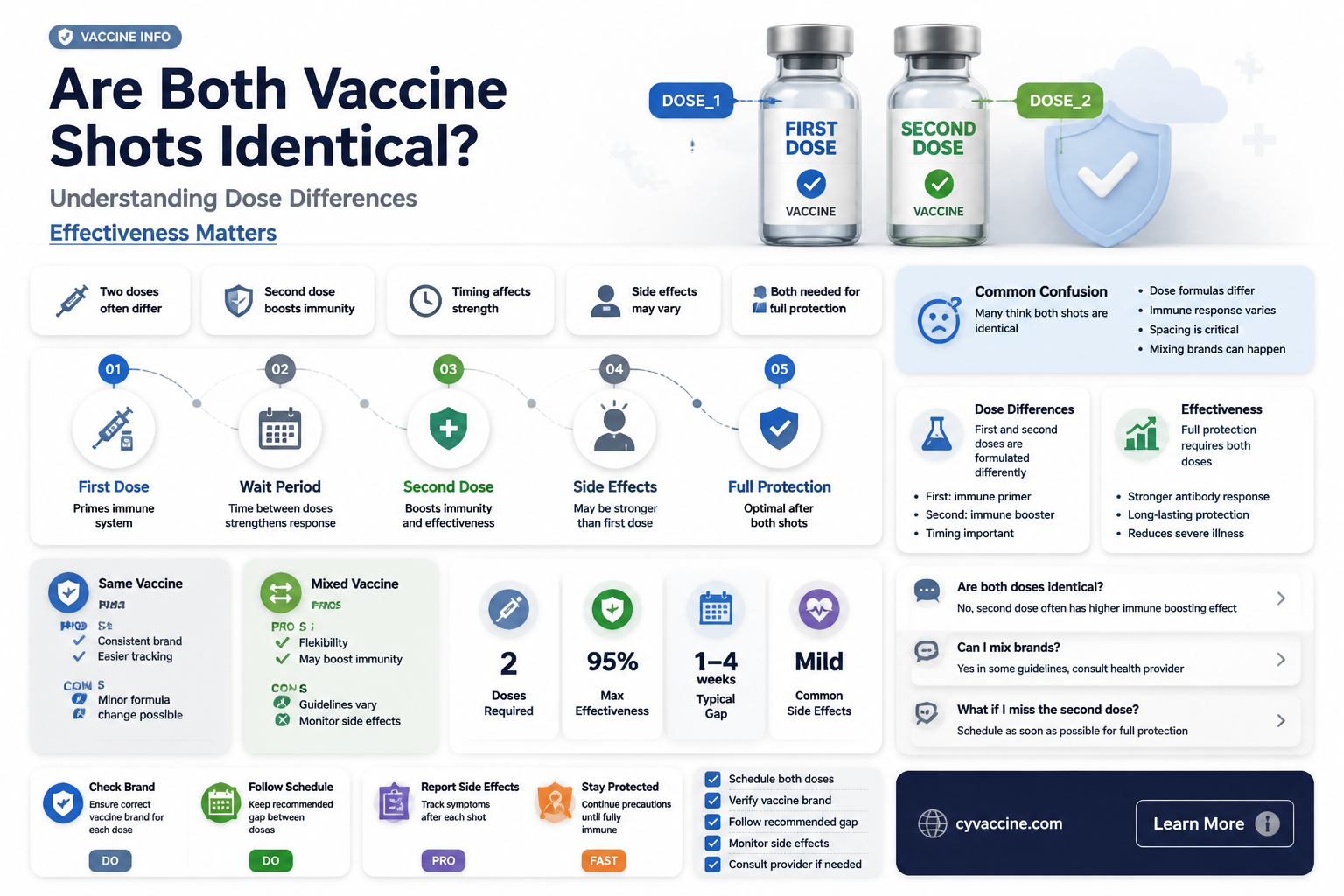
When considering whether both doses of a vaccine are the same, it’s important to understand that while many vaccines use identical formulations for each shot, some may vary based on the vaccine type or manufacturer’s design. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna typically administer the same dose in both shots, while others, such as the Oxford-AstraZeneca vaccine, may use the same formulation but focus on boosting the immune response. Additionally, some vaccines, like Novavax, might have slight differences in composition or dosage between doses. The consistency or variation between shots is carefully determined during clinical trials to ensure optimal safety and efficacy, and following the recommended schedule is crucial for achieving full protection. Always consult healthcare providers or official guidelines for specific information about the vaccine you’re receiving.
Explore related products






What You'll Learn
- Vaccine Composition: Do both doses contain identical ingredients, or are there variations in formulation
- Dosage Strength: Is the amount of active substance the same in both vaccine shots
- Manufacturer Consistency: Are both doses produced by the same manufacturer or different ones
- Immune Response: Does each shot trigger the same level of immune system activation
- Interval Impact: Does the time gap between doses affect their composition or effectiveness
![]()
Vaccine Composition: Do both doses contain identical ingredients, or are there variations in formulation?
The COVID-19 vaccines authorized for emergency use or approved by regulatory bodies like the FDA and EMA typically consist of two doses for the Pfizer-BioNTech and Moderna mRNA vaccines, and one or two doses for the AstraZeneca and Johnson & Johnson vaccines. A common question arises: are the ingredients in both doses identical, or do they vary in formulation? To address this, let’s dissect the composition of these vaccines and the rationale behind their design.
From an analytical perspective, the primary components of mRNA vaccines (Pfizer-BioNTech and Moderna) include mRNA molecules encoding the SARS-CoV-2 spike protein, lipids for encapsulation, and stabilizers like sucrose. For viral vector vaccines (AstraZeneca and Johnson & Johnson), the formulation includes a modified adenovirus carrying genetic material for the spike protein, along with stabilizers and buffers. In all cases, the active ingredient—whether mRNA or viral vector—remains consistent across doses. However, slight variations in excipients (inactive substances) may occur due to manufacturing processes, though these differences are minimal and do not impact efficacy or safety. For example, the Pfizer vaccine’s second dose contains the same 30 micrograms of mRNA as the first, with identical lipid nanoparticles.
Instructively, it’s crucial to understand that the consistency in formulation is intentional. Both doses are designed to prime and then boost the immune response. The first dose introduces the immune system to the spike protein, triggering initial antibody production. The second dose amplifies this response, ensuring a robust and durable immunity. Deviating from this standardized composition could compromise the vaccine’s effectiveness. For instance, altering the mRNA concentration or lipid composition in the second dose might lead to suboptimal immune activation or increased side effects.
Comparatively, while the core ingredients remain the same, the Johnson & Johnson vaccine stands out as a single-dose regimen. Its formulation includes a non-replicating adenovirus 26 vector, which delivers the spike protein gene in one shot. This contrasts with the two-dose mRNA vaccines, where the repeated exposure to the same formulation is key to building immunity. The consistency in composition across doses is a shared principle, even if the number of doses differs.
Practically, individuals receiving these vaccines should be aware that any perceived differences in side effects between doses are not due to changes in formulation but rather to the immune system’s evolving response. For example, the second dose of mRNA vaccines often causes more pronounced side effects (e.g., fatigue, fever) because the immune system is already primed and reacts more vigorously. To manage this, healthcare providers recommend staying hydrated, resting, and using over-the-counter pain relievers as needed.
In conclusion, both doses of multi-dose vaccines contain identical active ingredients and minimal variations in excipients, ensuring consistent immune stimulation. This uniformity is a cornerstone of vaccine design, optimizing efficacy and safety. Understanding this composition clarifies why adhering to the recommended dosing schedule is essential for achieving full protection against COVID-19.
The Most Popular Vaccine in the US: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Dosage Strength: Is the amount of active substance the same in both vaccine shots?
The COVID-19 vaccines authorized for use typically administer the same dosage strength in both shots for individuals aged 12 and older. For instance, the Pfizer-BioNTech vaccine delivers 30 micrograms of mRNA in each dose, while Moderna provides 100 micrograms. This consistency ensures a standardized immune response across the population. However, exceptions exist for specific age groups or medical conditions. Children aged 5–11 receive a lower dose of 10 micrograms per Pfizer shot, tailored to their smaller body mass and immune system maturity. Understanding these variations is crucial for informed decision-making and adherence to vaccination protocols.
From a practical standpoint, ensuring the correct dosage strength is a collaborative effort between healthcare providers and recipients. Vaccination sites follow strict guidelines to administer the appropriate dose based on age and vaccine type. For example, Moderna’s 100-microgram dose is exclusively for individuals aged 18 and older, while Pfizer’s 30-microgram dose is for those 12 and up. Parents and caregivers must verify the correct pediatric dosage for younger children, as errors can compromise efficacy or safety. Always confirm the vaccine type and dosage with the administering healthcare professional before proceeding.
A comparative analysis reveals that while dosage strength remains consistent within a vaccine series for most adults, differences arise when comparing vaccines. AstraZeneca’s viral vector vaccine, for instance, delivers 5 × 10^10 viral particles per dose, a fundamentally different measurement from mRNA vaccines. This highlights the importance of not interchanging vaccines mid-series unless explicitly advised by health authorities. For example, if a first dose of Moderna is administered, the second dose should also be Moderna to maintain consistency in both dosage strength and vaccine type.
Persuasively, adhering to the prescribed dosage strength is non-negotiable for optimal protection. Studies show that receiving the correct dose in both shots maximizes antibody production and long-term immunity. Deviations, such as administering a pediatric dose to an adult or vice versa, can lead to suboptimal responses or adverse effects. For those with concerns about dosage, consulting a healthcare provider is essential. They can clarify whether adjustments are necessary based on individual health conditions, such as immunocompromised states, where additional doses or modified regimens may be recommended.
In conclusion, while the dosage strength of active substances is generally consistent across both vaccine shots for adults, variations exist for specific demographics and vaccine types. Awareness of these differences empowers individuals to actively participate in their vaccination process. Always follow age-specific guidelines, verify vaccine details, and seek professional advice for personalized concerns. This knowledge ensures not only individual protection but also contributes to broader public health goals.
Tracking US Vaccination Progress: How Many Doses Administered So Far?
You may want to see also
Explore related products

![Disposable Shot Glasses [Pack of 36] - 2oz Red Plastic Shot Cups- Jello Shot, Party Shot Glasses For Birthdays, Graduations, Bachelorette, BBQs & More- Mini Tasting/Sample Cups](https://m.media-amazon.com/images/I/6198KiBm5rL._AC_UL320_.jpg)




![]()
Manufacturer Consistency: Are both doses produced by the same manufacturer or different ones?
In most vaccination protocols, both doses are ideally produced by the same manufacturer to ensure consistency in formulation, potency, and immune response. This practice is particularly critical for vaccines like Pfizer-BioNTech and Moderna, where each dose contains 30 µg and 100 µg of mRNA, respectively. Mixing manufacturers could introduce variability in lipid nanoparticle composition or mRNA stability, potentially affecting efficacy. For instance, the UK’s COVID-19 vaccination program initially allowed mixing doses in emergencies, but studies emphasized the importance of homologous dosing for optimal antibody production.
However, exceptions exist, especially in resource-constrained settings or during supply shortages. The World Health Organization (WHO) has conditionally endorsed heterologous dosing (e.g., AstraZeneca followed by Pfizer) based on studies showing comparable or enhanced immune responses in some cases. For example, a Canadian study found that mixing AstraZeneca and mRNA vaccines resulted in higher neutralizing antibody titers than two AstraZeneca doses. Yet, this approach requires careful consideration of age groups—individuals over 50 may respond differently due to age-related immune decline—and potential side effects, such as increased myalgia or fatigue.
From a logistical standpoint, ensuring manufacturer consistency simplifies inventory management and reduces administrative errors. Vaccination sites must track lot numbers and expiration dates, which become more complex when multiple manufacturers are involved. For instance, Pfizer doses require ultra-cold storage (-70°C), while Moderna doses can be stored at -20°C, adding operational challenges if both are used interchangeably. Clear labeling and staff training are essential to avoid mix-ups, particularly in mass vaccination campaigns targeting diverse age categories, such as adolescents (12–17 years) and older adults (65+).
Ultimately, while same-manufacturer dosing remains the gold standard, flexibility in mixing doses has proven beneficial in specific scenarios. Individuals should follow local health guidelines, which often prioritize completing the vaccine series over strict manufacturer consistency. Practical tips include keeping a vaccination card with dose details, scheduling appointments at the same clinic if possible, and discussing concerns with a healthcare provider, especially if pre-existing conditions or age-related factors apply. Manufacturer consistency ensures predictability, but adaptability in public health strategies can address real-world challenges effectively.
Vaccine Recall Alert: Major Drug Company Announces Critical Issue
You may want to see also
Explore related products






![]()
Immune Response: Does each shot trigger the same level of immune system activation?
The immune response to vaccine shots is a nuanced process, and the level of activation can vary between doses. For instance, the first dose of an mRNA COVID-19 vaccine, such as Pfizer-BioNTech or Moderna, often acts as a primer, introducing the immune system to the spike protein of the SARS-CoV-2 virus. This initial exposure triggers the production of antibodies and the activation of T cells, but the response is generally milder. Side effects like soreness at the injection site, fatigue, or mild fever are common but less intense. The second dose, administered 3-4 weeks later, acts as a booster, significantly ramping up the immune response. Studies show that antibody levels can increase 10-fold after the second shot, providing robust protection against severe disease. This staged approach ensures the immune system is fully prepared to combat the virus.
Consider the dosage and formulation of each shot, as these factors influence immune activation. In some vaccines, like the Pfizer-BioNTech COVID-19 vaccine, both doses contain the same amount of mRNA (30 micrograms). However, the immune system’s reaction to the second dose is often stronger due to immunological memory. For other vaccines, such as the Oxford-AstraZeneca COVID-19 vaccine, the dosage remains consistent, but the immune response is still heightened with the second dose. Age also plays a role; younger individuals (18-55 years) tend to mount a more vigorous immune response compared to older adults (65+ years), who may produce fewer antibodies. Understanding these variables helps explain why side effects and immune activation can differ between shots, even with identical dosages.
To maximize immune activation from each shot, follow practical guidelines. Ensure you’re well-rested and hydrated before vaccination, as fatigue or dehydration can dampen the immune response. Avoid over-the-counter pain relievers like ibuprofen or acetaminophen before vaccination unless medically advised, as they may interfere with immune signaling. After the shot, gentle arm movement can help reduce soreness and improve lymphatic circulation, aiding immune cell activation. Monitor side effects, as a stronger reaction to the second dose is normal and indicates a robust immune response. If you experience severe or persistent symptoms, consult a healthcare provider. These steps can help optimize the immune activation triggered by each vaccine dose.
Comparing immune responses across different vaccine platforms reveals further insights. For example, viral vector vaccines like Johnson & Johnson’s single-dose shot elicit a different immune profile than mRNA vaccines. While mRNA vaccines primarily stimulate antibody production, viral vector vaccines also robustly activate T cells, which are crucial for long-term immunity. In contrast, inactivated virus vaccines, such as Sinovac’s CoronaVac, often require multiple doses to achieve comparable immune activation. This highlights that while the goal of all vaccines is to trigger immunity, the mechanisms and levels of activation vary based on the technology used. Understanding these differences can help individuals and healthcare providers make informed decisions about vaccination strategies.
Finally, the concept of immune activation extends beyond immediate antibody production. The second vaccine dose not only boosts antibodies but also enhances the quality of the immune response by promoting the development of memory B cells and long-lived plasma cells. These cells provide durable immunity, ensuring a faster and more effective response if the virus is encountered in the future. For example, studies show that six months after the second dose of an mRNA vaccine, memory B cells continue to evolve, producing antibodies capable of neutralizing even variant strains of the virus. This long-term immune activation underscores the importance of completing the full vaccine series, as each dose contributes uniquely to building comprehensive protection.
When Did Vaccines Become Mandatory in Public Schools?
You may want to see also
Explore related products





![]()
Interval Impact: Does the time gap between doses affect their composition or effectiveness?
The interval between vaccine doses can significantly influence immune response, but it doesn’t alter the physical composition of the shots themselves. Whether it’s an mRNA vaccine like Pfizer-BioNTech or Moderna, or a viral vector vaccine like AstraZeneca, each dose contains the same formulation of active ingredients, stabilizers, and adjuvants. The difference lies in how the immune system responds to the timing. For instance, the Pfizer vaccine initially recommended a 3-week interval, while the UK extended it to 12 weeks to maximize first-dose coverage during supply shortages. This strategic delay didn’t change the vaccine’s makeup but amplified its population-level impact by providing partial immunity to more people faster.
Consider the immune system’s memory function: a longer interval between doses can enhance the quality of antibodies produced. Studies on the Oxford-AstraZeneca vaccine showed that a 12-week gap resulted in higher neutralizing antibody levels compared to a 4-week interval. Similarly, Moderna’s phase 3 trial used a 4-week gap, but real-world data suggests extending it to 6–8 weeks may improve efficacy, particularly in older adults. This isn’t about the vaccine’s composition changing but about optimizing the body’s response. For example, a 65-year-old with a weakened immune system might benefit more from a longer interval, as it allows their body to mount a more robust reaction to the second dose.
However, longer intervals aren’t universally superior. Shorter gaps can provide quicker full protection, which is critical during outbreaks. The CDC’s initial 3-week recommendation for Pfizer and 4-week for Moderna aimed to balance speed and efficacy. In high-risk populations, such as healthcare workers exposed to COVID-19 daily, sticking to these intervals ensures faster immunity. Practical tip: if you’re in a high-transmission area, prioritize the standard interval unless advised otherwise by a healthcare provider. Deviating from the recommended schedule without guidance could leave you vulnerable during the extended gap.
Age and health status also play a role in interval decisions. Adolescents and young adults, whose immune systems are highly responsive, may benefit from shorter intervals to minimize the risk of infection during the dosing period. Conversely, immunocompromised individuals might require a longer interval to ensure their bodies can adequately process and respond to the vaccine. For example, a 30-year-old with no comorbidities might follow the standard schedule, while a 70-year-old with diabetes could discuss extending the gap with their doctor. Always consult a healthcare professional before altering the recommended interval.
In summary, while the vaccine doses themselves remain identical, the interval between them acts as a lever to fine-tune immune response based on individual and population needs. Shorter gaps offer rapid protection, while longer ones can enhance antibody quality. The key is aligning the interval with personal health status, community transmission rates, and vaccine availability. Practical takeaway: if you’re unsure about the best interval for your situation, discuss it with a healthcare provider. They can help weigh factors like age, immunity, and local outbreak dynamics to tailor the timing for optimal effectiveness.
Upholding Parental Trust in Vaccines Amidst Misinformation and Challenges
You may want to see also
Frequently asked questions
Yes, for most COVID-19 vaccines, both doses are the same formulation and contain the same active ingredients. However, some vaccines, like the Moderna vaccine, have a half-dose option for booster shots, but this is not part of the initial two-dose series.
Ideally, you should receive the same vaccine brand for both doses, as this is how the vaccines were studied in clinical trials. However, in some cases, mixing vaccines (heterologous vaccination) is allowed and can still provide robust immunity, depending on local health guidelines.
Side effects can vary between the first and second doses. Many people experience more noticeable side effects (e.g., fatigue, fever, or arm pain) after the second dose, as the immune response is stronger. However, this is not universal, and some individuals may have milder reactions.
In some regions, health authorities allow mixing vaccines if the same brand is not available. For example, someone who received Pfizer for their first dose might get Moderna for the second. Always follow local health guidelines for such scenarios.
Yes, both doses are crucial for achieving full protection. The first dose primes the immune system, while the second dose significantly boosts immunity, providing longer-lasting and more effective protection against the virus. Skipping the second dose reduces the vaccine's effectiveness.