated using cells descended from elective abortions decades ago. These cells, not fetal tissue, are used to grow viruses for vaccines, ensuring safety and efficacy. Understanding this distinction is crucial for faith-based communities concerned about the sanctity of life.
From a moral standpoint, religious leaders and ethicists often differentiate between direct involvement in abortion and indirect, distant associations. The Vatican, for instance, has stated that using such vaccines is morally acceptable when no alternative exists, as refusing vaccination could pose greater risks to public health. This perspective emphasizes the principle of remote cooperation, where the intent and proximity to the act matter. For parents, this means vaccinating children aligns with protecting life, a core tenet of many faiths.
Practical steps can help faith-based communities navigate these concerns. First, consult trusted religious authorities who understand both theological principles and scientific facts. Second, research vaccine-specific details; not all vaccines use fetal cell lines, and alternatives often exist. Third, advocate for ethical advancements in vaccine research, such as synthetic cell lines, to address future concerns. Finally, frame vaccination as an act of love and stewardship, safeguarding vulnerable populations in line with religious teachings.
Comparing this issue to other faith-based dilemmas, such as organ donation or blood transfusions, reveals a pattern: many religious communities adapt their interpretations to balance doctrine with compassion. Vaccination, like these practices, can be viewed as a moral imperative to protect life. By focusing on the greater good and seeking informed guidance, faith-based objections can be addressed with clarity and empathy, ensuring both spiritual and physical well-being.
Understanding mRNA Vaccines: Spike Protein Production and Its Impact
You may want to see also
![]()
Public Health Impact: How misinformation harms vaccination rates and community health
Misinformation about vaccines, such as the baseless claim that "dead babies are in vaccines," directly undermines public trust in life-saving immunizations. This specific myth, often tied to the use of fetal cell lines in vaccine development, exploits emotional triggers to spread fear. Historically, vaccines like the rubella vaccine were developed using cells derived from a terminated pregnancy in the 1960s. These cells, replicated in labs, have no connection to "dead babies" in vaccines today. Yet, this distortion persists, fueling hesitancy and reducing vaccination rates, particularly among parents of children under 5, a critical age for immunizations like MMR (measles, mumps, rubella).
Consider the measles outbreak in 2019, where communities with low MMR vaccination rates saw infection rates spike to 1,282 cases nationwide. Misinformation campaigns linking vaccines to moral or safety concerns created pockets of vulnerability. For instance, a single dose of MMR vaccine is 93% effective, and two doses raise protection to 97%. However, when vaccination rates drop below 95%, herd immunity falters, exposing infants too young to be vaccinated and immunocompromised individuals. The spread of misinformation thus transforms isolated skepticism into a public health crisis, turning preventable diseases into resurging threats.
To combat this, public health strategies must address misinformation at its root. First, clarify the science: fetal cell lines (e.g., WI-38, MRC-5) are used in production for vaccines like chickenpox and hepatitis A, but no fetal tissue is present in the final product. Second, engage trusted messengers—pediatricians, community leaders, or religious figures—to debunk myths with empathy, not condescension. For example, a study found that parents were 20% more likely to vaccinate when informed by a pediatrician who acknowledged concerns while providing factual reassurance. Third, leverage data visualization tools to show the correlation between declining vaccination rates and disease outbreaks, making abstract risks tangible.
However, caution is necessary. Overcorrecting misinformation with excessive technical detail can overwhelm audiences. Instead, focus on actionable takeaways: emphasize the safety profile of vaccines (e.g., the MMR vaccine has been administered safely to over 500 million children globally) and the real-world consequences of skipping doses. For parents of newborns, stress the importance of timely vaccinations—the first dose of DTaP (diphtheria, tetanus, pertussis) is given at 2 months, with boosters at 4 and 6 months, to build immunity during peak vulnerability. Misinformation thrives in ambiguity; clarity and specificity are its antidote.
Ultimately, the harm of vaccine misinformation extends beyond individual choices—it fractures community health. When myths like "dead babies in vaccines" take hold, they erode collective immunity, endangering the most vulnerable. Public health efforts must bridge the gap between scientific fact and emotional narrative, using storytelling and data to rebuild trust. For instance, sharing testimonials of families protected by vaccines or highlighting historical successes (e.g., smallpox eradication) can humanize the impact of immunization. In this battle, accuracy alone is not enough; it must be paired with compassion and strategic communication to safeguard both individuals and communities.
Whooping Cough Vaccine: Duration of Protection and Booster Needs
You may want to see also
Frequently asked questions
No, there are no dead babies in vaccines. This is a misinformation claim that has been thoroughly debunked by scientific and medical authorities.
The rumor often stems from misinformation campaigns, conspiracy theories, or misinterpretations of vaccine ingredients. Vaccines are rigorously tested and regulated to ensure safety.
Some vaccines are produced using cell lines derived from fetal tissue obtained decades ago. However, the vaccines themselves do not contain fetal tissue or cells. These cell lines are used in the manufacturing process and are safe.
The use of fetal cell lines in vaccine production is a complex ethical issue. Many religious and ethical organizations, including the Vatican, have stated that receiving such vaccines is morally acceptable, as the original source was from decades ago and the vaccines save lives.