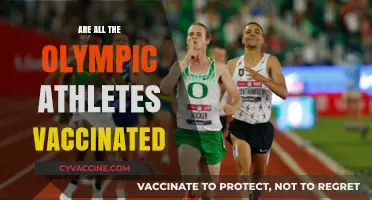
The question of whether all coronavirus vaccines are mRNA-based is a common one, reflecting the significant attention mRNA technology has received during the COVID-19 pandemic. While mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna, have been widely used and highly effective, they are not the only type of COVID-19 vaccine available. Other vaccine platforms include viral vector vaccines, like those from AstraZeneca and Johnson & Johnson, and inactivated virus vaccines, such as Sinovac and Sinopharm. Each type works differently to trigger an immune response, but mRNA vaccines have gained prominence due to their rapid development and high efficacy rates. Understanding the diversity of vaccine technologies is crucial for addressing concerns and ensuring informed decisions about vaccination.
| Characteristics | Values |
|---|---|
| Are all COVID-19 vaccines mRNA? | No, not all COVID-19 vaccines are mRNA-based. |
| Types of COVID-19 vaccines | 1. mRNA vaccines (e.g., Pfizer-BioNTech, Moderna) 2. Viral vector vaccines (e.g., AstraZeneca, Johnson & Johnson) 3. Protein subunit vaccines (e.g., Novavax) 4. Inactivated virus vaccines (e.g., Sinovac, Sinopharm) |
| mRNA vaccines | Use messenger RNA to instruct cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. |
| Viral vector vaccines | Use a modified, harmless virus to deliver genetic material encoding the spike protein into cells. |
| Protein subunit vaccines | Contain harmless pieces of the SARS-CoV-2 spike protein directly, without genetic material. |
| Inactivated virus vaccines | Use a killed version of the SARS-CoV-2 virus to elicit an immune response. |
| Examples of mRNA vaccines | Pfizer-BioNTech (Comirnaty), Moderna (Spikevax) |
| Examples of non-mRNA vaccines | AstraZeneca (Vaxzevria), Johnson & Johnson (Janssen), Novavax (Nuvaxovid), Sinovac (CoronaVac), Sinopharm (BBIBP-CorV) |
| Global usage | mRNA vaccines are widely used in North America, Europe, and parts of Asia, while viral vector and inactivated vaccines are more common in other regions. |
| Efficacy | Varies by vaccine type and strain; mRNA vaccines have shown high efficacy against severe disease and hospitalization. |
| Storage requirements | mRNA vaccines require ultra-cold storage initially, while other types (e.g., viral vector, protein subunit) have less stringent storage needs. |
Explore related products






What You'll Learn
- Non-mRNA Vaccine Types: Includes viral vector, protein subunit, and inactivated virus technologies
- mRNA Vaccine Examples: Pfizer-BioNTech and Moderna use mRNA technology
- Non-mRNA Vaccine Examples: AstraZeneca, Johnson & Johnson, Novavax, Sinovac
- mRNA Vaccine Mechanism: Teaches cells to produce spike protein, triggering immune response
- Global Vaccine Distribution: Mix of mRNA and non-mRNA vaccines used worldwide
![]()
Non-mRNA Vaccine Types: Includes viral vector, protein subunit, and inactivated virus technologies
Not all COVID-19 vaccines rely on mRNA technology. While Pfizer-BioNTech and Moderna’s vaccines use mRNA to instruct cells to produce the SARS-CoV-2 spike protein, other vaccines employ distinct mechanisms to trigger immunity. These alternatives—viral vector, protein subunit, and inactivated virus vaccines—offer diverse options for global vaccination efforts, each with unique advantages and considerations.
Viral vector vaccines, such as Johnson & Johnson’s Janssen and AstraZeneca’s Vaxzevria, use a modified, harmless virus (e.g., adenovirus) to deliver genetic material encoding the spike protein into cells. This approach leverages the body’s natural immune response to viruses, requiring only a single dose for Janssen (0.5 mL) and two doses for AstraZeneca (0.5 mL each, 4–12 weeks apart). These vaccines are particularly useful in resource-limited settings due to their stability at standard refrigerator temperatures (2–8°C). However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have been reported, primarily in younger adults, prompting some countries to restrict their use to older age groups.
Protein subunit vaccines, exemplified by Novavax’s Nuvaxovid, contain purified pieces of the spike protein, often combined with adjuvants to enhance immune response. Administered in two doses (0.5 mL each, 3–8 weeks apart), this vaccine is suitable for individuals aged 12 and older. Its key advantage lies in its familiarity—the technology has been used in vaccines like Hepatitis B and HPV—making it a reassuring option for those hesitant about newer platforms. Storage at 2–8°C further simplifies distribution, though its rollout has been slower compared to mRNA vaccines.
Inactivated virus vaccines, such as Sinovac’s CoronaVac and Sinopharm’s BBIBP-CorV, use viruses rendered incapable of replicating but still capable of eliciting an immune response. Typically given in two doses (0.5 mL each, 2–4 weeks apart), with a third dose recommended for enhanced protection, these vaccines are widely used in countries like China, Brazil, and Indonesia. Their stability at 2–8°C and established manufacturing processes make them accessible globally. However, efficacy rates are generally lower than mRNA vaccines, often requiring additional doses to maintain immunity, particularly in older adults.
Choosing a non-mRNA vaccine depends on availability, individual health conditions, and regional guidelines. For instance, viral vector vaccines may be preferred in areas with limited refrigeration capabilities, while protein subunit vaccines could appeal to those seeking a traditional approach. Inactivated virus vaccines remain a cornerstone in regions with established production infrastructure. Each type underscores the importance of a multifaceted vaccine portfolio to combat the pandemic effectively.
Traveling Unvaccinated: Countries Welcoming Visitors Without Vaccine Requirements
You may want to see also
Explore related products






![]()
mRNA Vaccine Examples: Pfizer-BioNTech and Moderna use mRNA technology
Not all coronavirus vaccines rely on mRNA technology, but the Pfizer-BioNTech and Moderna vaccines are the most prominent examples that do. These vaccines represent a groundbreaking approach to immunization, leveraging messenger RNA (mRNA) to instruct cells to produce a harmless protein mimicking the virus’s spike protein. This triggers an immune response, preparing the body to fight COVID-19 without exposing it to the actual virus. Both vaccines have been authorized for emergency use in numerous countries and have played a pivotal role in global vaccination efforts.
Pfizer-BioNTech’s vaccine, known as Comirnaty, is administered in a two-dose series, typically 3 to 4 weeks apart, with a third dose recommended for certain immunocompromised individuals. The dosage for individuals aged 12 and older is 30 micrograms per shot, while children aged 5 to 11 receive a lower dose of 10 micrograms. Moderna’s vaccine, known as Spikevax, follows a similar two-dose regimen but with a longer interval of 4 to 6 weeks between doses. Each dose contains 100 micrograms of mRNA, making it a higher concentration compared to Pfizer-BioNTech. Both vaccines require storage at ultra-cold temperatures initially, though Pfizer’s can now be stored in standard freezers for short periods, easing distribution challenges.
One key advantage of mRNA vaccines is their rapid development timeline. Unlike traditional vaccines, which can take years to produce, mRNA vaccines can be designed and manufactured within months. This speed was critical in responding to the COVID-19 pandemic. However, this innovation also brought challenges, such as ensuring equitable global distribution and addressing public hesitancy due to the technology’s novelty. Both Pfizer-BioNTech and Moderna have since adapted their vaccines to target emerging variants, demonstrating the flexibility of mRNA platforms.
Practical tips for recipients include scheduling doses well in advance to ensure timely administration and monitoring for side effects, which are generally mild and include fatigue, headache, and soreness at the injection site. Staying hydrated and resting after vaccination can help alleviate discomfort. For parents vaccinating children, explaining the process in simple terms and offering distractions during the shot can ease anxiety. While mRNA vaccines are highly effective, they are not the only option; viral vector vaccines like AstraZeneca and Johnson & Johnson, as well as inactivated virus vaccines like Sinovac and Sinopharm, offer alternatives for those with specific preferences or contraindications.
In summary, Pfizer-BioNTech and Moderna’s mRNA vaccines exemplify the potential of this technology in combating infectious diseases. Their efficacy, adaptability, and rapid development highlight a new era in vaccinology, though they are not the sole tools in the fight against COVID-19. Understanding their unique features and practical considerations empowers individuals to make informed decisions about their health and contributes to broader public health goals.
Addressing Parental Concerns: Vaccination Safety for Children Explained
You may want to see also
Explore related products






![]()
Non-mRNA Vaccine Examples: AstraZeneca, Johnson & Johnson, Novavax, Sinovac
Not all COVID-19 vaccines rely on mRNA technology. Several widely used vaccines employ alternative methods to trigger an immune response, offering diverse options for global vaccination efforts. Among these are AstraZeneca, Johnson & Johnson, Novavax, and Sinovac, each utilizing distinct approaches to protect against the coronavirus.
AstraZeneca's vaccine, developed with the University of Oxford, uses a viral vector platform. It employs a modified chimpanzee adenovirus (ChAdOx1) to deliver genetic material encoding the SARS-CoV-2 spike protein into cells. This prompts the immune system to recognize and combat the virus. Administered in two doses, typically 8–12 weeks apart, it has been authorized for individuals aged 18 and above. Its storage requirements are less stringent than mRNA vaccines, making it a practical choice for many countries.
Johnson & Johnson’s vaccine also utilizes a viral vector, in this case, a human adenovirus (Ad26). Unlike AstraZeneca, it requires only a single dose, offering convenience and rapid immunity. Approved for adults aged 18 and older, it has been particularly useful in settings where administering two doses is challenging. However, rare cases of thrombosis with thrombocytopenia syndrome (TTS) have been reported, primarily in younger women, prompting careful consideration of its use in specific populations.
Novavax takes a protein subunit approach, using purified pieces of the coronavirus spike protein to stimulate an immune response. Administered in two doses, 3–8 weeks apart, it includes an adjuvant to enhance immune activation. This vaccine is suitable for individuals aged 12 and older and has been praised for its traditional technology, which may appeal to those hesitant about newer platforms like mRNA. Its efficacy and safety profile have made it a valuable addition to the global vaccine arsenal.
Sinovac’s CoronaVac is an inactivated virus vaccine, created by treating the SARS-CoV-2 virus with chemicals to render it non-infectious while preserving its ability to trigger immunity. Given in two doses, 2–4 weeks apart, it is authorized for individuals aged 3 and older in some countries. Its simplicity and established technology have made it a cornerstone of vaccination campaigns in many low- and middle-income nations. However, its efficacy varies, often requiring additional booster doses for sustained protection.
These non-mRNA vaccines demonstrate the diversity of scientific strategies employed to combat COVID-19. Each has unique advantages, from ease of storage to dosing schedules, ensuring that a broader range of populations can access protection. Understanding these options empowers individuals and policymakers to make informed decisions tailored to specific needs and circumstances.
Is Meningitis B Vaccine Live? Understanding Its Composition and Safety
You may want to see also
Explore related products






![]()
mRNA Vaccine Mechanism: Teaches cells to produce spike protein, triggering immune response
Not all coronavirus vaccines are mRNA-based, but those that are, such as Pfizer-BioNTech and Moderna, operate through a groundbreaking mechanism. Unlike traditional vaccines that introduce a weakened or inactivated virus, mRNA vaccines deliver genetic instructions to our cells. These instructions, encoded in messenger RNA (mRNA), teach cells to produce a harmless piece of the SARS-CoV-2 virus called the spike protein. This protein is crucial for the virus to enter human cells, making it an ideal target for the immune system.
The process begins with a tiny dose of mRNA, typically around 30 micrograms for the Pfizer vaccine and 100 micrograms for Moderna, encapsulated in lipid nanoparticles to protect it from degradation. Once injected into the muscle, these nanoparticles fuse with cell membranes, releasing the mRNA into the cytoplasm. Here, the mRNA hijacks the cell's protein-making machinery, specifically the ribosomes, to synthesize the spike protein. This production is transient, as the mRNA degrades within days, leaving no lasting genetic changes.
The newly synthesized spike proteins are displayed on the cell's surface, where they act as red flags for the immune system. Immune cells, such as dendritic cells, recognize these foreign proteins and present them to T cells and B cells, triggering a robust immune response. B cells produce antibodies that neutralize the spike protein, while T cells help by eliminating infected cells and coordinating the overall immune reaction. This dual-action prepares the body to fight off the actual virus if exposed.
One of the advantages of mRNA vaccines is their precision and adaptability. Since they only code for a single viral protein, they minimize the risk of adverse reactions compared to whole-virus vaccines. Additionally, the technology allows for rapid modification, as seen in the development of updated boosters targeting new variants. For instance, the bivalent boosters introduced in 2022 contain mRNA for both the original virus and the Omicron variant, broadening immune protection.
Practical considerations for mRNA vaccines include storage and administration. Pfizer’s vaccine requires ultra-cold storage (-70°C), though it can be stored in a refrigerator for up to 5 days before use. Moderna’s vaccine is more stable, needing -20°C storage but also allowing for refrigeration. Both vaccines are administered in a two-dose series, typically 3–4 weeks apart, with boosters recommended every 6–12 months depending on age and health status. For children aged 5–11, Pfizer offers a lower dose (10 micrograms) to balance efficacy and safety. Always consult healthcare providers for personalized advice, especially for individuals with allergies or compromised immune systems.
Hepatitis Vaccine: The 1984 Children's Story
You may want to see also
Explore related products






![]()
Global Vaccine Distribution: Mix of mRNA and non-mRNA vaccines used worldwide
The global fight against COVID-19 has relied on a diverse arsenal of vaccines, not just mRNA technology. While Pfizer-BioNTech and Moderna’s mRNA vaccines dominate headlines, they represent only a portion of the worldwide distribution. Over 13 billion doses have been administered globally, with non-mRNA vaccines like Oxford-AstraZeneca’s viral vector (ChAdOx1) and Sinopharm’s inactivated virus (BBIBP-CorV) playing critical roles, particularly in low- and middle-income countries. This mix reflects strategic choices driven by cost, storage requirements, and local manufacturing capabilities.
Consider the logistical advantages of non-mRNA vaccines. Viral vector vaccines, such as Johnson & Johnson’s single-dose offering, require standard refrigeration (2–8°C), making them ideal for regions with limited ultra-cold chain infrastructure. In contrast, mRNA vaccines demand stricter conditions—Pfizer’s must be stored at -70°C, though Moderna’s allows -20°C. Inactivated vaccines, like Sinovac’s CoronaVac, also use standard refrigeration, enabling broader accessibility in rural or resource-constrained areas. These differences have shaped distribution patterns, with mRNA vaccines predominantly used in high-income nations and non-mRNA alternatives filling gaps elsewhere.
Age-specific approvals further highlight the diversity in vaccine deployment. While Pfizer’s mRNA vaccine is authorized for children as young as 6 months in many countries, alternatives like Sinopharm’s inactivated vaccine are often the primary option for pediatric populations in Asia, Africa, and Latin America. For instance, China has administered over 3.4 billion doses, primarily BBIBP-CorV, to individuals aged 3 and older. Such variations underscore the importance of tailoring vaccine strategies to local contexts, including regulatory approvals, cultural acceptance, and healthcare infrastructure.
A persuasive argument for this mixed approach lies in its ability to address vaccine hesitancy and supply shortages. mRNA vaccines, though highly effective (95% efficacy in trials), faced skepticism in some regions due to their novel technology. Non-mRNA vaccines, with more established platforms, provided a familiar alternative. For example, India’s reliance on the Oxford-AstraZeneca vaccine (locally produced as Covishield) allowed it to administer over 2 billion doses, contributing significantly to global coverage. This blend of technologies ensured that no single supply disruption could derail vaccination efforts worldwide.
In practice, countries have adopted hybrid strategies, combining mRNA and non-mRNA vaccines to maximize reach and efficacy. Booster campaigns often mix technologies—a prime example is heterologous boosting, where an initial viral vector dose (e.g., AstraZeneca) is followed by an mRNA booster (e.g., Pfizer). Studies show this approach can enhance immune responses, offering flexibility in resource allocation. For individuals, understanding these options empowers informed decisions, particularly for those with allergies to mRNA components or living in areas with limited access to specific vaccines.
Ultimately, the global vaccine distribution landscape is a testament to innovation and adaptability. No single vaccine type fits all scenarios, and the coexistence of mRNA and non-mRNA technologies has been pivotal in combating the pandemic. As new variants emerge and vaccination efforts continue, this diversified approach remains a cornerstone of public health resilience.
Rite Aid's Vaccine Offerings: Types, Availability, and What You Need to Know
You may want to see also
Frequently asked questions
No, not all coronavirus vaccines are mRNA-based. While some, like Pfizer-BioNTech and Moderna, use mRNA technology, others, such as AstraZeneca, Johnson & Johnson, and Novavax, use different approaches like viral vectors or protein subunits.
mRNA vaccines (e.g., Pfizer and Moderna) deliver genetic instructions to cells to produce a harmless piece of the virus’s spike protein, triggering an immune response. Non-mRNA vaccines, like viral vector (Johnson & Johnson) or protein subunit (Novavax), use other methods to introduce the spike protein or its components to the immune system.
Availability of vaccine types varies by location and supply. In many places, you may have the option to choose, but it’s best to consult local health authorities or your healthcare provider for guidance on what’s available and recommended for you.
Both mRNA and non-mRNA vaccines have proven effective in preventing severe illness, hospitalization, and death from COVID-19. The effectiveness can vary slightly depending on the variant and individual factors, but all approved vaccines meet rigorous safety and efficacy standards.
No, mRNA vaccines do not alter your DNA. The mRNA never enters the cell’s nucleus, where DNA is stored. It simply provides temporary instructions for cells to produce the spike protein, which is then cleared from the body after triggering an immune response.