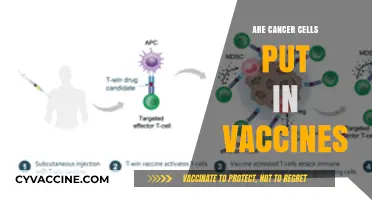
Blood clots have emerged as a rare but concerning side effect associated with certain COVID-19 vaccines, particularly those using adenovirus vector technology. While the incidence of vaccine-induced thrombotic thrombocytopenia (VITT) is extremely low, it has raised questions about the treatability of such clots. Medical professionals emphasize that prompt diagnosis and specialized treatment, including the use of non-heparin anticoagulants and immune globulin, can effectively manage these clots. Early recognition of symptoms, such as persistent headaches, abdominal pain, or unusual bruising, is crucial for successful intervention. Despite the rarity of this side effect, ongoing research and clinical guidelines continue to refine treatment approaches, ensuring that individuals affected by vaccine-related blood clots receive appropriate and timely care.
| Characteristics | Values |
|---|---|
| Treatability | Yes, blood clots associated with vaccines (e.g., rare cases linked to adenovirus vector vaccines like AstraZeneca or J&J) are treatable. |
| Common Treatment | Anticoagulants (blood thinners) such as low-molecular-weight heparin (LMWH) are recommended instead of heparin due to the risk of heparin-induced thrombocytopenia (HIT) in vaccine-induced immune thrombotic thrombocytopenia (VITT). |
| Specific Condition | Vaccine-induced immune thrombotic thrombocytopenia (VITT) or thrombosis with thrombocytopenia syndrome (TTS) is a rare condition treatable with non-heparin anticoagulants and intravenous immunoglobulin (IVIG). |
| Symptoms to Watch | Persistent severe headache, blurred vision, chest pain, leg swelling, easy bruising, or pinpoint rash (petechiae) after vaccination. |
| Timeframe for Symptoms | Symptoms typically appear 4-28 days post-vaccination. |
| Risk Factors | Higher risk in younger adults (under 50-60 years), particularly women, for adenovirus vector vaccines. |
| Vaccines Associated | Adenovirus vector vaccines (AstraZeneca, J&J) have rare links to blood clots; mRNA vaccines (Pfizer, Moderna) have no established causal link to blood clots. |
| Prognosis | Early diagnosis and treatment lead to favorable outcomes in most cases. |
| Prevalence | Extremely rare (e.g., ~1 in 100,000 for AstraZeneca vaccine). |
| Medical Guidance | Seek immediate medical attention if symptoms occur post-vaccination. |
| Alternative Vaccines | mRNA vaccines are recommended for individuals at higher risk of VITT/TTS. |
| Global Recommendations | Health agencies (e.g., WHO, CDC) emphasize that vaccine benefits outweigh the rare risk of blood clots. |
| Research Status | Ongoing research to better understand mechanisms and improve treatment protocols. |
Explore related products






What You'll Learn
![]()
Recognizing Vaccine-Induced Blood Clot Symptoms
Vaccine-induced blood clots, though rare, have been a focal point of concern following the rollout of certain COVID-19 vaccines, particularly adenovirus vector-based ones like AstraZeneca and Johnson & Johnson. Recognizing the symptoms early is crucial for timely intervention. Unlike typical blood clots, vaccine-induced thrombotic thrombocytopenia (VITT) often presents with a unique combination of clotting and bleeding tendencies due to a drop in platelet levels. This paradoxical condition demands vigilance, especially within 4 to 28 days post-vaccination, the window during which most cases emerge.
Symptoms of vaccine-induced blood clots can mimic those of common ailments, making them easy to overlook. Persistent, severe headaches that worsen with movement or over time, often accompanied by blurred vision or seizures, are red flags. Unusual bruising or pinpoint red spots (petechiae) on the skin, along with swelling, pain, or discoloration in the arms or legs, signal potential clotting issues. Gastrointestinal symptoms like abdominal pain, nausea, or blood in the stool should also raise concern, as VITT can cause clots in the abdominal veins. If these symptoms appear after vaccination, particularly in individuals under 60, immediate medical attention is essential.
Diagnosis relies on recognizing this distinct symptom cluster and confirming low platelet counts alongside clotting markers. Treatment differs from standard clot management; heparin, a common anticoagulant, is contraindicated due to the risk of exacerbating thrombocytopenia. Instead, non-heparin anticoagulants like fondaparinux, coupled with intravenous immunoglobulin (IVIG) to neutralize the immune response, are recommended. Early intervention significantly improves outcomes, with studies showing a 70-80% survival rate when treated promptly.
Prevention hinges on awareness and risk stratification. Health agencies have adjusted guidelines, recommending mRNA vaccines (Pfizer, Moderna) over adenovirus vector vaccines for younger populations. For those who’ve received a first dose of an adenovirus vaccine without complications, completing the series with an mRNA vaccine is advised. Public health campaigns emphasizing symptom recognition and the importance of seeking care within the critical post-vaccination window have been pivotal in reducing severe outcomes.
In summary, recognizing vaccine-induced blood clot symptoms requires attentiveness to specific neurological, dermatological, and gastrointestinal signs within a defined timeframe. Swift, targeted treatment can mitigate risks, underscoring the need for public education and healthcare provider training. While rare, the impact of VITT highlights the delicate balance between vaccination benefits and vigilance against adverse events.
Polio Vaccine Rollout in the Philippines: A Historical Overview
You may want to see also
Explore related products





![]()
Available Treatment Options for Vaccine-Related Clots
Blood clots associated with certain vaccines, such as the rare but serious condition known as vaccine-induced immune thrombotic thrombocytopenia (VITT), require prompt and specialized treatment. Unlike typical blood clots, VITT involves a unique mechanism where the body produces antibodies against platelet factor 4 (PF4), leading to abnormal clotting and low platelet counts. Treatment must address both the clotting and the underlying immune response, making it distinct from standard clot management.
Step 1: Immediate Anticoagulation with Non-Heparin Agents
The first line of treatment for vaccine-related clots is anticoagulation, but not with heparin. Heparin can worsen VITT due to its interaction with PF4 antibodies. Instead, direct oral anticoagulants (DOACs) like rivaroxaban or apixaban, or parenteral agents like argatroban or bivalirudin, are used. For example, rivaroxaban is typically prescribed at 15 mg twice daily for the first three weeks, followed by 20 mg daily for long-term management. This approach prevents further clot formation while minimizing bleeding risks.
Step 2: Intravenous Immunoglobulin (IVIG) Therapy
To neutralize the PF4 antibodies driving the immune response, high-dose intravenous immunoglobulin (IVIG) is administered. A typical dose is 1 g/kg body weight per day for two days. IVIG works by blocking the antibodies and stabilizing platelet counts. This treatment is often initiated alongside anticoagulation for rapid control of the immune-mediated process.
Step 3: Corticosteroids for Immune Suppression
Corticosteroids, such as methylprednisolone or prednisone, are used to suppress the immune response and reduce inflammation. Methylprednisolone is commonly given at 1–2 mg/kg/day intravenously, followed by an oral taper of prednisone over several weeks. This step is crucial for preventing recurrent clotting episodes and managing long-term immune complications.
Cautions and Monitoring
Treating vaccine-related clots requires careful monitoring to avoid complications. Regular platelet count checks and coagulation studies are essential to assess treatment efficacy. Patients should be warned about signs of bleeding (e.g., easy bruising, nosebleeds) or recurrent clotting (e.g., swelling, pain in limbs). Additionally, alternative vaccines should be considered for future immunizations to avoid triggering a similar reaction.
Vaccine-related clots demand a tailored treatment strategy that combines anticoagulation, immune modulation, and close monitoring. While the condition is rare, early recognition and intervention are critical for successful outcomes. Patients and healthcare providers must remain vigilant and informed to navigate this complex but treatable condition effectively.
Battling Malaria: The Pre-Vaccination Struggles of Soldiers on Duty
You may want to see also
Explore related products





![]()
Role of Anticoagulants in Clot Management
Blood clots associated with vaccines, though rare, have raised significant concern, particularly with certain COVID-19 vaccines. When such clots occur, prompt and effective treatment is critical to prevent severe complications like stroke or organ damage. Anticoagulants, commonly known as blood thinners, play a central role in managing these clots by inhibiting the coagulation process and preventing further clot growth. Unlike antiplatelet drugs, which target platelet aggregation, anticoagulants act on the clotting cascade, making them essential for treating vaccine-induced thrombotic events, such as cerebral venous sinus thrombosis (CVST).
The choice of anticoagulant and dosage depends on the clot’s location, severity, and patient-specific factors. For instance, low molecular weight heparin (LMWH), such as enoxaparin, is often preferred over unfractionated heparin due to its predictable dosing and lower risk of complications. A typical starting dose of enoxaparin is 1 mg/kg every 12 hours, adjusted based on anti-Xa levels and renal function. Direct oral anticoagulants (DOACs) like rivaroxaban or apixaban may be used in stable patients, offering convenience with once- or twice-daily dosing. However, in cases of CVST or heparin-induced thrombocytopenia (HIT), alternatives like fondaparinux or argatroban are necessary to avoid exacerbating the condition.
One critical consideration is the duration of anticoagulant therapy, which varies based on the clot’s resolution and bleeding risk. For vaccine-induced immune thrombotic thrombocytopenia (VITT), treatment often includes high-dose intravenous immunoglobulin (IVIG) alongside anticoagulation, with therapy continuing for 3–6 months or longer in some cases. Monitoring is essential, particularly for patients on warfarin, where regular INR checks ensure the drug’s effectiveness without increasing bleeding risk. For DOACs, routine monitoring is less frequent but may be warranted in patients with renal impairment or those at high bleeding risk.
While anticoagulants are effective, they are not without risks. Major bleeding, particularly in the gastrointestinal tract or brain, is a significant concern, especially in older adults or those with comorbidities. Patients should be educated on signs of bleeding, such as unusual bruising, blood in urine or stool, or severe headaches. Practical tips include avoiding contact sports, using soft-bristled toothbrushes, and ensuring medication adherence. In cases of minor bleeding, such as nosebleeds, applying direct pressure and seeking medical advice is crucial. For major bleeding, immediate reversal agents like idarucizumab (for dabigatran) or andexanet alfa (for factor Xa inhibitors) may be lifesaving.
In summary, anticoagulants are a cornerstone in treating blood clots from vaccines, offering targeted therapy to prevent clot progression and complications. Tailored dosing, careful monitoring, and patient education are vital to balancing efficacy and safety. As research evolves, guidelines for managing vaccine-related clots will likely refine, emphasizing the importance of individualized treatment plans. For healthcare providers and patients alike, understanding the role of anticoagulants ensures timely and effective intervention in these rare but serious events.
Vaccine and Alcohol: What's Safe?
You may want to see also
Explore related products






![]()
Timeframe for Treatment Effectiveness
The effectiveness of treating blood clots related to vaccines hinges critically on the timing of intervention. Immediate recognition and response are paramount, as delays can exacerbate complications such as deep vein thrombosis (DVT) or pulmonary embolism (PE). For instance, symptoms like persistent leg pain, swelling, or shortness of breath warrant urgent medical attention. Anticoagulant therapy, often initiated within 24 hours of diagnosis, is the cornerstone of treatment, with low molecular weight heparin (LMWH) typically administered at a dosage of 1 mg/kg every 12 hours for adults. This rapid action can prevent clot propagation and reduce the risk of long-term sequelae.
Contrastingly, the treatment window for rare vaccine-induced immune thrombotic thrombocytopenia (VITT) is more complex. VITT, associated with adenovirus vector vaccines, requires specialized management, including high-dose intravenous immunoglobulin (IVIG, 1 g/kg daily for 2 days) and non-heparin anticoagulants like argatroban. Unlike conventional clots, VITT treatment must begin within hours of suspicion, as platelet counts can plummet rapidly. Delays in administering IVIG or failing to avoid platelet transfusions can lead to catastrophic outcomes, emphasizing the need for swift, protocol-driven care.
Age and comorbidities further influence treatment timelines. Younger, otherwise healthy individuals may respond more rapidly to anticoagulation, whereas older adults or those with renal impairment may require dosage adjustments and extended monitoring. For example, direct oral anticoagulants (DOACs) like rivaroxaban (15 mg twice daily for 21 days, then 20 mg daily) are often preferred for their convenience but must be used cautiously in patients with creatinine clearance below 30 mL/min. Tailoring treatment to individual risk profiles ensures both efficacy and safety within the critical timeframe.
Practical tips for patients and providers include maintaining a high index of suspicion post-vaccination, especially within 4–28 days for VITT. Patients should be educated to monitor for symptoms and seek care promptly, while healthcare teams must prioritize rapid diagnostic workups, including D-dimer testing and platelet count assessments. Early collaboration with hematologists can streamline decision-making, ensuring that treatment is initiated within the narrow window where interventions are most effective. In the race against clot-related complications, every hour counts.
Vaccines and Allergies: Unraveling the Potential Connection and Facts
You may want to see also
Explore related products





![]()
Preventive Measures Post-Vaccination Clot Diagnosis
Blood clots post-vaccination, though rare, demand immediate attention and proactive management. Once diagnosed, the focus shifts from treatment to prevention of recurrence or complications. This involves a multifaceted approach tailored to individual risk factors and clot characteristics.
Understanding the Landscape:
While research continues, evidence suggests certain vaccines, particularly adenovirus vector-based ones like AstraZeneca and Johnson & Johnson, have a slightly elevated risk of rare blood clots, often accompanied by low platelet counts (thrombosis with thrombocytopenia syndrome, TTS). These clots often occur in unusual locations, such as the brain (cerebral venous sinus thrombosis) or abdomen.
Early diagnosis is crucial, as prompt treatment with specialized anticoagulants and, in some cases, immunoglobulin therapy, significantly improves outcomes.
Proactive Prevention:
Following a clot diagnosis post-vaccination, the primary goal is preventing future clots and mitigating potential complications. This involves a combination of medical interventions and lifestyle adjustments:
- Anticoagulant Therapy: Long-term anticoagulant medication, such as warfarin or direct oral anticoagulants (DOACs), is often prescribed to prevent new clot formation. Dosage and duration are individualized based on clot severity, location, and individual risk factors.
- Platelet Monitoring: Regular blood tests to monitor platelet counts are essential, especially in cases of TTS. This allows for early detection of any recurrence of thrombocytopenia and adjustment of treatment accordingly.
- Lifestyle Modifications:
- Hydration: Staying adequately hydrated helps prevent blood from becoming too thick and clotting more easily. Aim for 8-10 glasses of water daily.
- Movement: Regular physical activity, even gentle exercises like walking, improves blood flow and reduces clotting risk. Avoid prolonged periods of immobility, especially during travel.
- Smoking Cessation: Smoking damages blood vessels and increases clotting risk. Quitting smoking is crucial for long-term clot prevention.
- Healthy Diet: A diet rich in fruits, vegetables, whole grains, and healthy fats promotes overall cardiovascular health and reduces clotting risk.
Individualized Approach:
The specific preventive measures recommended will vary depending on the individual's medical history, clot characteristics, and overall health. Close collaboration with a hematologist is essential to develop a personalized plan. This may involve:
- Specialized Imaging: Follow-up imaging studies, such as MRI or CT scans, may be necessary to monitor clot resolution and detect any new clots.
- Genetic Testing: In some cases, genetic testing may be recommended to identify underlying clotting disorders that could contribute to recurrent clots.
- Psychological Support: A clot diagnosis can be emotionally challenging. Access to counseling or support groups can help individuals cope with anxiety and fear.
Long-Term Vigilance:
While preventive measures significantly reduce the risk of recurrent clots, long-term vigilance is crucial. Individuals with a history of vaccine-related clots should be aware of the signs and symptoms of clotting, such as swelling, pain, redness, and shortness of breath, and seek immediate medical attention if they experience any of these. Regular follow-up appointments with a hematologist are essential for ongoing monitoring and adjustment of the preventive plan as needed.
Reimmunization for Hep B Vaccine: Is It Necessary or Redundant?
You may want to see also
Frequently asked questions
Yes, blood clots caused by vaccines, such as those associated with rare cases of the Johnson & Johnson or AstraZeneca vaccines, are treatable. Treatment typically involves anticoagulant medications (blood thinners) and close medical monitoring.
Treatment options include anticoagulants like heparin or direct oral anticoagulants (DOACs), but not heparin in cases of thrombosis with thrombocytopenia syndrome (TTS). Corticosteroids and intravenous immunoglobulin (IVIG) may also be used to manage associated immune responses.
Vaccine-related blood clots, especially those linked to rare conditions like TTS, require immediate medical attention. Early diagnosis and treatment are critical to prevent severe complications such as stroke or organ damage. Seek medical help promptly if symptoms like persistent headaches, abdominal pain, or swelling occur after vaccination.