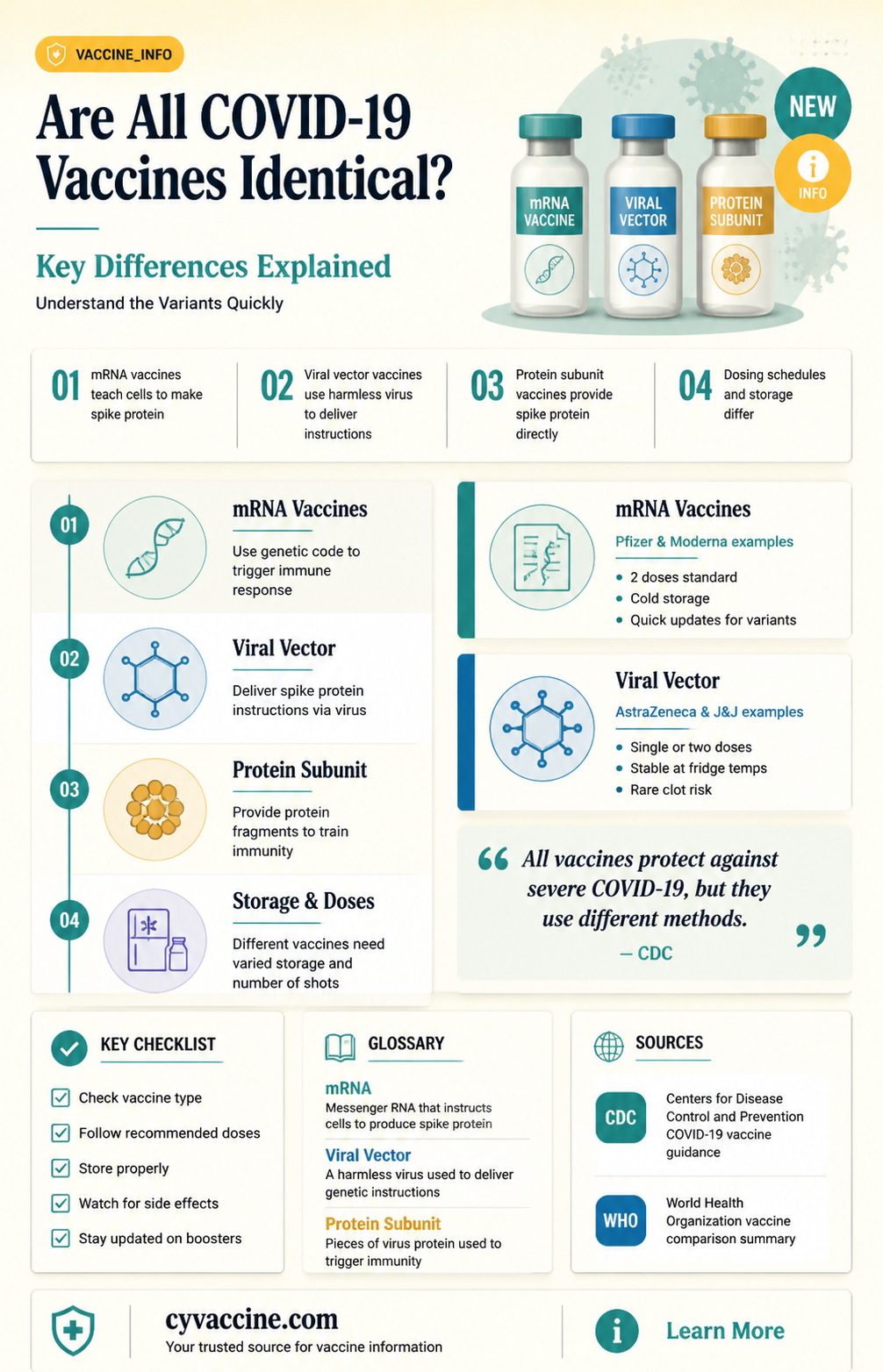
The question of whether all COVID-19 vaccines are the same is a common one, given the variety of vaccines developed and distributed globally. While all authorized vaccines aim to protect against COVID-19, they differ significantly in their technology, efficacy rates, dosage regimens, and side effects. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna use genetic material to instruct cells to produce a protein that triggers an immune response, whereas viral vector vaccines like AstraZeneca and Johnson & Johnson use a modified virus to deliver genetic instructions. Additionally, inactivated virus vaccines, such as Sinovac and Sinopharm, contain killed virus particles to stimulate immunity. These differences influence factors like storage requirements, administration schedules, and the types of immune responses generated, making it essential to understand that while all vaccines share the common goal of preventing severe illness, they are not identical in their mechanisms or outcomes.
| Characteristics | Values |
|---|---|
| Type of Vaccine | mRNA (Pfizer-BioNTech, Moderna), Viral Vector (AstraZeneca, Johnson & Johnson), Protein Subunit (Novavax), Inactivated Virus (Sinovac, Sinopharm) |
| Efficacy Against Symptomatic COVID-19 | Pfizer: 95%, Moderna: 94.1%, AstraZeneca: 70-82%, J&J: 66-72%, Novavax: 90.4%, Sinovac: 51-84%, Sinopharm: 78-86% |
| Dose Regimen | Pfizer: 2 doses (21 days apart), Moderna: 2 doses (28 days apart), AstraZeneca: 2 doses (4-12 weeks apart), J&J: Single dose, Novavax: 2 doses (3-8 weeks apart), Sinovac: 2 doses (2-4 weeks apart), Sinopharm: 2 doses (3-4 weeks apart) |
| Storage Requirements | Pfizer: -70°C (ultra-cold), Moderna: -20°C, AstraZeneca: 2-8°C, J&J: 2-8°C, Novavax: 2-8°C, Sinovac: 2-8°C, Sinopharm: 2-8°C |
| Technology | mRNA (Pfizer, Moderna), Adenovirus Vector (AstraZeneca, J&J), Recombinant Nanoparticle (Novavax), Inactivated Whole Virus (Sinovac, Sinopharm) |
| Common Side Effects | Pain at injection site, fatigue, headache, muscle pain, fever, chills (varies slightly by vaccine) |
| Approval Status | Pfizer, Moderna, AstraZeneca, J&J: Approved/Authorized in many countries including FDA, EMA, WHO. Novavax, Sinovac, Sinopharm: WHO Emergency Use Listing (EUL) |
| Booster Recommendations | Boosters recommended for most vaccines, especially mRNA types, to enhance immunity against variants like Omicron |
| Effectiveness Against Variants | Varies; mRNA vaccines show higher efficacy against variants like Delta and Omicron compared to viral vector and inactivated vaccines |
| Global Distribution | Pfizer and Moderna widely used in high-income countries, AstraZeneca and J&J in middle-income countries, Sinovac and Sinopharm predominantly in Asia, Africa, and Latin America |
| Cost | Varies by country and agreements; mRNA vaccines generally more expensive than viral vector and inactivated vaccines |
Explore related products

$11.93 $21.99





What You'll Learn
- Vaccine Types: mRNA, viral vector, protein subunit, and inactivated virus vaccines differ in technology
- Efficacy Rates: Vaccines vary in preventing infection, severe illness, and hospitalization
- Side Effects: Common side effects differ across vaccines, including pain, fever, and fatigue
- Dosage & Schedule: Number of doses and intervals vary between vaccine manufacturers
- Approval Status: Regulatory approvals and emergency use authorizations differ globally for each vaccine
![]()
Vaccine Types: mRNA, viral vector, protein subunit, and inactivated virus vaccines differ in technology
The COVID-19 pandemic spurred the development of multiple vaccine technologies, each with distinct mechanisms to trigger immunity. Understanding these differences is crucial for informed decision-making and addressing vaccine hesitancy. Four primary types emerged: mRNA, viral vector, protein subunit, and inactivated virus vaccines. Each harnesses unique biological processes to protect against SARS-CoV-2, offering varying advantages in efficacy, storage, and administration.
MRNA vaccines, such as Pfizer-BioNTech and Moderna, introduce genetic material encoding the virus’s spike protein into cells. These cells then produce the protein, prompting an immune response. Unlike traditional vaccines, mRNA does not alter DNA and degrades quickly after use. A standard regimen involves two doses, 3–4 weeks apart, with boosters recommended for sustained immunity. Storage requirements are stringent—Pfizer’s vaccine needs ultra-cold temperatures (–70°C), though Moderna’s is stable at –20°C. These vaccines boast high efficacy (90–95%) and are approved for individuals aged 5 and older, with pediatric doses adjusted for younger age groups.
Viral vector vaccines, exemplified by AstraZeneca and Johnson & Johnson, employ a harmless virus (e.g., adenovirus) to deliver spike protein genes into cells. Johnson & Johnson’s single-dose approach offers convenience, while AstraZeneca requires two doses. Efficacy ranges from 67% to 90%, depending on the study and variant. These vaccines are easier to store (2–8°C) and are widely used in low-resource settings. However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have limited their use in certain demographics, particularly younger adults.
Protein subunit vaccines, such as Novavax, contain lab-produced spike proteins directly injected into the body. This approach avoids genetic material or live viruses, making it suitable for those with mRNA or viral vector concerns. Novavax’s two-dose regimen (3 weeks apart) shows 90% efficacy and is stored at standard refrigeration temperatures. Its traditional technology may appeal to vaccine-hesitant individuals, though it has seen slower uptake compared to earlier vaccines.
Inactivated virus vaccines, like Sinovac and Sinopharm, use killed SARS-CoV-2 particles to stimulate immunity. This well-established method has been used for decades in vaccines such as those for polio and flu. A two-dose series (2–4 weeks apart) is typical, with boosters often recommended. Efficacy varies widely (50–80%) depending on the study and variant. These vaccines are stable at 2–8°C, making them accessible globally. However, their lower efficacy against certain variants has led to limited adoption in some regions.
Practical tips for vaccine selection include considering storage feasibility, dosing schedules, and individual health profiles. For instance, mRNA vaccines offer high efficacy but require careful storage, while viral vector vaccines provide single-dose convenience with easier storage. Protein subunit and inactivated virus vaccines cater to those preferring traditional technologies. Always consult healthcare providers to determine the best option based on age, health conditions, and local availability. Understanding these differences empowers individuals to make informed choices in the fight against COVID-19.
Update Your Vaccine Certificate: Steps to Change Mobile Number Easily
You may want to see also
Explore related products





![]()
Efficacy Rates: Vaccines vary in preventing infection, severe illness, and hospitalization
Not all COVID-19 vaccines are created equal, and their efficacy rates—their ability to prevent infection, severe illness, and hospitalization—vary significantly. For instance, the Pfizer-BioNTech mRNA vaccine demonstrated 95% efficacy in preventing symptomatic COVID-19 in clinical trials, while the Oxford-AstraZeneca viral vector vaccine showed around 70% efficacy. These differences stem from factors like vaccine technology, dosage regimens, and the populations studied. Understanding these variations is crucial for informed decision-making, especially as new variants emerge and booster strategies evolve.
Consider the practical implications of these efficacy rates. A vaccine with higher efficacy against infection, like Moderna’s 94% rate, may reduce community transmission more effectively, but even vaccines with lower infection prevention rates, such as Johnson & Johnson’s 66%, still offer robust protection against severe illness and hospitalization—often above 85%. For example, a single dose of Johnson & Johnson provides convenience for hard-to-reach populations, while Pfizer’s two-dose regimen (30 µg each) requires more logistical planning but offers stronger initial immunity. Tailoring vaccine choice to individual needs—age, health status, and exposure risk—maximizes protection.
Age plays a critical role in vaccine efficacy. Studies show that older adults, particularly those over 65, may experience lower efficacy rates due to age-related immune decline. For instance, Pfizer’s vaccine efficacy in this group drops to around 94% for severe disease but remains highly effective at preventing hospitalization. In contrast, younger populations, such as adolescents (12–15 years), exhibit even higher efficacy rates, nearing 100% in some trials. This underscores the importance of age-specific recommendations, such as booster doses for seniors or adjusted dosing for children, to ensure optimal protection across demographics.
When comparing vaccines, it’s essential to interpret efficacy data in context. Real-world effectiveness often differs from clinical trial results due to factors like variant circulation and waning immunity. For example, while Pfizer and Moderna initially boasted higher efficacy, their protection against infection declined over time, necessitating boosters. Meanwhile, vaccines like Novavax, a protein subunit vaccine with 90% efficacy, offer an alternative for those hesitant about mRNA technology. Practical tips include staying updated on booster recommendations, monitoring local variant prevalence, and consulting healthcare providers to choose the best vaccine for your circumstances.
Ultimately, the goal of vaccination is to prevent severe outcomes, and all authorized COVID-19 vaccines excel in this regard. While efficacy rates vary, the collective impact of vaccination programs has been profound, reducing hospitalizations and deaths globally. For instance, countries with high vaccination rates, such as Israel and Singapore, have seen dramatic declines in severe cases despite variant surges. By focusing on the shared objective of protection rather than minor efficacy differences, individuals can make informed choices that contribute to both personal and public health.
Hepatitis A and C Vaccines: Availability, Protection, and Prevention Explained
You may want to see also
Explore related products






![]()
Side Effects: Common side effects differ across vaccines, including pain, fever, and fatigue
Not all COVID-19 vaccines are created equal, and this becomes particularly evident when examining their side effects. While the primary goal of any vaccine is to trigger an immune response, the journey to protection can vary significantly depending on the type of vaccine administered. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines often report higher rates of fatigue and fever after the second dose, with some individuals experiencing chills and muscle pain. These symptoms typically peak within 24–48 hours post-vaccination and resolve within a few days. In contrast, the Johnson & Johnson viral vector vaccine is more frequently associated with injection site pain and headaches, though systemic reactions like fever are less common. Understanding these differences can help individuals prepare for what to expect and manage symptoms effectively.
From an analytical perspective, the variation in side effects can be attributed to the distinct mechanisms of action of each vaccine. mRNA vaccines, like Pfizer and Moderna, deliver genetic material that instructs cells to produce a harmless piece of the SARS-CoV-2 spike protein, prompting a robust immune response. This process can lead to more pronounced systemic reactions, such as fever and fatigue, as the body works to build immunity. On the other hand, the Johnson & Johnson vaccine uses a modified adenovirus to deliver the spike protein gene, which may elicit a milder systemic response but more localized reactions, such as arm soreness. These differences highlight the importance of considering individual health profiles when choosing a vaccine, particularly for those with specific sensitivities or medical conditions.
For those preparing to receive a COVID-19 vaccine, practical tips can make the experience more manageable. If you’re scheduled for an mRNA vaccine, plan for potential downtime after the second dose, especially if you’re in a younger age group (16–55), as this demographic tends to report stronger side effects. Stock up on over-the-counter pain relievers like acetaminophen or ibuprofen, but avoid taking them preemptively unless advised by a healthcare provider, as they may interfere with the immune response. Stay hydrated and dress in loose clothing to minimize discomfort at the injection site. For Johnson & Johnson recipients, focus on managing localized pain with cold compresses and gentle arm exercises to improve circulation.
A comparative analysis reveals that while side effects differ, they are generally mild to moderate and short-lived across all vaccines. For example, a study published in *JAMA* found that while 75% of mRNA vaccine recipients reported fatigue, only 35% of Johnson & Johnson recipients experienced the same. However, the Johnson & Johnson vaccine was associated with a higher incidence of nausea (26%) compared to Moderna (16%). These statistics underscore the importance of weighing individual tolerances and preferences when selecting a vaccine. It’s also worth noting that rare but serious side effects, such as blood clots or anaphylaxis, are not correlated with common side effects like pain or fever, and their occurrence is extremely low across all vaccines.
In conclusion, while all COVID-19 vaccines share the common goal of preventing severe illness, their side effect profiles differ in meaningful ways. By understanding these variations, individuals can better prepare for their vaccination experience and take proactive steps to manage symptoms. Whether it’s scheduling rest after an mRNA vaccine or focusing on local pain relief for a viral vector vaccine, being informed empowers individuals to approach vaccination with confidence. Ultimately, the transient nature of these side effects pales in comparison to the long-term protection they provide against a potentially life-threatening virus.
Understanding Prevnar 20: Benefits, Uses, and Importance of the Vaccine
You may want to see also
Explore related products






![]()
Dosage & Schedule: Number of doses and intervals vary between vaccine manufacturers
The COVID-19 vaccines are not one-size-fits-all, and this is particularly evident when examining their dosage and administration schedules. Each vaccine manufacturer has developed a unique regimen, tailored to their specific vaccine technology and clinical trial data. For instance, the Pfizer-BioNTech vaccine requires two doses, administered 3 to 4 weeks apart for individuals aged 16 and above, while the interval can be extended up to 6 weeks in some countries. In contrast, the Moderna vaccine follows a similar two-dose regimen but with a recommended interval of 4 weeks, and in some cases, up to 6 weeks.
A notable exception is the Johnson & Johnson (Janssen) vaccine, which is a single-dose vaccine for individuals aged 18 and above. This vaccine utilizes a different technology, employing a modified adenovirus vector, which allows for a robust immune response after just one dose. The AstraZeneca vaccine, also using adenovirus vector technology, typically requires two doses, with an interval of 4 to 12 weeks, depending on local guidelines and the specific population being vaccinated. These variations in dosage and schedule are not arbitrary; they are based on extensive clinical trials and ongoing real-world data, ensuring optimal immune response and safety.
For parents and caregivers, it's essential to note that vaccine schedules for children and adolescents may differ. The Pfizer-BioNTech vaccine is authorized for individuals aged 5 and above, with a lower dosage (10 μg) for children aged 5-11, compared to the 30 μg dose for those aged 12 and above. The two-dose regimen remains consistent, but the interval may be adjusted based on local health authority recommendations. This tailored approach ensures that the vaccine is both effective and safe for different age groups.
In practical terms, these varying schedules can impact vaccination campaigns and individual planning. For instance, a person opting for the Johnson & Johnson vaccine may complete their vaccination course in a single visit, whereas those choosing mRNA vaccines like Pfizer or Moderna will need to schedule a second appointment. It's crucial to follow the recommended intervals, as deviating from the prescribed schedule may affect the vaccine's efficacy. Additionally, some countries offer flexibility in mixing and matching vaccines, especially in cases where the initial vaccine type is unavailable for the second dose. However, this should only be done under the guidance of healthcare professionals, considering the latest scientific evidence.
The diversity in dosage and schedules highlights the complexity of vaccine development and the need for personalized approaches in public health. As more vaccines become available and research progresses, these regimens may be further refined. For now, understanding these differences is key to making informed decisions and ensuring successful vaccination outcomes. This knowledge empowers individuals to actively participate in their healthcare and contributes to the overall success of global vaccination efforts.
Why California Doctors Charge for Vaccination Records: Explained
You may want to see also
Explore related products






![]()
Approval Status: Regulatory approvals and emergency use authorizations differ globally for each vaccine
Regulatory approvals and emergency use authorizations for COVID-19 vaccines vary widely across countries, creating a complex landscape for global vaccination efforts. For instance, the Pfizer-BioNTech vaccine received full approval from the U.S. FDA for individuals aged 16 and older, while maintaining emergency use authorization (EUA) for those aged 5–15. In contrast, the European Medicines Agency (EMA) approved it for ages 12 and up, with some countries like Germany offering it to children as young as 5 under specific conditions. These discrepancies highlight how age categories and approval types differ even among closely aligned regulatory bodies.
Consider the AstraZeneca vaccine, which exemplifies how geopolitical factors influence approval status. While the EMA and the UK’s MHRA granted full approval for adults, the U.S. FDA has yet to authorize it, citing the need for additional data. Meanwhile, many African and Asian countries have embraced it as a cost-effective option, often administered in a two-dose regimen with an 8–12 week interval. This vaccine’s global rollout underscores how local regulatory priorities and resource availability shape its acceptance and distribution.
Emergency use authorizations (EUAs) have been a critical tool for accelerating vaccine access, but their criteria and timelines vary significantly. For example, India’s Bharat Biotech developed Covaxin, which received EUA in India in January 2021 but was not approved by the WHO until November 2021. This delay impacted its acceptance in international travel and global vaccine-sharing programs. Similarly, China’s Sinovac and Sinopharm vaccines have been widely used in Latin America and the Middle East under EUAs, despite limited data transparency initially slowing WHO endorsement.
Practical tips for navigating this fragmented approval landscape include verifying vaccine recognition for international travel, as some countries only accept specific vaccines or require additional doses. For instance, the EU’s Digital COVID Certificate accepts WHO-approved vaccines, but individual member states may impose stricter rules. Additionally, travelers should check if their vaccine’s EUA status affects entry requirements, as seen with countries differentiating between fully approved and emergency-authorized vaccines. Staying informed through official health agency websites is essential to avoid travel disruptions.
In conclusion, the global patchwork of regulatory approvals and EUAs for COVID-19 vaccines demands careful attention to detail. From age-specific authorizations to geopolitical influences, these variations impact vaccine accessibility, distribution, and acceptance. Understanding these differences empowers individuals and policymakers to make informed decisions, ensuring equitable and effective vaccination strategies worldwide.
Did Robert Malone Invent mRNA Vaccines? Unraveling the Truth
You may want to see also
Frequently asked questions
No, COVID-19 vaccines use different technologies, including mRNA (e.g., Pfizer-BioNTech, Moderna), viral vector (e.g., Johnson & Johnson, AstraZeneca), and protein subunit (e.g., Novavax) approaches.
While all approved vaccines are effective at preventing severe illness, hospitalization, and death, their efficacy rates vary. For example, mRNA vaccines generally have higher efficacy rates compared to some viral vector vaccines.
No, side effects differ depending on the vaccine type. Common side effects like fatigue, headache, and soreness are similar, but specific reactions (e.g., rare blood clots with viral vector vaccines) vary.
Yes, in many countries, mixing and matching vaccines (e.g., receiving one dose of AstraZeneca and another of Pfizer) is allowed and has been shown to be safe and effective in some cases.
No, vaccine availability varies by region due to factors like production capacity, distribution challenges, and funding disparities, leading to unequal access in low-income countries.