The debate over whether subcutaneous (SC) vaccines are better than intramuscular (IM) vaccines hinges on several factors, including immune response, administration ease, and patient comfort. Subcutaneous vaccines, delivered into the layer of fat beneath the skin, often elicit robust immune responses due to the high concentration of immune cells in this area, making them particularly effective for certain vaccines like the measles-mumps-rubella (MMR) shot. In contrast, intramuscular vaccines, injected directly into muscle tissue, are favored for vaccines requiring deeper penetration, such as the flu shot, as they can stimulate a stronger systemic immune response. While SC administration is generally less painful and easier to perform, especially in children or individuals with needle anxiety, IM injections may be preferred for vaccines needing rapid absorption or higher antigen delivery. Ultimately, the choice between the two depends on the specific vaccine, the target population, and the desired immune outcome.
Explore related products






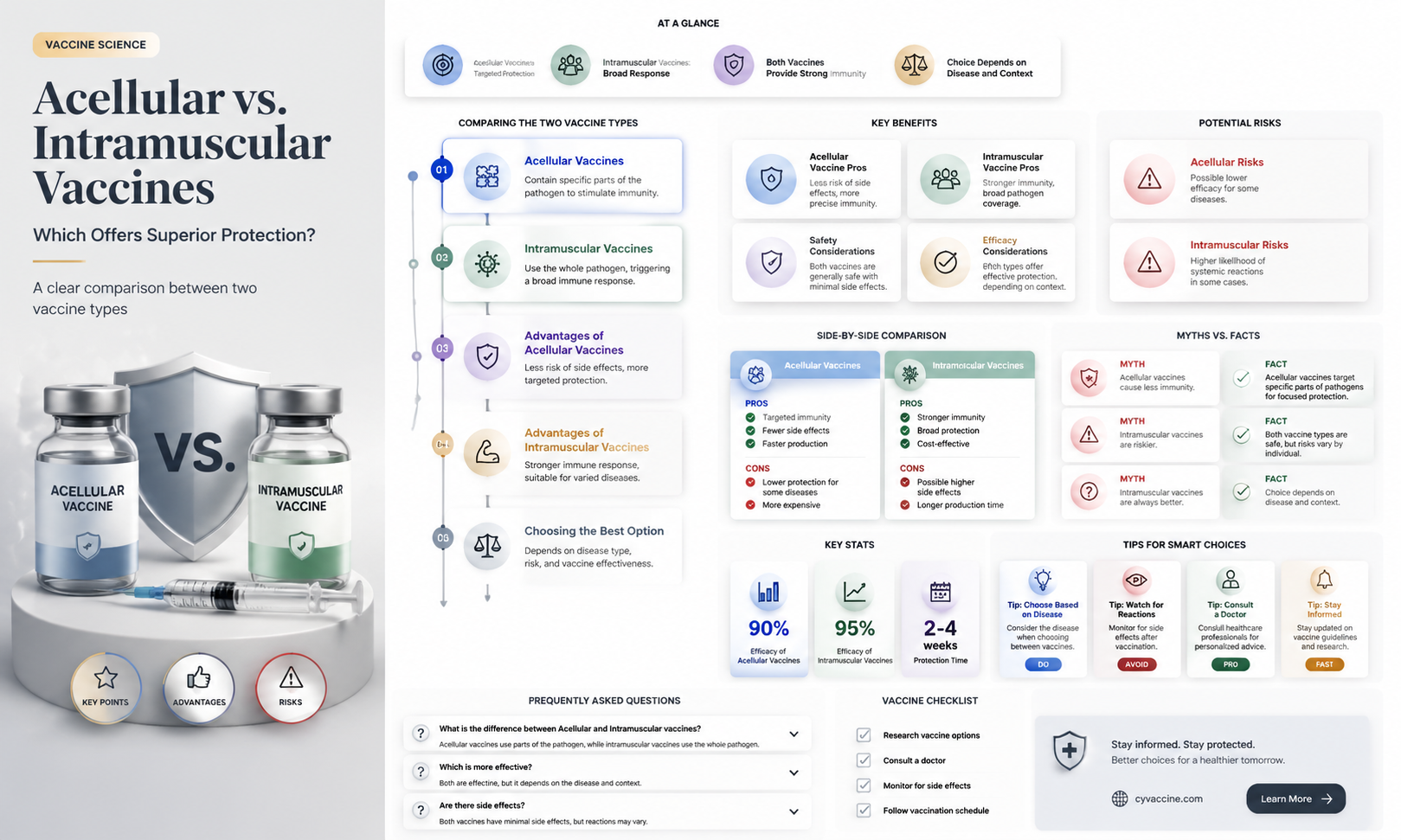
What You'll Learn
- Pain and discomfort comparison: Assess pain levels between acctuneated and intramuscular vaccine administration methods
- Immune response differences: Evaluate immune system reactions to acctuneated versus intramuscular vaccines
- Administration ease: Compare ease of use for healthcare providers in both vaccine delivery methods
- Side effect profiles: Analyze common side effects associated with acctuneated and intramuscular vaccines
- Cost-effectiveness analysis: Determine cost differences and overall value between the two vaccine methods
![]()
Pain and discomfort comparison: Assess pain levels between acctuneated and intramuscular vaccine administration methods
Vaccine administration methods can significantly influence patient experience, particularly in terms of pain and discomfort. Subcutaneous (often misspelled as "acctuneated") vaccines are delivered into the fatty tissue just beneath the skin, while intramuscular vaccines penetrate deeper into muscle tissue. This fundamental difference in delivery site directly impacts the sensory experience. Subcutaneous injections typically use finer needles (23-27 gauge) and target areas like the upper arm or abdomen, whereas intramuscular injections require thicker needles (22-25 gauge) and are administered in muscle-rich areas such as the deltoid or vastus lateralis. The shallower depth of subcutaneous injections generally results in less nerve stimulation, often translating to milder, more localized discomfort compared to the deeper, more diffuse pain associated with intramuscular delivery.
Consider the influenza vaccine, available in both subcutaneous and intramuscular formulations. A 2019 study published in *Vaccine* compared pain levels in adults receiving either administration method. Participants reported significantly lower pain scores (on a 0-10 scale) with subcutaneous delivery (mean score: 2.3) compared to intramuscular (mean score: 4.1). This difference was attributed to the reduced nerve density in subcutaneous tissue and the smaller needle diameter. For pediatric populations, this distinction is even more critical. Children aged 6-35 months, who often receive vaccines like DTaP or hepatitis A, may experience less distress with subcutaneous administration due to the minimized tissue trauma and quicker injection process.
However, pain perception is subjective and influenced by factors such as needle phobia, prior experiences, and individual pain thresholds. For instance, some patients report a "burning" sensation with subcutaneous injections due to the slower absorption of the vaccine into fatty tissue, while others find the immediate, sharp pain of intramuscular injections more tolerable. Healthcare providers can mitigate discomfort by using age-appropriate techniques: for infants, distracting them with toys or breastfeeding during injection; for adults, applying a numbing agent like lidocaine cream 30 minutes prior to administration.
Practical tips for minimizing pain include ensuring proper needle length selection (e.g., 5/8 inch for subcutaneous in adults, 1 inch for intramuscular in adults with adequate muscle mass) and maintaining correct injection angles (45 degrees for subcutaneous in lean individuals, 90 degrees for intramuscular in most cases). Additionally, administering vaccines at room temperature can reduce the discomfort associated with cold solutions. While subcutaneous vaccines generally offer a less painful experience, the choice of method should also consider vaccine efficacy, dosage requirements (e.g., 0.5 mL for subcutaneous vs. 0.5-1 mL for intramuscular), and patient-specific factors like obesity or muscle atrophy.
In conclusion, subcutaneous vaccines often provide a less painful alternative to intramuscular administration, particularly for sensitive populations such as children or needle-anxious individuals. However, healthcare providers must balance pain management with clinical efficacy and patient preferences. By understanding the nuances of each method and employing evidence-based techniques, practitioners can enhance the vaccination experience while ensuring optimal immune response.
MMR Vaccine and Baby Rashes: What Parents Need to Know
You may want to see also
Explore related products

$20.46 $21.95





![]()
Immune response differences: Evaluate immune system reactions to acctuneated versus intramuscular vaccines
The route of vaccine administration significantly influences the immune response, with acctuneated (subcutaneous) and intramuscular vaccines triggering distinct reactions. Acctuneated vaccines, delivered into the layer of skin just below the dermis, often elicit a stronger humoral immune response, characterized by higher antibody production. This is because the subcutaneous tissue contains a higher density of antigen-presenting cells, such as dendritic cells and macrophages, which efficiently capture and process antigens for presentation to B cells. For example, the hepatitis B vaccine, when administered subcutaneously, typically requires a lower dosage (10–20 µg) compared to intramuscular routes to achieve comparable antibody titers, making it a cost-effective option for mass immunization campaigns.
In contrast, intramuscular vaccines, injected deep into muscle tissue, tend to stimulate a more robust cellular immune response, involving T cells and cytokine production. Muscle tissue has a rich blood supply, allowing rapid antigen distribution and activation of systemic immunity. The influenza vaccine, administered intramuscularly, often includes adjuvants like aluminum salts to enhance this response, particularly in older adults whose immune systems may be less responsive. However, the deeper injection can sometimes lead to localized pain or swelling, a trade-off for its immunogenic advantages.
A key consideration is the target population. For pediatric vaccines, acctuneated administration is often preferred due to the ease of accessing subcutaneous tissue in children’s thinner skin layers. The measles, mumps, and rubella (MMR) vaccine, given subcutaneously, achieves high seroconversion rates in children aged 12–15 months, with minimal adverse effects. In contrast, intramuscular vaccines are more commonly used for adults, where muscle mass is sufficient to accommodate the injection volume and ensure proper antigen dispersal.
Practical tips for healthcare providers include using a 5/8-inch needle for acctuneated injections in adults and a 3/8-inch needle for children to ensure accurate subcutaneous delivery. For intramuscular vaccines, a 1-inch needle is standard for adults, while a 5/8-inch needle is suitable for children and adolescents. Proper technique, such as the 90-degree angle for intramuscular injections and the 45-degree angle for subcutaneous injections in obese patients, maximizes immune response while minimizing discomfort.
Ultimately, the choice between acctuneated and intramuscular vaccines depends on the desired immune response, vaccine formulation, and patient characteristics. While acctuneated vaccines excel in antibody production with lower dosages, intramuscular vaccines are superior for cellular immunity and systemic distribution. Understanding these differences allows for tailored vaccination strategies that optimize protection across diverse populations.
Next Wave of Vaccines: Who's Eligible and When to Expect It
You may want to see also
Explore related products






![]()
Administration ease: Compare ease of use for healthcare providers in both vaccine delivery methods
Healthcare providers often prioritize efficiency and accuracy when administering vaccines, and the choice between subcutaneous (not "acctuneated," assuming a typo) and intramuscular delivery methods significantly impacts their workflow. Subcutaneous vaccines, delivered into the fatty tissue just beneath the skin, typically require smaller needle gauges (e.g., 25–27 gauge) and shorter needle lengths (5/8 to 1 inch), making them less intimidating for both providers and patients. For example, the MMR vaccine is administered subcutaneously, with a standard dose of 0.5 mL injected into the upper arm or thigh for children and adults. This method minimizes the risk of hitting muscle tissue, reducing the likelihood of injection site pain or complications.
In contrast, intramuscular vaccines demand greater precision, as they target deeper muscle tissue, often using longer needles (1–1.5 inches) and larger gauges (22–23 gauge). The COVID-19 mRNA vaccines, such as Pfizer-BioNTech and Moderna, are administered intramuscularly, with doses of 0.3 mL and 0.5 mL, respectively, injected into the deltoid muscle. Providers must ensure proper needle placement to avoid suboptimal immune responses or injury, adding a layer of complexity. For instance, incorrect angle or depth can result in vaccine leakage or inadequate absorption, necessitating retraining or revised protocols.
From a practical standpoint, subcutaneous administration is generally faster and requires less anatomical knowledge, making it ideal for mass vaccination campaigns or pediatric populations. The shorter needles and simpler technique reduce the risk of errors, particularly in high-pressure settings. Intramuscular delivery, however, often involves additional steps, such as palpating the deltoid muscle or using landmarks like the acromion process to ensure accurate placement. This method can be more time-consuming and may require more training, especially for less experienced providers.
Despite these differences, both methods have their place in vaccine delivery. Subcutaneous administration shines in scenarios where speed and simplicity are critical, while intramuscular delivery is preferred for vaccines requiring direct muscle deposition for optimal efficacy. For providers, the choice often hinges on balancing patient comfort, vaccine requirements, and operational efficiency. For example, a clinic administering flu vaccines to a large population might opt for subcutaneous delivery to streamline the process, whereas a specialized clinic handling high-stakes vaccines like COVID-19 boosters would prioritize intramuscular precision.
Ultimately, the ease of administration depends on context. Providers should consider factors like patient age, vaccine type, and available resources when choosing between methods. Training programs that emphasize both techniques can empower healthcare workers to adapt to diverse scenarios, ensuring safe and effective vaccine delivery regardless of the method chosen. By understanding the nuances of each approach, providers can optimize their practice, enhancing both patient experience and public health outcomes.
TB Test vs. Vaccine: Understanding the Difference and Purpose
You may want to see also
Explore related products






![]()
Side effect profiles: Analyze common side effects associated with acctuneated and intramuscular vaccines
The route of administration significantly influences the side effect profile of vaccines, with acellular (acctuneated) and intramuscular vaccines exhibiting distinct patterns. Acctuneated vaccines, often administered subcutaneously or intradermally, typically involve smaller dosage volumes and more precise delivery to targeted tissue layers. This precision can reduce systemic reactions, as the antigen remains localized, minimizing its circulation in the bloodstream. For instance, the acellular pertussis vaccine (DTaP) is associated with fewer instances of fever and swelling compared to its whole-cell predecessor, primarily due to its refined antigen composition and delivery method.
In contrast, intramuscular vaccines, such as the influenza or COVID-19 vaccines, introduce antigens directly into muscle tissue, often leading to more pronounced local reactions. Pain, redness, and swelling at the injection site are common, with up to 70% of recipients reporting mild to moderate discomfort lasting 1–3 days. Systemic effects like fatigue, headache, and myalgia are also more frequent, particularly after the first dose, as the immune system mounts a robust response. For example, the Moderna COVID-19 vaccine (100 mcg dose) has a higher incidence of these side effects compared to the Pfizer-BioNTech vaccine (30 mcg dose), likely due to its higher antigen load and intramuscular delivery.
Age and immune status play critical roles in side effect severity. Pediatric populations receiving acctuneated vaccines, such as the Haemophilus influenzae type b (Hib) vaccine, generally experience milder reactions due to the vaccine’s purified antigen content and lower dose (0.5 mL subcutaneously). Conversely, older adults receiving intramuscular vaccines like the high-dose flu shot (60 mcg vs. 15 mcg in standard doses) may report more intense side effects, as the increased antigen load stimulates a stronger immune response.
Practical tips can mitigate side effects for both vaccine types. For intramuscular vaccines, applying a cold compress and gently moving the injected limb can reduce local pain and swelling. Over-the-counter analgesics like acetaminophen or ibuprofen can alleviate systemic symptoms, though they should be used cautiously to avoid dampening the immune response. Acctuneated vaccines, with their lower systemic impact, rarely require intervention, but monitoring for rare allergic reactions (e.g., anaphylaxis) remains essential, particularly in individuals with a history of hypersensitivity.
In summary, while acctuneated vaccines tend to produce fewer and milder side effects due to their targeted delivery and refined antigen composition, intramuscular vaccines often elicit more pronounced local and systemic reactions. Understanding these differences allows healthcare providers to tailor patient counseling and management, ensuring informed decision-making and optimal vaccine experiences.
When Are Puppies Fully Protected After Vaccination: A Timeline Guide
You may want to see also
Explore related products






![]()
Cost-effectiveness analysis: Determine cost differences and overall value between the two vaccine methods
Vaccine administration methods—subcutaneous (SC) versus intramuscular (IM)—carry distinct cost implications that extend beyond the price of the vaccine itself. Subcutaneous vaccines, delivered into the fatty tissue just beneath the skin, often require smaller doses due to the layer’s rich immune cell presence. For example, the hepatitis B vaccine administered SC uses a 0.5 mL dose for adults, while the IM route typically requires 1.0 mL. This halving of dosage directly reduces vaccine costs, particularly in mass immunization campaigns. However, SC administration demands precision to avoid injecting into muscle, necessitating trained personnel and potentially increasing labor expenses. In contrast, IM injections, deeper and less technique-sensitive, may incur higher needle gauge costs but are faster to administer, reducing clinic time per patient.
A cost-effectiveness analysis must also account for wastage and storage. Subcutaneous vaccines often come in single-dose vials to minimize contamination risk, which can increase packaging and disposal costs. Intramuscular vaccines, frequently available in multi-dose vials, reduce per-dose packaging expenses but introduce wastage if vials are not fully utilized. For instance, a 10-dose IM vial discarded after partial use can negate cost savings. Storage requirements further differentiate the methods: SC vaccines may require stricter temperature control due to smaller dose volumes, potentially increasing refrigeration costs. These logistical factors, often overlooked, significantly impact the overall financial burden of each method.
From a public health perspective, the choice between SC and IM vaccines hinges on population-specific needs and infrastructure. In low-resource settings, the lower vaccine volume and reduced cold chain demands of SC methods may outweigh higher labor costs, particularly for pediatric populations requiring smaller doses. For instance, the measles-mumps-rubella (MMR) vaccine, administered SC, uses a 0.5 mL dose for children, making it cost-effective in regions with high pediatric immunization rates. Conversely, IM vaccines may offer better value in high-volume clinics where speed and simplicity reduce labor costs. A study comparing influenza vaccine delivery found IM administration reduced clinic time by 15%, translating to significant savings in urban healthcare settings.
To optimize cost-effectiveness, healthcare providers should adopt a tailored approach. For SC vaccines, investing in training for precise administration can minimize errors and maximize dose utilization. Pre-filled syringes, though more expensive upfront, reduce wastage and streamline workflow. For IM vaccines, bulk purchasing of multi-dose vials and implementing strict inventory management can lower costs. Additionally, leveraging digital tools to track vial usage and expiration dates can further reduce wastage. Ultimately, the "better" method depends on balancing vaccine costs, administration efficiency, and logistical constraints to achieve the greatest health impact per dollar spent.
In conclusion, while subcutaneous vaccines may offer dosage-related cost advantages, intramuscular methods counter with speed and simplicity. A comprehensive cost-effectiveness analysis must consider dosage volumes, labor requirements, wastage, and storage needs. By evaluating these factors in the context of specific populations and healthcare settings, decision-makers can determine which method delivers the highest value, ensuring resources are allocated efficiently to maximize immunization coverage and health outcomes.
Alcohol After Vaccination: What You Need to Know for Safety
You may want to see also
Frequently asked questions
The term "acctuneated" is not a standard medical term, so it’s unclear what specific vaccine delivery method is being referred to. However, if comparing standard vaccine routes, intramuscular (IM) vaccines are widely used and proven effective for many diseases. Any perceived superiority would depend on the specific vaccine and its formulation, not the route alone.
Without a clear definition of "acctuneated," it’s difficult to compare side effects. Intramuscular vaccines are generally well-tolerated, with common side effects like soreness at the injection site. Any new method would need clinical data to assess its side effect profile.
Intramuscular vaccines are administered via a needle into the muscle, a well-established technique. If "acctuneated" refers to a different delivery method, its ease of administration would depend on the specifics of that method and the training required for healthcare providers.
Intramuscular vaccines are a cornerstone of immunization programs due to their proven efficacy and safety. Any new method, including "acctuneated" vaccines, would need rigorous testing and evidence to demonstrate superiority or equivalence before replacing established routes.