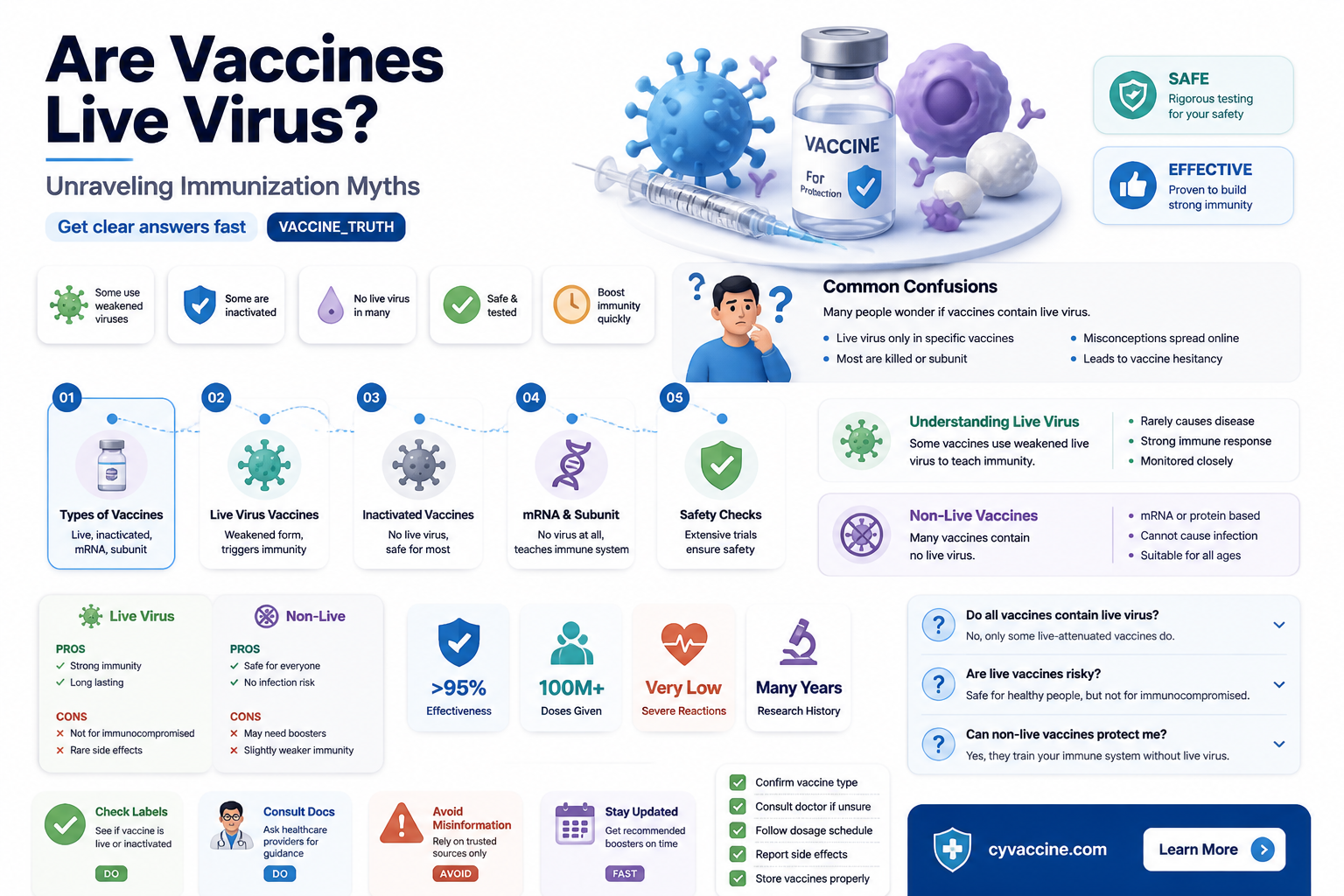
Vaccinations are a cornerstone of public health, but a common question arises regarding whether any vaccines contain live viruses. The answer is yes—some vaccines, known as live attenuated vaccines, do contain weakened (attenuated) forms of the virus they aim to protect against. These viruses are modified to be harmless while still triggering a robust immune response. Examples include the measles, mumps, and rubella (MMR) vaccine, the varicella (chickenpox) vaccine, and the nasal spray flu vaccine. Although live attenuated vaccines are highly effective, they are generally not recommended for individuals with weakened immune systems, as there is a minimal risk the virus could cause illness in these cases. Understanding the nature of these vaccines helps clarify their safety and importance in preventing infectious diseases.
| Characteristics | Values |
|---|---|
| Definition | Live virus vaccines use a weakened (attenuated) form of the virus, which can still replicate but does not cause severe disease in healthy individuals. |
| Examples | Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Rotavirus, Yellow Fever, Oral Polio Vaccine (OPV), Zoster (Shingles) |
| Mechanism | Stimulates a strong immune response by mimicking a natural infection, leading to the production of antibodies and memory cells. |
| Efficacy | Generally highly effective, often providing long-lasting immunity after one or two doses. |
| Safety | Generally safe for healthy individuals, but may cause mild side effects (e.g., fever, rash). Not recommended for immunocompromised individuals or pregnant women. |
| Storage | Often requires refrigeration (2–8°C) to maintain viability of the live virus. |
| Shedding | Some live virus vaccines (e.g., OPV) can lead to viral shedding, potentially transmitting the vaccine virus to close contacts. |
| Contraindications | Immunocompromised individuals, pregnant women, and those with severe allergies to vaccine components. |
| Duration of Immunity | Typically long-lasting, often lifelong, but may require boosters in some cases (e.g., shingles vaccine). |
| Development Time | Longer development process due to the need to safely attenuate the virus. |
| Cost | Generally more expensive to produce and store compared to inactivated or subunit vaccines. |
| Global Use | Widely used globally, especially in childhood immunization programs, but alternatives (e.g., inactivated vaccines) are preferred in certain populations. |
Explore related products

$16.53 $17.99





What You'll Learn
- Live vs. Inactivated Vaccines: Key differences in how they work and immune response
- Examples of Live Vaccines: MMR, varicella, and yellow fever vaccines explained
- Safety Concerns: Risks for immunocompromised individuals and rare side effects
- Attenuated Viruses: How live vaccines are weakened for safety and efficacy
- Benefits of Live Vaccines: Long-lasting immunity and fewer doses required
![]()
Live vs. Inactivated Vaccines: Key differences in how they work and immune response
Vaccines are categorized primarily into live and inactivated types, each harnessing distinct mechanisms to trigger immune responses. Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened (attenuated) viruses that replicate in the body without causing disease. This replication mimics a natural infection, prompting a robust and long-lasting immune response, often requiring only one or two doses. Inactivated vaccines, like the injectable polio vaccine (IPV), use viruses rendered non-replicative through chemical or physical methods. These vaccines typically necessitate multiple doses and booster shots to achieve comparable immunity, as they elicit a less intense immune reaction.
Consider the varicella vaccine, a live vaccine administered to children aged 12–15 months, with a booster at 4–6 years. Its attenuated virus stimulates both humoral (antibody-mediated) and cell-mediated immunity, providing over 90% protection against chickenpox. In contrast, the inactivated influenza vaccine, given annually to individuals aged 6 months and older, targets specific viral proteins, primarily inducing antibodies. This narrower response explains why seasonal flu shots are reformulated yearly to match circulating strains, whereas live vaccines like MMR offer lifelong immunity after two doses.
From a practical standpoint, live vaccines are contraindicated in immunocompromised individuals due to the theoretical risk of viral reversion to a pathogenic form. For instance, the live yellow fever vaccine is avoided in those with HIV or undergoing chemotherapy. Inactivated vaccines, however, pose no such risk, making them safer for vulnerable populations. Pregnant individuals, for example, receive the inactivated Tdap vaccine to protect against tetanus, diphtheria, and pertussis, while live vaccines like varicella are deferred until postpartum.
The immune response kinetics also differ. Live vaccines produce memory cells and antibodies more rapidly, often within 2–3 weeks of the first dose. Inactivated vaccines may take 4–6 weeks post-primary series to confer protection, with boosters extending immunity. For instance, the hepatitis A vaccine (inactivated) requires two doses spaced 6–12 months apart to achieve long-term immunity, whereas the live oral typhoid vaccine (Ty21a) offers protection after 3–4 doses over 5–7 days.
In summary, live vaccines leverage attenuated viruses to generate a comprehensive, durable immune response, ideal for healthy individuals. Inactivated vaccines, while safer for at-risk groups, demand repeated dosing to sustain immunity. Understanding these differences empowers healthcare providers and recipients to make informed decisions, balancing efficacy with safety in vaccination strategies.
Uploading Vaccination Certificates in Singapore: A Guide for Foreigners
You may want to see also
Explore related products






![]()
Examples of Live Vaccines: MMR, varicella, and yellow fever vaccines explained
Live vaccines contain a weakened (attenuated) form of the virus they aim to protect against, triggering a robust immune response without causing severe illness. Among the most well-known live vaccines are the MMR (measles, mumps, rubella), varicella (chickenpox), and yellow fever vaccines. Each serves a distinct purpose, targeting specific viruses with unique administration protocols and age-specific guidelines. Understanding these vaccines—their mechanisms, dosages, and practical considerations—is essential for informed decision-making.
The MMR vaccine is a cornerstone of childhood immunization, typically administered in two doses: the first at 12–15 months and the second at 4–6 years. This live attenuated vaccine contains weakened strains of measles, mumps, and rubella viruses, providing over 95% immunity after the second dose. While generally safe, mild side effects like fever or rash may occur 7–12 days post-vaccination. Notably, the MMR vaccine is contraindicated for pregnant individuals and those with severe immunocompromisation, underscoring the importance of consulting healthcare providers for personalized advice.
In contrast, the varicella vaccine targets the varicella-zoster virus, which causes chickenpox. Recommended for children aged 12–15 months, with a second dose at 4–6 years, this live vaccine reduces the risk of severe chickenpox complications. Adolescents and adults without immunity may require catch-up doses, spaced 4–8 weeks apart. Unlike the MMR vaccine, varicella immunization can cause mild itching or a localized rash at the injection site. Parents should avoid administering aspirin to children post-vaccination due to the risk of Reye’s syndrome, opting for acetaminophen instead to manage fever.
The yellow fever vaccine stands apart as a travel-specific immunization, required for entry into certain countries with endemic transmission. Administered as a single dose to individuals aged 9 months and older, it provides lifelong immunity in most cases. Unlike the MMR and varicella vaccines, yellow fever immunization is not part of routine childhood schedules but is critical for travelers to regions like sub-Saharan Africa and tropical South America. Rare side effects include severe allergic reactions or vaccine-associated viscerotropic disease, emphasizing the need for pre-travel health consultations.
In practice, these live vaccines exemplify the balance between efficacy and safety in immunization. While they share the commonality of using attenuated viruses, their administration, age recommendations, and contraindications differ significantly. For instance, the MMR and varicella vaccines are routine in pediatric care, whereas the yellow fever vaccine is travel-specific. Adhering to dosage schedules, understanding contraindications, and managing side effects are key to maximizing protection. By demystifying these vaccines, individuals can make informed choices, ensuring both personal and community health.
Pierce College Vaccine Site: Drive-Thru Convenience for COVID-19 Shots
You may want to see also
Explore related products






![]()
Safety Concerns: Risks for immunocompromised individuals and rare side effects
Live virus vaccines, while highly effective, pose unique safety concerns, particularly for immunocompromised individuals. These vaccines contain weakened forms of the virus, which can replicate in the body to stimulate a robust immune response. However, in people with weakened immune systems—such as those undergoing chemotherapy, living with HIV, or taking immunosuppressive medications—the virus may not be adequately controlled, leading to potential infection or severe complications. For instance, the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine are live virus vaccines that carry specific warnings for immunocompromised patients. Healthcare providers must carefully assess the risks and benefits before administering these vaccines to vulnerable populations, often opting for alternative strategies like passive immunization or delaying vaccination until immune function improves.
Rare side effects of live virus vaccines further complicate their safety profile, though they occur in a small fraction of recipients. For example, the oral polio vaccine (OPV), though no longer used in the U.S., has been associated with vaccine-derived poliovirus causing paralysis in approximately 1 in 2.7 million doses. Similarly, the yellow fever vaccine, another live virus vaccine, has been linked to severe adverse events such as viscerotropic disease (affecting internal organs) and neurologic complications, occurring in roughly 1 in 200,000 to 1 in 300,000 doses. These risks, while uncommon, underscore the importance of informed consent and careful patient selection, especially in older adults or those with underlying health conditions who may be more susceptible to adverse reactions.
For immunocompromised individuals, the decision to administer live virus vaccines requires a nuanced approach. The CDC and WHO provide guidelines to minimize risks, such as avoiding live vaccines during severe immunosuppression or within specific timeframes before and after treatments like chemotherapy. For example, live vaccines should generally be withheld for at least 3 months after high-dose corticosteroid therapy or until immune reconstitution occurs in patients with HIV. In some cases, serologic testing may be recommended to confirm immunity before proceeding with vaccination. Practical tips include ensuring close monitoring for symptoms of vaccine-related illness and maintaining open communication between specialists and primary care providers to coordinate care effectively.
Comparatively, inactivated or subunit vaccines offer a safer alternative for immunocompromised individuals, as they cannot cause disease even in those with weakened immune systems. However, their efficacy may be reduced in this population due to impaired immune responses. This highlights the delicate balance between protection and risk in vaccine selection. For instance, the inactivated influenza vaccine is preferred over the live attenuated nasal spray for immunocompromised patients, despite the latter’s potential for stronger immunity in healthy individuals. Ultimately, individualized risk assessment, adherence to guidelines, and ongoing research into safer vaccine formulations are critical to addressing safety concerns in this vulnerable group.
VICP Coverage: Exploring Vaccine Types Protected Under the Program
You may want to see also
Explore related products






![]()
Attenuated Viruses: How live vaccines are weakened for safety and efficacy
Live vaccines, such as those for measles, mumps, rubella (MMR), chickenpox, and yellow fever, contain attenuated viruses—microorganisms weakened in the lab to trigger immunity without causing severe disease. Attenuation is achieved through methods like serial passage, where the virus is repeatedly grown in cells or animals until it adapts to replicate less efficiently in humans. For instance, the measles vaccine virus, Edmonston strain, underwent over 80 passages in cell cultures, reducing its virulence while retaining immunogenicity. This process ensures the virus can still infect cells and provoke an immune response but lacks the ability to spread widely or cause illness.
The safety of attenuated viruses hinges on their inability to revert to a virulent form, a concern rigorously addressed during vaccine development. For example, the oral polio vaccine (OPV) uses attenuated poliovirus strains that have been stabilized through genetic modifications to prevent reversion. Despite rare cases of vaccine-derived poliovirus (VDPV) in underimmunized populations, the risk is minimized by following recommended dosing schedules—typically a series of 3–4 doses starting at 2 months of age. This balance between efficacy and safety is further reinforced by contraindicating live vaccines for immunocompromised individuals, as their weakened immune systems may struggle to control even attenuated viruses.
Efficacy is another hallmark of live vaccines, often providing lifelong immunity after one or two doses. The varicella (chickenpox) vaccine, for instance, is 98% effective in preventing severe disease and 70–90% effective against mild disease after two doses administered at 12–15 months and 4–6 years of age. This high efficacy stems from the vaccine’s ability to mimic natural infection, stimulating both humoral (antibody-mediated) and cell-mediated immune responses. Unlike inactivated vaccines, which may require adjuvants or boosters, live vaccines often achieve robust immunity with fewer doses, making them cost-effective and logistically simpler to administer.
Practical considerations for live vaccines include storage, administration, and timing. Most live vaccines require refrigeration at 2–8°C to maintain viability, with exposure to heat or light potentially reducing potency. Healthcare providers must also ensure a 4-week interval between live vaccines if not administered simultaneously, as concurrent administration does not interfere with immune responses. For travelers, vaccines like yellow fever require a single dose at least 10 days before potential exposure, providing lifelong protection. Understanding these specifics ensures optimal use of attenuated virus vaccines, maximizing their safety and efficacy in preventing disease.
Is RSV Vaccine Covered by Medicare Part B? What You Need to Know
You may want to see also
Explore related products






![]()
Benefits of Live Vaccines: Long-lasting immunity and fewer doses required
Live vaccines, such as those for measles, mumps, rubella (MMR), chickenpox, and yellow fever, contain a weakened (attenuated) form of the virus. This design mimics a natural infection without causing severe disease, prompting the immune system to mount a robust response. Unlike inactivated or subunit vaccines, live vaccines closely resemble the actual pathogen, often leading to long-lasting immunity after just one or two doses. For instance, the MMR vaccine is typically administered in two doses—the first at 12–15 months and the second at 4–6 years—providing lifelong protection for 97% of recipients. This efficiency contrasts with vaccines like the annual flu shot, which requires repeated administration due to the virus’s evolving nature.
The mechanism behind live vaccines’ durability lies in their ability to stimulate both humoral (antibody-mediated) and cell-mediated immunity. The attenuated virus replicates locally, triggering memory B and T cells that persist for decades. This dual-pronged response is why diseases like smallpox, eradicated through a live vaccine, no longer require vaccination in most parts of the world. For example, the yellow fever vaccine, a single-dose live vaccine, confers lifelong immunity in 99% of recipients, making it a cornerstone of travel medicine for those visiting endemic regions. This contrasts with the hepatitis B vaccine, which often requires a three-dose series and periodic boosters for sustained protection.
One practical advantage of live vaccines is their reduced dosing schedule, simplifying immunization programs and improving compliance. The varicella (chickenpox) vaccine, for instance, is given in two doses—the first at 12–15 months and the second at 4–6 years—and prevents severe disease in over 90% of vaccinated individuals. This streamlined approach is particularly beneficial in low-resource settings, where multiple clinic visits can be logistically challenging. However, it’s crucial to note that live vaccines are generally not recommended for immunocompromised individuals, pregnant people, or those with specific allergies, as the weakened virus could pose a risk. Always consult a healthcare provider to assess eligibility.
Despite their strengths, live vaccines are not without limitations. Their storage requirements are more stringent, often needing refrigeration to maintain viability. Additionally, the interval between live vaccines must be carefully managed—the CDC recommends spacing them at least 28 days apart to ensure optimal immune response. For example, if a child receives the MMR vaccine, they should wait at least four weeks before getting the varicella vaccine. This spacing rule underscores the need for careful planning in immunization schedules, especially in pediatric populations.
In summary, live vaccines offer a unique combination of long-lasting immunity and dosing efficiency, making them indispensable tools in public health. Their ability to mimic natural infection results in robust, enduring protection, often after just one or two doses. While considerations like storage and contraindications require attention, the benefits far outweigh the challenges. For healthy individuals, live vaccines represent a cornerstone of preventive medicine, safeguarding against diseases that once caused widespread morbidity and mortality. Understanding their mechanisms and practicalities empowers both healthcare providers and recipients to maximize their impact.
Should You Get the Hep A Vaccine? Key Considerations Explained
You may want to see also
Frequently asked questions
Yes, some vaccines contain live, attenuated (weakened) viruses, such as the measles, mumps, rubella (MMR), chickenpox, and shingles vaccines. These vaccines use a weakened form of the virus to trigger an immune response without causing severe illness.
Live virus vaccines are generally safe for most healthy individuals, but they may not be recommended for people with weakened immune systems, pregnant women, or those with certain medical conditions. Always consult a healthcare provider to determine if a live virus vaccine is appropriate for your situation.
While extremely rare, live virus vaccines can cause mild symptoms similar to the disease they prevent. For example, the MMR vaccine may cause a mild rash or fever. However, the risk of severe disease from the vaccine is significantly lower than the risk from the actual infection.