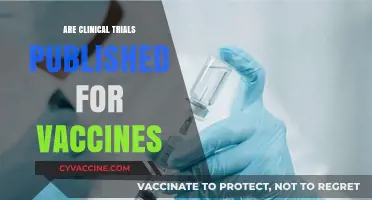
The question of whether children are vaccinated against smallpox today is an important one, rooted in the disease's historical impact and its eradication. Smallpox, a devastating and often fatal illness caused by the variola virus, was declared eradicated by the World Health Organization (WHO) in 1980, thanks to a global vaccination campaign. As a result, routine smallpox vaccination for the general public, including children, was discontinued in the early 1970s in most countries. However, the vaccine is still maintained in limited quantities for emergency use, such as in the event of a bioterrorism threat. Today, children are not routinely vaccinated against smallpox, as the disease no longer exists in the wild, and the risks associated with the vaccine outweigh the benefits for the general population.
| Characteristics | Values |
|---|---|
| Current Vaccination Status | No, children are not routinely vaccinated against smallpox. |
| Reason for Discontinuation | Smallpox was eradicated globally in 1980, leading to vaccine cessation. |
| Last Routine Vaccination Year | Most countries stopped routine smallpox vaccination by the early 1970s. |
| Current Vaccine Availability | Smallpox vaccines are stockpiled for emergency use only. |
| Target Population for Stockpiled Vaccines | High-risk groups (e.g., lab workers, first responders) in case of bioterrorism. |
| Global Eradication Year | 1980, certified by the World Health Organization (WHO). |
| Vaccine Types Stockpiled | First-generation (e.g., Dryvax) and third-generation (e.g., ACAM2000) vaccines. |
| Immunity in Younger Generations | No natural immunity; smallpox vaccination is no longer part of childhood immunization schedules. |
| Public Health Focus | Surveillance and preparedness for potential re-emergence or bioterrorism threats. |
Explore related products






What You'll Learn
- Current smallpox vaccination policies for children in different countries
- Historical smallpox vaccination practices and their effectiveness in children
- Reasons smallpox vaccination is no longer routine for children today
- Risks and benefits of smallpox vaccination in pediatric populations
- Smallpox vaccine availability for children in case of outbreaks
![]()
Current smallpox vaccination policies for children in different countries
Smallpox, a disease eradicated in 1980, no longer requires routine vaccination for children in most countries. The World Health Organization (WHO) ceased global smallpox vaccination campaigns in 1980, as the virus no longer circulates naturally. However, the legacy of smallpox vaccination policies persists, and a few nations maintain stockpiles of the vaccine for emergency preparedness. This raises the question: how do current policies address smallpox vaccination for children in different countries?
In the United States, the Centers for Disease Control and Prevention (CDC) does not recommend routine smallpox vaccination for the general public, including children. The vaccine, known as ACAM2000, is reserved for specific high-risk groups, such as laboratory workers handling the virus or military personnel. For children, vaccination is only considered in the event of a confirmed smallpox outbreak or bioterrorism threat. Parents should note that the smallpox vaccine contains a live virus (vaccinia), which can cause serious side effects, including a progressive and potentially fatal rash called progressive vaccinia, particularly in immunocompromised individuals.
Contrastingly, some countries adopt a more precautionary approach. Russia, for instance, maintains a strategic reserve of smallpox vaccine and has occasionally vaccinated military personnel and laboratory workers. While children are not routinely vaccinated, the infrastructure exists to rapidly deploy the vaccine if needed. Similarly, India, which played a significant role in the global eradication effort, retains a stockpile of smallpox vaccine but does not administer it to children under normal circumstances. These policies reflect a balance between preparedness and the risks associated with the vaccine.
In Europe, smallpox vaccination policies are largely harmonized under the guidance of the European Centre for Disease Prevention and Control (ECDC). No European country routinely vaccinates children against smallpox. However, many nations, including the United Kingdom and Germany, store smallpox vaccine doses as part of their national security strategy. In the UK, the vaccine is held at the National Emergency Stockpile and would only be used in the event of a confirmed outbreak. Parents in these regions should be aware that smallpox vaccination for children is not a standard practice but could be implemented in emergency scenarios.
A notable exception to the global trend is the ongoing debate about smallpox vaccination in the context of bioterrorism. Countries like the United States and Canada have explored the idea of vaccinating select populations, including children, in high-risk areas following a bioterrorist attack. However, such measures are highly controversial due to the vaccine’s side effects and the low probability of a smallpox resurgence. For parents, understanding these policies underscores the importance of staying informed about public health advisories and emergency protocols in their respective countries.
In summary, current smallpox vaccination policies for children vary widely but are consistently rooted in the disease’s eradication and the vaccine’s risks. Routine vaccination is obsolete, yet strategic stockpiles and emergency plans remain in place in many countries. Parents should familiarize themselves with their nation’s specific policies, particularly in regions with heightened security concerns, to ensure they are prepared for any unforeseen developments.
Understanding Vaccine-Induced Immunity: Active, Passive, or Adaptive?
You may want to see also
Explore related products






![]()
Historical smallpox vaccination practices and their effectiveness in children
Smallpox vaccination in children has a storied past, marked by evolving practices and significant milestones. The earliest smallpox vaccines, introduced in the late 18th century, were administered via arm-to-arm inoculation, where lymph fluid from a vaccinated individual was transferred to the arm of another. This method, while groundbreaking, carried risks of transmitting other diseases and was often inconsistent in its effectiveness. Children, typically vaccinated between the ages of 3 months and 2 years, were particularly vulnerable to complications due to their developing immune systems. Despite these challenges, early vaccination efforts laid the foundation for global eradication campaigns.
By the mid-20th century, the introduction of the lymph-based vaccine and later the freeze-dried vaccine standardized smallpox vaccination practices. The recommended dosage for children was 0.04 mL of reconstituted vaccine, administered via multiple punctures using a bifurcated needle. This method ensured a reliable immune response in over 95% of recipients. Mass vaccination campaigns targeted children as a priority group, as they were both highly susceptible to smallpox and effective in building herd immunity. Historical data from these campaigns demonstrated that vaccinated children experienced significantly lower mortality rates compared to unvaccinated populations, with protection lasting up to 10 years before a booster was needed.
However, smallpox vaccination in children was not without risks. Post-vaccination complications, such as progressive vaccinia or eczema vaccinatum, were more common in younger age groups, particularly those with compromised immune systems. To mitigate these risks, contraindications were established, excluding children with severe eczema or immunodeficiencies from vaccination. Public health strategies also emphasized post-vaccination care, including keeping the vaccination site clean and monitoring for adverse reactions. These precautions ensured that the benefits of vaccination outweighed the risks for the majority of children.
Comparing historical smallpox vaccination practices to modern immunization programs highlights both progress and enduring principles. While smallpox vaccination focused on a single disease, today’s childhood immunization schedules address multiple pathogens. However, the success of smallpox eradication underscores the importance of targeted, age-specific strategies and global collaboration. Historical practices also remind us of the need for rigorous safety monitoring and public trust, lessons that remain relevant in contemporary vaccine development and deployment.
In conclusion, historical smallpox vaccination practices in children were a cornerstone of the disease’s eradication, combining scientific innovation with practical public health measures. The effectiveness of these efforts was evident in reduced morbidity and mortality rates among vaccinated populations, particularly children. While smallpox vaccination is no longer necessary today, its legacy informs current strategies for preventing infectious diseases, emphasizing the critical role of early childhood immunization in global health.
Understanding the Feline Ultranasal FVRCP Vaccine: Benefits and Uses
You may want to see also
Explore related products






![]()
Reasons smallpox vaccination is no longer routine for children today
Smallpox vaccination is no longer part of routine childhood immunizations, a stark contrast to its historical status as a cornerstone of public health. This shift is primarily due to the eradication of smallpox, declared by the World Health Organization (WHO) in 1980. The last known natural case occurred in 1977, rendering the vaccine unnecessary for the general population. Unlike vaccines for measles or polio, which target persistent threats, smallpox vaccination serves no preventive purpose today. This eradication success story highlights the power of global vaccination campaigns but also underscores the logic of discontinuing a vaccine when its target disease no longer exists.
From a practical standpoint, the smallpox vaccine carries risks that outweigh its benefits in a disease-free world. The vaccine, known as the Dryvax or ACAM2000, uses a live virus called vaccinia, which is related to smallpox. While effective, it can cause severe side effects, including a painful lesion at the injection site, fever, and, in rare cases, life-threatening conditions like encephalitis or myocarditis. For children, whose immune systems are still developing, these risks are particularly concerning. Modern vaccine strategies prioritize safety, especially when the disease itself is no longer a threat, making smallpox vaccination an unacceptably risky choice for routine use.
Another critical factor is the shift in public health priorities. With smallpox eradicated, resources are now allocated to combating active threats like COVID-19, influenza, and measles. Routine smallpox vaccination would divert attention and funding from these pressing issues. Additionally, the smallpox vaccine’s unique administration method—a pronged needle that delivers the vaccine through the skin—requires specialized training, making it impractical for widespread use. This logistical challenge, combined with the vaccine’s side effects, further justifies its exclusion from childhood immunization schedules.
Finally, smallpox vaccination is reserved for specific high-risk groups, such as laboratory workers handling the virus and military personnel who might face bioterrorism threats. For these individuals, the benefits of protection outweigh the risks. However, children in the general population face no such risks, eliminating the need for vaccination. This targeted approach ensures that the vaccine is used efficiently, without exposing unnecessary individuals to its potential harms. In a world free of smallpox, this strategy strikes the right balance between preparedness and prudence.
CVS Vaccine Clinics: Exploring Three Types for Community Health
You may want to see also
Explore related products






![]()
Risks and benefits of smallpox vaccination in pediatric populations
Smallpox vaccination in children is no longer routine, as the disease was declared eradicated in 1980. However, the question of vaccinating pediatric populations remains relevant due to bioterrorism concerns and emerging research on vaccine safety and efficacy in younger age groups. The smallpox vaccine, known as the Vaccinia virus vaccine, has been studied in children as young as 2 years old, with dosages typically ranging from 0.0025 mL to 0.005 mL administered via scarification. While the vaccine has proven effective in preventing smallpox, its use in children must be carefully weighed against potential risks, including rare but severe adverse events.
Analytical Perspective:
The benefits of smallpox vaccination in children are clear in a hypothetical outbreak scenario. The vaccine provides robust immunity, with studies showing seroconversion rates exceeding 90% in pediatric populations. However, the risk-benefit calculus shifts when considering the vaccine’s side effects. Common reactions include fever, fatigue, and a localized lesion at the vaccination site. More concerning are rare complications such as postvaccinial encephalitis, which occurs in approximately 1 in 100,000 vaccine recipients, and progressive vaccinia, a severe condition more likely in immunocompromised individuals. For healthy children, the risks may outweigh the benefits in the absence of an active threat, but stockpiling the vaccine and understanding its pediatric application remain critical for public health preparedness.
Instructive Approach:
If smallpox vaccination becomes necessary for children, healthcare providers must follow specific protocols. The vaccine is administered using a bifurcated needle, with 15 jabs into the skin of the upper arm. Parents should monitor children for signs of adverse reactions, such as persistent fever, confusion, or severe skin lesions, and seek immediate medical attention if these occur. Immunocompromised children, including those with eczema or HIV, should not receive the vaccine due to heightened risks. Post-vaccination care includes keeping the vaccination site clean and covered to prevent transmission of the vaccinia virus to others, particularly vulnerable populations.
Persuasive Argument:
While smallpox vaccination carries risks, the potential consequences of a smallpox resurgence far outweigh these concerns. Historical data show that smallpox had a mortality rate of 30% in unvaccinated populations, with children being particularly vulnerable. In a bioterrorism scenario, vaccinating children could be a critical component of containment strategies. Advances in vaccine technology, such as the development of attenuated vaccinia strains, may further reduce risks in the future. Public health officials must balance caution with the imperative to protect the most susceptible age groups, ensuring that vaccination campaigns are both safe and effective.
Comparative Analysis:
Compared to other childhood vaccines, the smallpox vaccine presents unique challenges. Unlike the measles or polio vaccines, which are routinely administered with minimal risk, the smallpox vaccine’s side effect profile necessitates stricter eligibility criteria. For instance, the MMR vaccine has a risk of severe allergic reaction in approximately 1 in 1 million doses, whereas the smallpox vaccine’s risk of life-threatening complications is significantly higher. However, the context of use differs—MMR is given universally, while smallpox vaccination is reserved for specific threats. This comparison underscores the need for tailored public health strategies that account for both disease severity and vaccine safety.
Practical Takeaway:
For parents and healthcare providers, understanding the risks and benefits of smallpox vaccination in children is essential for informed decision-making. While routine vaccination is not recommended, familiarity with the vaccine’s administration, dosage, and potential complications is crucial for emergency preparedness. Public health agencies should continue to educate communities about smallpox vaccination, emphasizing its role as a last line of defense rather than a routine preventive measure. In the absence of an immediate threat, the focus should remain on maintaining vaccine stockpiles and advancing research to improve safety for pediatric populations.
Is Asking About Vaccination Status a HIPAA Violation?
You may want to see also
Explore related products






![]()
Smallpox vaccine availability for children in case of outbreaks
Routine smallpox vaccination for children ceased in the United States in 1972, following the global eradication of the disease declared by the World Health Organization (WHO) in 1980. Today, smallpox vaccination is not part of the standard childhood immunization schedule in any country. However, the question of smallpox vaccine availability for children in case of outbreaks remains critical due to the potential bioterrorism threat. The U.S. Strategic National Stockpile (SNS) maintains a supply of the ACAM2000 vaccine, a second-generation smallpox vaccine licensed by the FDA in 2007. In the event of an outbreak, this stockpile could be rapidly deployed to protect both adults and children, though specific guidelines for pediatric use are limited.
Administering smallpox vaccines to children during an outbreak requires careful consideration of dosage and safety. The ACAM2000 vaccine is approved for individuals aged 18 and older, but in emergency situations, it could be used off-label for younger age groups under the guidance of public health authorities. The standard dose is 0.0025 mL, delivered via a bifurcated needle in a scarification technique. For children, the same dose would likely apply, but monitoring for adverse effects such as myopericarditis or progressive vaccinia would be essential, as these risks are higher in immunocompromised individuals or those with certain skin conditions. Parents and caregivers should be educated about post-vaccination care, including keeping the vaccination site clean and covered to prevent transmission of the vaccinia virus.
Comparatively, the older Dryvax vaccine, used during the eradication campaign, had a higher incidence of side effects, which is why ACAM2000 is preferred today. However, neither vaccine has been extensively studied in pediatric populations, creating a knowledge gap in outbreak scenarios. Historical data suggest that children generally tolerate smallpox vaccines well, but modern surveillance systems would need to be activated to track outcomes in real time. In contrast to routine childhood vaccines, smallpox vaccination during an outbreak would be a reactive measure, prioritizing speed and coverage over long-term safety data.
Practically, public health officials would need to implement targeted communication strategies to address parental concerns and ensure compliance. This includes clarifying that the vaccine’s benefits outweigh the risks in an outbreak setting and providing clear instructions for recognizing and managing side effects. Schools and pediatric healthcare providers would play a central role in distribution, potentially using drive-through clinics or mobile units to vaccinate large numbers of children quickly. Collaboration with international health organizations would also be crucial, as a smallpox outbreak in one region could rapidly become a global crisis.
In conclusion, while smallpox vaccination is not routine for children, preparedness for potential outbreaks involves maintaining vaccine stockpiles, developing age-appropriate protocols, and ensuring rapid deployment capabilities. The focus must be on balancing urgency with safety, leveraging historical knowledge while adapting to modern challenges. Parents, healthcare providers, and policymakers must remain informed and ready to act decisively to protect children in the face of this rare but grave threat.
India's Chickenpox Vaccine: A Timeline of Its Introduction and Impact
You may want to see also
Frequently asked questions
No, children are not routinely vaccinated against smallpox because the disease was declared eradicated globally in 1980, and vaccination ceased in most countries by the 1970s.
Children are not vaccinated against smallpox because the virus no longer exists in the wild, and the risks of the smallpox vaccine (such as side effects) outweigh the benefits in the absence of the disease.
Yes, stockpiles of the smallpox vaccine are maintained by governments and organizations like the WHO for emergency use in case of a bioterrorism event or accidental release of the virus.
No, children (or anyone) cannot receive the smallpox vaccine for routine travel purposes, as it is not administered unless there is a specific, verified threat of smallpox exposure.
While newer, safer smallpox vaccines have been developed (e.g., ACAM2000 and JYNNEOS), they are not administered to children unless there is a confirmed smallpox threat, as the disease is eradicated.